0434
Combining T2-weighted and synthetic double inversion recovery magnetic resonance imaging improved rectal cancer T staging1Affiliated Hospital of Jiangnan University, wuxi, China, 2MR Reseach,GE Healthcare, Beijing, China
Synopsis
Keywords: MR Fingerprinting/Synthetic MR, Cancer, rectal neoplasms; neoplasm staging;
This study aimed at investigating the role of synthetic double inversion recovery (SyDIR) magnetic resonance imaging (MRI) in staging rectal cancer (RC). 79 pathologically confirmed RC patients were retrospectively selected. Our results showed SyDIR can provided RC anatomical features for muscular infiltration detection. Compared with using T2WI alone, the combination of T2WI and SyDIR improved the diagnose performance of muscle layer invasion and significantly increase the staging consistency between MRI and pathology for both junior and senior radiologist. Our study indicated the combination of T2WI and SyDIR would be beneficial for RC treatment selection.introduction
Rectal cancer (RC) is one of the most common malignant tumors. For patients with T3-4 and /or (N+), preoperative neoadjuvant chemoradiotherapy is recommended,while total mesorectal excision is usually considered for T1-2 patients[1]. Therefore, accurate T staging is important for treatment selection. T2-weighted imaging (T2WI) is the primary magnetic resonance imaging (MRI) sequence for RC T staging, but some studies have shown that diagnostic accuracy varies from 62% to 85% [2-3].Previous studies have shown the role of double inversion recovery (DIR) MRI in distinguishing normal from tumor tissue [4-5]. However, the inversion recovery time should be defined before scanning which might not be optimum. Synthetic MRI (SyMRI) can synthesize various contrast-weighted images using quantitative T1, T2 and proton density maps obtaining from one scan [6]. For the synthetic DIR (SyDIR), the inversion recovery time can be manually adjusted to best present specific tissues which might be benefic for diagnosing.
The aim of this study was to investigate the value of SyDIR in RC T staging and if the combination of SyDIR and T2WI would improve the T staging accuracy.
Materials and Methods
Patients79 pathologically confirmed RC were selected.
MRI experiment
All MRI examinations were performed using a 3.0 T scanner (Signa Architect; GE Healthcare, Milwaukee, CA, USA) with a 16-channel phased-array body coil. The T2WI was scanned in the sagittal, axial, and coronal positions with the following parameters: TR/TE, 4000 ms/102 ms; field of view (FOV), 24 cm × 24 cm; flip angle, 111°; matrix size, 320 × 224; slice thickness, 3mm; slice number, 23. Synthetic MRI was obtained using the vendor provided MAGiC sequence with the following parameters: echo time, 19.5/97.3 ms; saturation delay time, 210/610/1810/3810 ms; FOV, 24 cm × 24 cm; FA, 111°; matrix size, 320 × 224; slice thickness, 3 mm; slice number, 23.
Data analysis
SyDIR was generated from MAGiC using Synthetic MR software (v8.0; Linköping, Sweden). According to the image contrast, the parameters of SyDIR are manually set as follow: TR/TE, 15000 ms/100 ms; TI1/TI2, 470 ms/3750 ms.MRI based T staging was conducted by one junior and one senior radiologist with four and twenty years clinic experience, respectively.All statistical analyses were performed in SPSS and MedCalc software. Weighted Kappa-test was used to evaluate the consistency of the RC T staging between MRI and pathology results. The receiver operating characteristic curve (ROC) was used to present the staging performance of using T2WI alone and the combination of T2WI and SyDIR. The area under the curve (AUC) of ROC was used to evaluate the diagnosis efficiency. P<0.05 was considered statistical significance.
