0441
The value of diffusion-relaxation correlation spectrum imaging in differential diagnosis of early and advanced squamous cervical carcinoma1Northern Jiangsu People's Hospital, Yangzhou, Jiangsu Province, China, 2MR Collaboration, Central Research Institute, United Imaging Healthcare, Shanghai, China, Shanghai, China
Synopsis
Keywords: Uterus, Microstructure, multi dimension
Accurately staging squamous cell carcinoma (SCC) is of vital importance for determining the treatment plan, prognosis and outcome. Diffusion-relaxation correlation spectrum imaging (DR-CSI) can jointly encode diffusion and relaxation information and resolve information of tissue compartments and heterogeneity at a sub-voxel level. In this study we investigated the feasibility of DR-CSI in characterizing tissue microenvironment and staging SCC. The DR-CSI technique can non-invasively provide information on microscopic tissue compartments within voxels, reflecting intra-tissue heterogeneity. The diagnostic performance of DR-CSI in identifying early and advanced SCC was significantly superior to conventional ADC and T2.Introduction
Cervical carcinoma is the fourth most common carcinoma among women in the world, ranking second in low- and middle-income countries, among which, the most common type is squamous cell carcinoma (SCC)1,2. The stage diagnosis of SCC is an important factor to determine the treatment plan and to predict prognosis and outcome1. Diffusion-weighted imaging (DWI) and T2-weighted imaging (T2WI) have shown potential in staging SCC3,4. However, conventional apparent diffusion coefficient (ADC) and T2 values are averages for a single voxel, which may limit their ability in reflecting the underlying complex microstructure. Diffusion-relaxation correlation spectrum imaging (DR-CSI) can jointly encode diffusion and relaxation information and resolve information of tissue compartments and heterogeneity at a sub-voxel level5. Thus the aim of this study was to investigate the feasibility of DR-CSI in characterizing tissue microenvironment and identifying the early and advanced stage cervical carcinoma.Methods
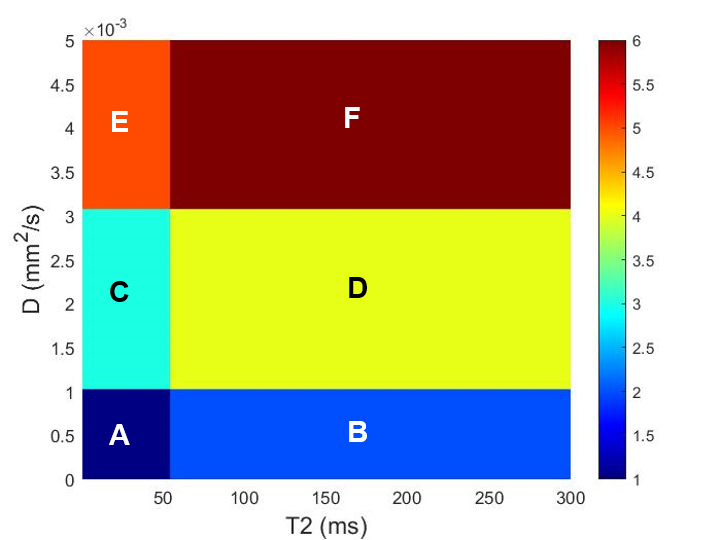
Totally twenty-one patients with histopathologically proven SCC (10 early stage and 11 advanced stage, according to FIGO 2018 staging criteria) underwent preoperative MRI examination on a 3.0T scanner (uMR 790, United Imaging Healthcare, Shanghai, China). DR-CSI data was acquired with the single-shot spin-echo echo planar imaging sequence using a combination of five echo times (47.6, 60, 70, 80, 90ms) and six b values (0, 200, 400, 800, 1200, 1600mm2/s).The regions of interest (ROIs) were delineated on the slice with the largest tumor size to cover the solid part and exclude the necrotic area. DR-CSI modeled the MRI signal at each voxel as a summation of continuous exponential decay functions characterized by transverse relaxation time (T2) and diffusion coefficient (D)6. T2-D spectrum of each voxel was constructed using every combination of 40 D values (distributed from 0.001 to 5×10-3mm2/s) and 40 T2 values (distributed from 0 to 300ms) by applying the non-negativity and spatial total variation constraints. It was further segmented into six compartments with cut-off values of ADC: 1×10-3mm2/s, 3×10-3mm2/s and T2: 50ms (Fig.1). The compartmental fractions (fA, fB, fC, fD, fE and fF) for ROIs were calculated by normalizing for the integration of each compartmental voxel-wise spectra. The mean ADC, T2 values of ROIs were also measured.