Results
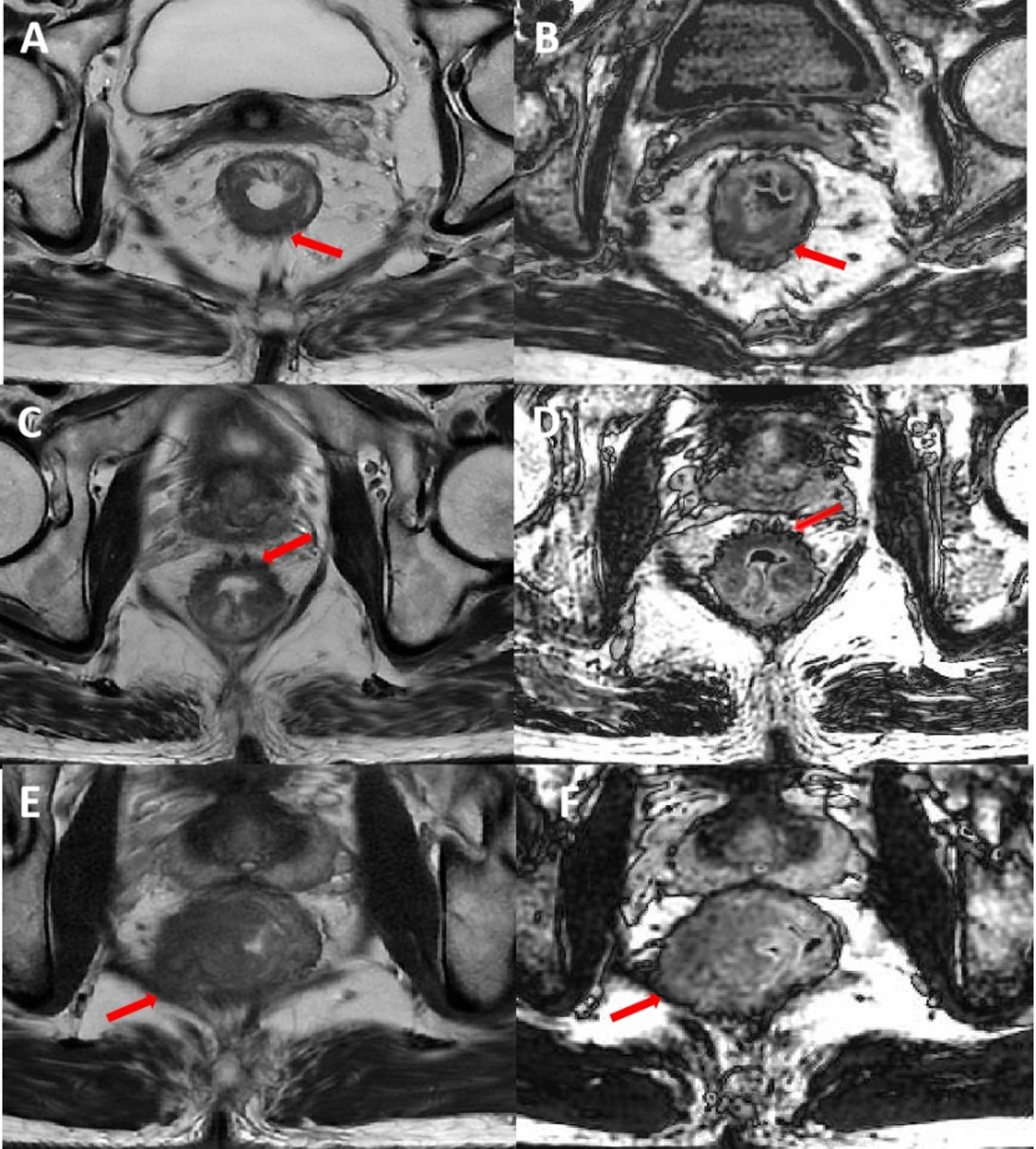
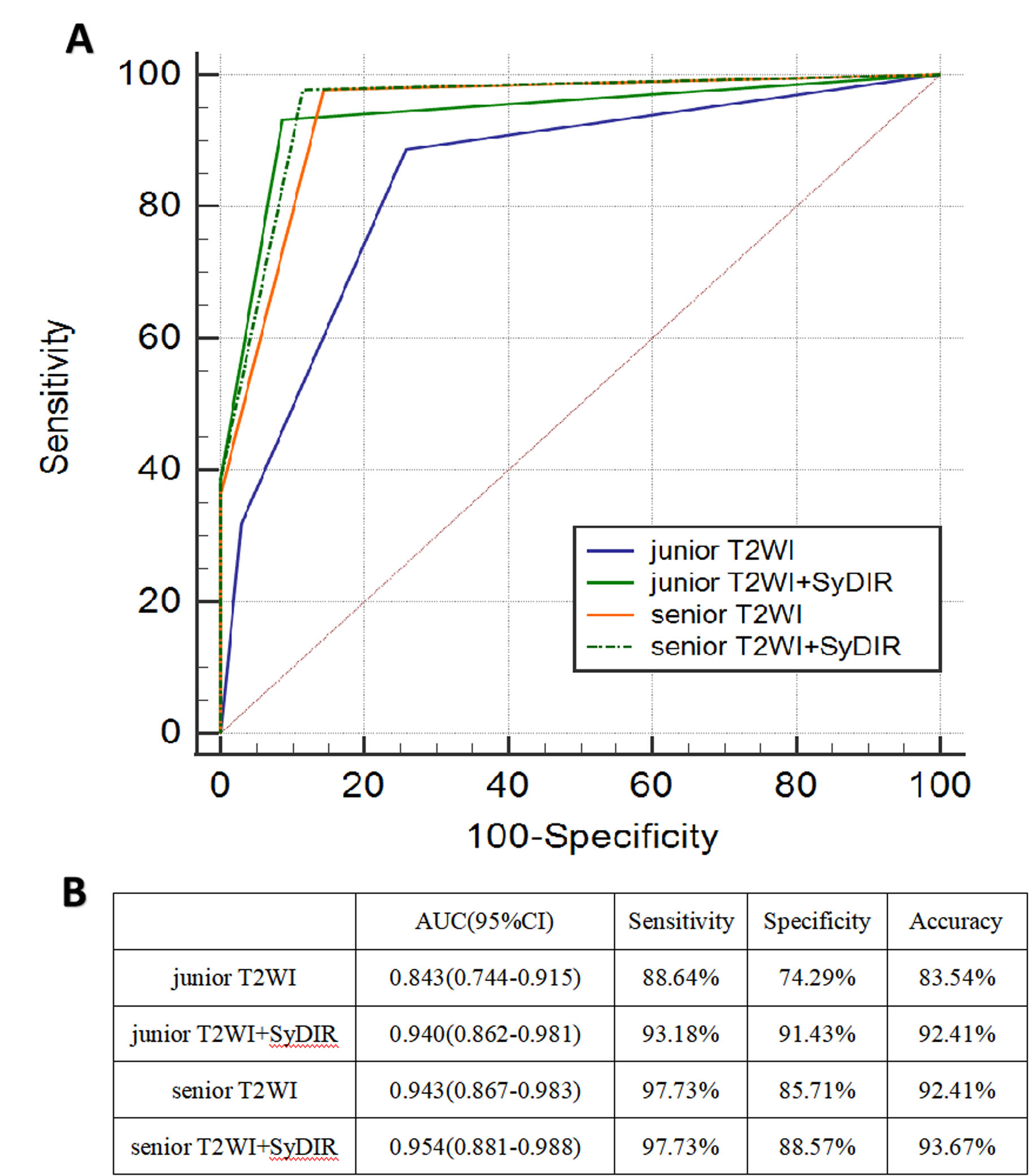
It’s difficult to differentiate T1 and T2 stage RC using MRI [2]. So, these patients were group together in this study. The number of pathologically confirmed T1-2, T3 and T4 stage patients was 35, 27 and 17, respectively. The T1-2 stage patients did not show muscle layer infiltration but the T3 and T4 stage patients did.For the T2 stage patients, the local boundary between tumor and muscular layer was unclear and a cork-like hypointensity shadow can be observed in the mesorectal membrane on T2WI (Fig.1 A). SyDIR of the same patient showed well-demarcated slightly hyperintensity tumor and no spines associated with the lesion were seen in the mesorectal membrane (Fig.1 B). On the T2WI, the spinous protrusions invaded the mesorectum at the outer edge of the tumor can be observed in T3 stage patients (Fig.1 C). SyDIR showed the tumor boundary was serrated and invaded the perirectal mesangium in the same T3 stage patient (Fig.1 D). For the selected T4 stage patient, SyDIR clearly showed the dark hook of tumor invaded the left levator ani muscle (Fig.1 F), but this was unclear on the T2WI (Fig.1 E).As shown in figure 2, the combination of T2WI and SyDIR also improved the diagnose performance of muscle layer invasion for both junior and senior radiologist (AUC increased from 0.843 to 0.94 and from 0.943 to 0.954, respectively).
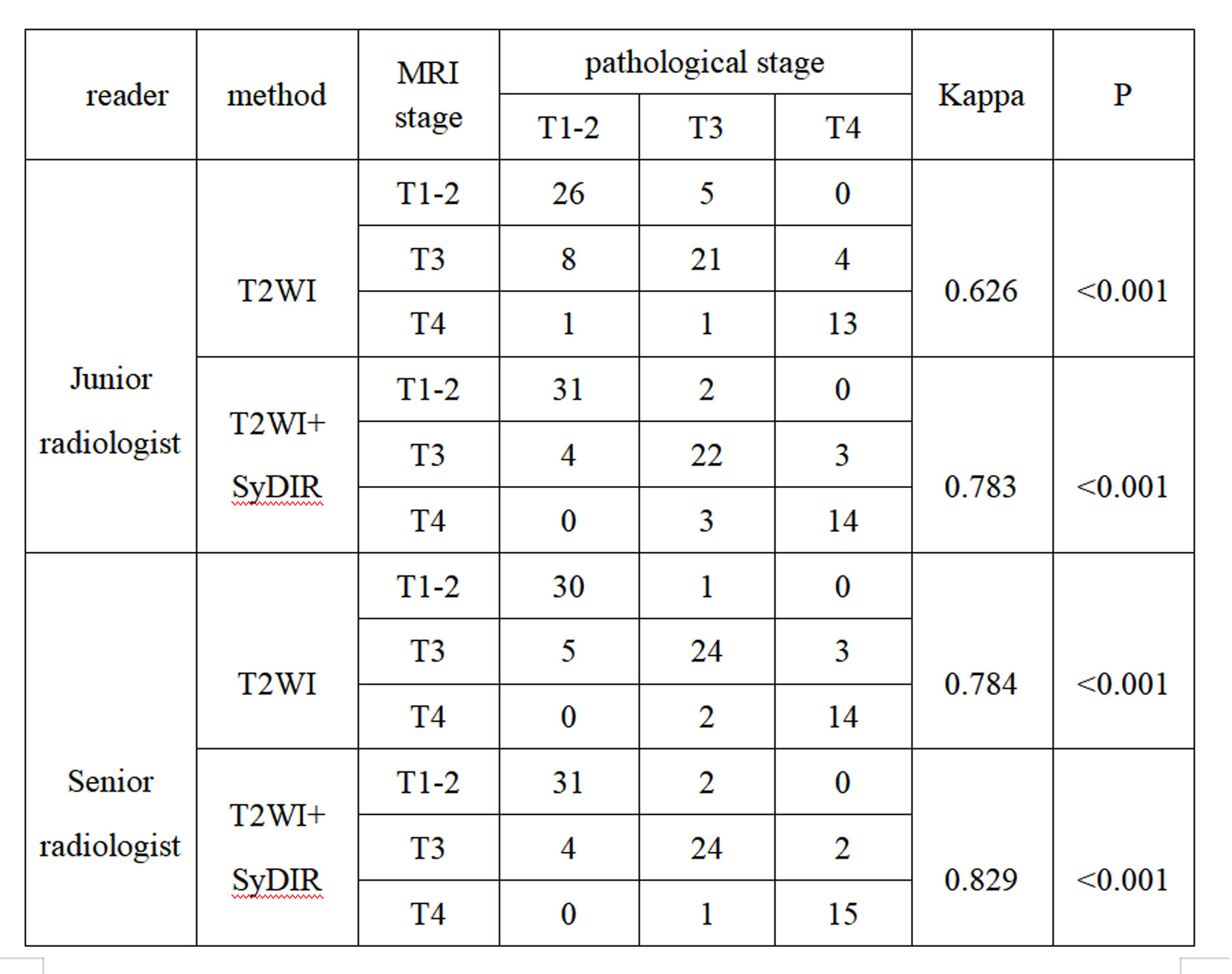
As shown in Table 1, compared using T2WI alone, the consistency of RC T staging using combination of T2WI and SyDIR was significantly improved from 0.626 to 0.784 and from 0.783 to 0.829 for junior and senior radiologist, respectively.