ADC, T2 values and compartmental fractions (fA, fB, fC, fD, fE and fF)were compared with independent sample t-test or Mann-Whitney U test. Binary Logistic regression analysis was used for multi-parameter joint analysis and receiver operating characteristics (ROC) analysis were used to evaluate the diagnostic efficiency of each parameter and their combinations in distinguishing the early from advanced SCC. Delong test was used to compare the significant differences between AUCs of each parameter and their combinations.
Results
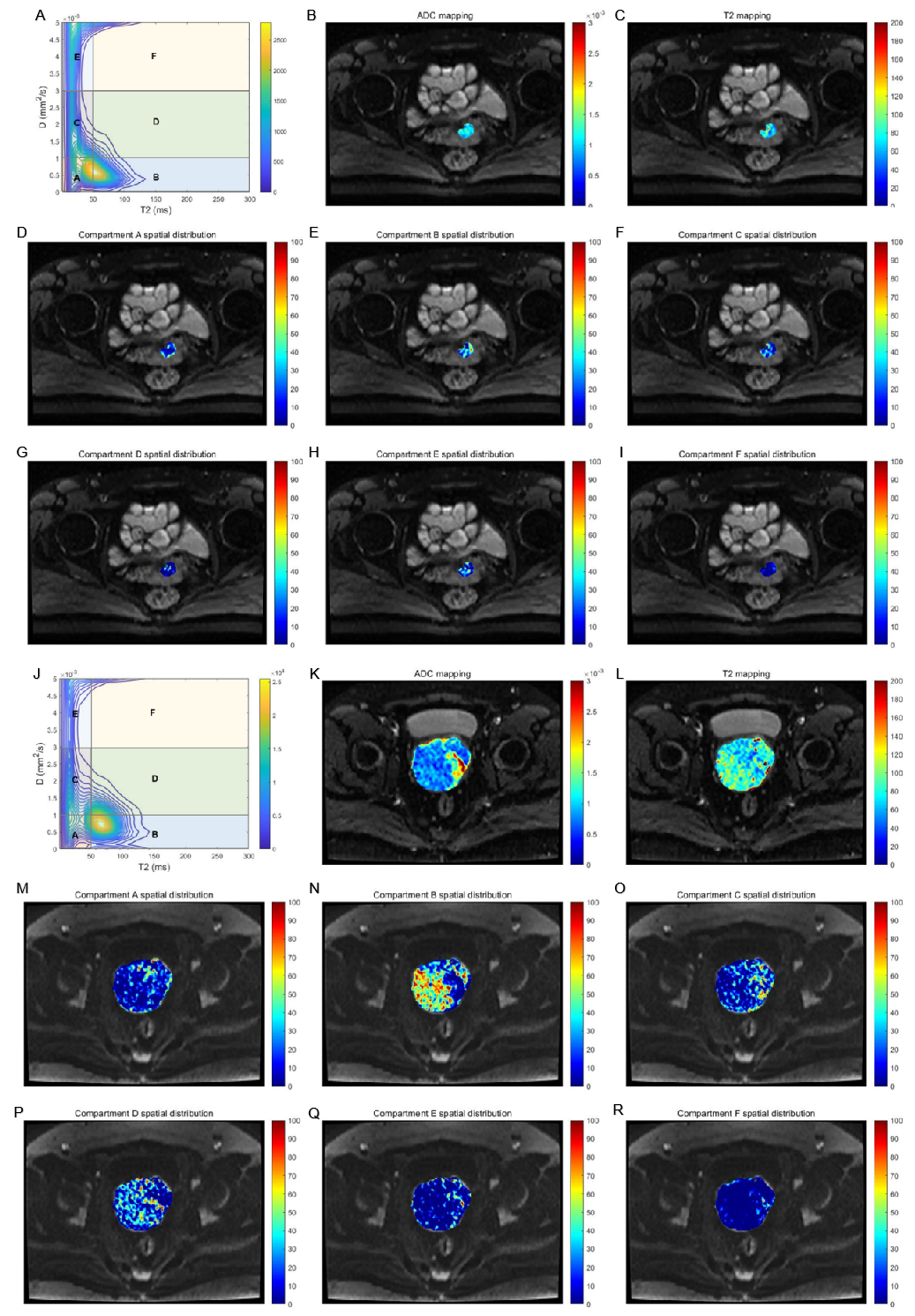
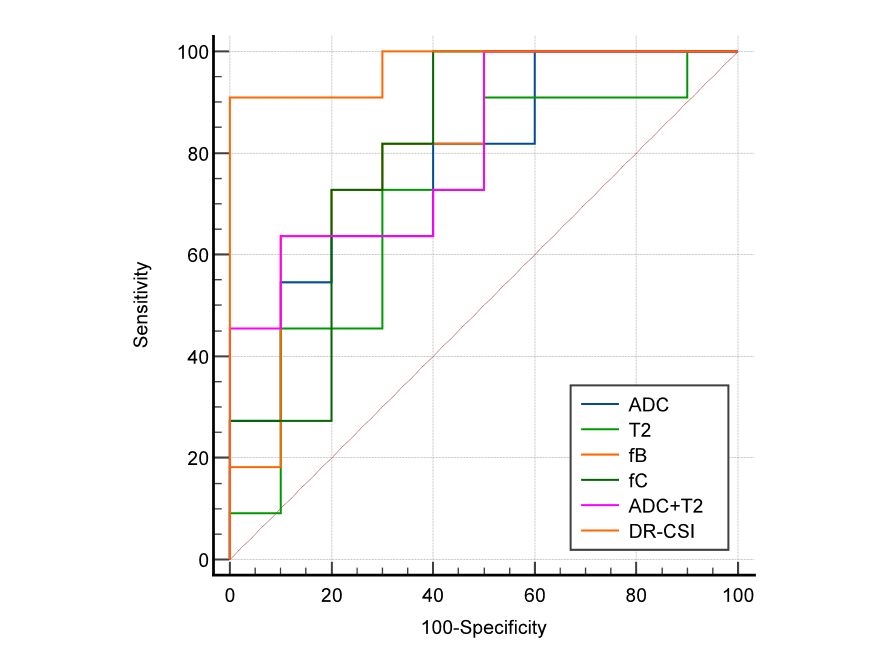
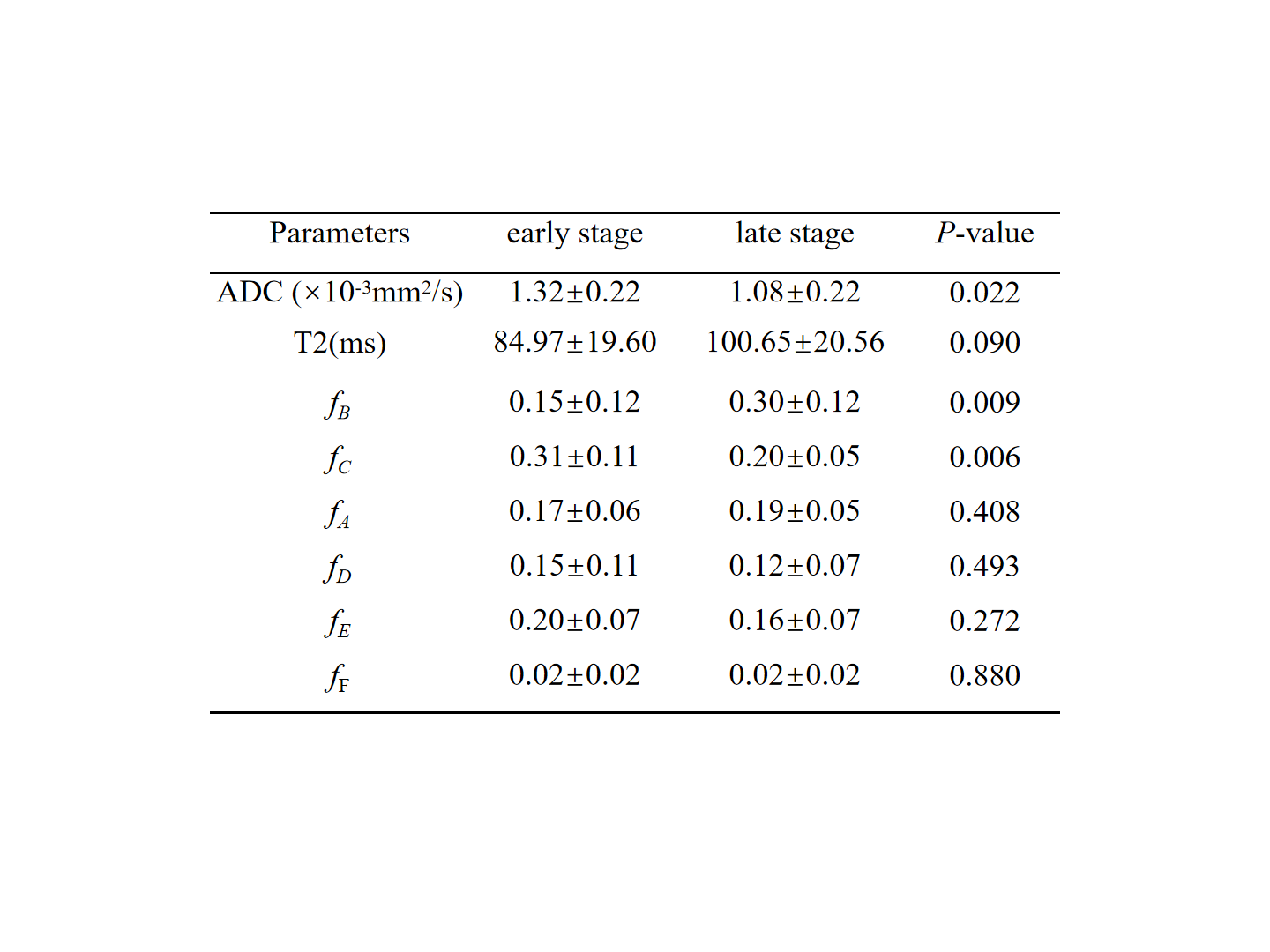
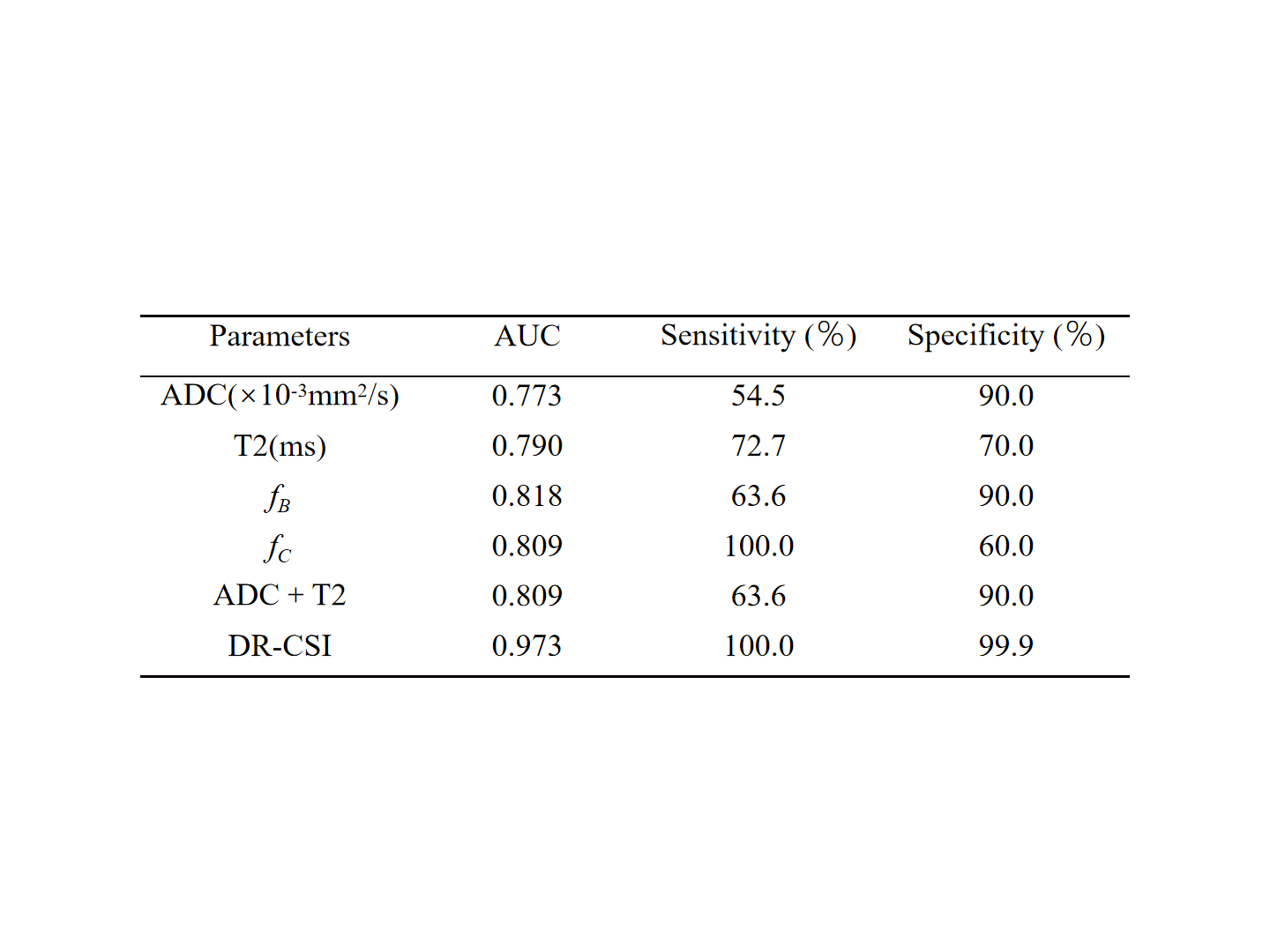
Representative images for the early and advanced SCC are shown in Fig.2. The fB was the highest in advanced SCC and fC was the highest in early SCC. The ADC (P=0.022) and fC (P=0.009) in the advanced group were significantly lower than those in the early group, while the fB was significantly higher (P=0.006) (Table1). Among single parameter, the fB showed the highest diagnostic efficiency with the area under curve (AUC) (0.818), followed by fC (0.809) and ADC (0.773). By combining the fractions of six compartments, the AUC value was improved to 0.973, which was higher than that of ADC combined with T2 (P=0.065) and significantly better than that of ADC (P=0.031) and T2 (P=0.040) alone (Table2, Fig.3).Discussion
ADC can reflect diffusion information of water molecules in tissues, while T2 reflects local physical and chemical microenvironmental changes7. As the stage of cervical cancer increases, the heterogeneity and complexity of the tumour tissue increases, which can be demonstrated by changes of f for each tissue compartment in voxels. In our study, fB was highest in advanced SCC among all compartmental fractions, indicating a predominance of compartment with lower ADC and higher T2 in advanced SCC. Advanced SCC usually has a faster rate of tumour appreciation, increased tumour cell density and reduced extracellular space compared to early stage SCC, which significantly restricts the diffusion of water molecules and results in lower ADC 8. Besides, more abundant tumour blood supply and gradual increase in micro necrotic areas as the tumour stage increases leads to the prolonged T2 value4,9. Thus fC of the compartment with higher ADC and lower T2 value was more prevalent in early SCC.Conventional ADC and T2 values are weighted averages of the diffusion coefficients and transverse relaxation of all compartments, respectively, and therefore they can not reflect the contribution of microstructural compartments to the overall voxel signal. While f derived from DR-CSI can characterize different microscopic tissue compartments within a voxel6. As such, DR-CSI may provide more biological information than single ADC and T2, which was consistent with our result that the optimal diagnostic performance of DR-CSI in staging SCC was obtained compared with ADC and T2.
Conclusion
In conclusion, the DR-CSI technique can non-invasively provide information on microscopic tissue compartments within voxels, reflecting intra-tissue heterogeneity, and identify early and advanced squamous cervical cancer by signal differences in microscopic tissue compartments. The significantly improved diagnostic performance of DR-CSI compared with conventional ADC and T2, indicated that it could provide supplement micro-information and added value for staging SCC.Acknowledgements
NO AcknowledgementsReferences
1. Salib M Y, Russell J H B, Stewart V R, et al. 2018 FIGO Staging Classification for Cervical Cancer: Added Benefits of Imaging[J]. Radiographics, 2020, 40(6): 1807-1822.
2. Shi B, Dong J N, Zhang L X, et al. A Combination Analysis of IVIM-DWI Biomarkers and T2WI-Based Texture Features for Tumor Differentiation Grade of Cervical Squamous Cell Carcinoma[J]. Contrast Media Mol Imaging, 2022, 2022: 2837905.
3. Demirbas T, Cimilli T, Bayramoglu S, et al. Contribution of diffusion-weighted imaging to diagnosis and staging of cervical cancer[J]. Balkan Med J, 2014, 31(2): 154-7.
4. Li S, Liu J, Zhang F, et al. Novel T2 Mapping for Evaluating Cervical Cancer Features by Providing Quantitative T2 Maps and Synthetic Morphologic Images: A Preliminary Study[J]. Journal of Magnetic Resonance Imaging, 2020, 52(6): 1859-1869.
5. Kim D, Doyle E K, Wisnowski J L, et al. Diffusion-relaxation correlation spectroscopic imaging: A multidimensional approach for probing microstructure[J]. Magn Reson Med, 2017, 78(6): 2236-2249.
6. Zhang Z, Wu H H, Priester A, et al. Prostate Microstructure in Prostate Cancer Using 3-T MRI with Diffusion-Relaxation Correlation Spectrum Imaging: Validation with Whole-Mount Digital Histopathology[J]. Radiology, 2020, 296(2): 348-355.
7. Mai J, Abubrig M, Lehmann T, et al. T2 Mapping in Prostate Cancer[J]. Invest Radiol, 2019, 54(3): 146-152.
8. Bhardwaj R, Boruah D K, Gogoi B B, et al. Added-Value of Diffusion-Weighted Imaging (DWI) and Dynamic Contrast-Enhanced (DCE-MRI) Magnetic Resonance Imaging in the Preoperative Assessment of Cervical Cancer[J]. J Obstet Gynaecol India, 2022, 72(4): 330-340.
9. Adams L C, Bressem K K, Jurmeister P, et al. Use of quantitative T2 mapping for the assessment of renal cell carcinomas: first results[J]. Cancer Imaging, 2019, 19(1): 35.
Figures