Discussion and conclusion
Our study showed SyDIR provided additional information to T2WI for characterizing the anatomical feature of RC. Compared with using T2WI alone, the consistency between pathology and MRI T staging was significantly increased using the combination of T2WI and SyDIR for both junior and senior radiologist (all P<0.001). The combination also improved the diagnose performance of muscle layer infiltration which was important for differentiating T1-2 from T3-4. Particularly, the junior radiologist almost reached the diagnose performance of senior radiologist by combining T2WI and SyDIR. Taking the prediction accuracy for example, it increased from 83.54% to 92.41% and from 92.41% to 93.67% for junior and senior radiologist, respectively.In conclusion, the SyDIR can be used to characterize RC tumor. The combination of T2WI and SyDIR increased the accuracy of muscle layer infiltration and improved the T staging performance which would be beneficial for treatment selection.
Acknowledgements
Acknowledgments
We thank Ke-Wei Wang for help with the statistical analysis of the data in this paper. We thank Yu-xi Ge, Xin-yi Zhou and Bo-jian Fei for their contributions to patient treatment data collection. All authors had access to the study data, and reviewed and approved the final manuscript.
Funding:This study was funded by the Wuxi Scientific and technological achievements and suitable technology Popularization(Grant No. T202036).
Compliance with ethical standards
Guarantor:The scientific guarantor of this publication is Shu-dong Hu, M.D., Ph.D.
Conflict of interest :The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Statistics and biometry :Ke-Wei Wang kindly provided statistical advice for this manuscript.
Informed consent :Written informed consent was waived by the Institutional Review Board.
Ethical approval :Institutional Review Board approval was obtained.
Study subjects or cohorts overlap
No subjects or cohorts have been previously reported.
Methodology:retrospective;diagnostic study ;performed at one institution
References
1. Benson AB III, Venook AP, Al-Hawary MM et al (2018) Rectal cancer, version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 16:874–901.
2. White R, Ung KA, Mathlum M. Accuracy of magnetic resonance imaging in the pre-operative staging of rectal adenocarcinoma: Experience from a regional Australian cancer center. Asia Pac J Clin Oncol, 2013, 9(4): 318-323.DOI: 10.1111/ajco.12033.
3. Al-Sukhni, E, Milot, L, Fruitman, M, et al. Diagnostic accuracy of MRI for assessment of T category, lymph node metastases, and circumferential resection margin involvement in patients with rectal cancer: a systematic review and meta-analysis. ANN SURG ONCOL. 2012; 19 (7): 2212-23. doi: 10.1245/s10434-011-2210-5
4. Kim JH, Ryu JK, Jahng GH, et al. Double inversion recovery MR imaging of the breast: efficacy in detection of breast cancer. J Magn Reson Imaging, 2014, 39(1): 51-58. DOI:10.1002/jmri.24115.
5.Onwuharine EN, Clark AJ. Comparison of double inversion recovery magnetic resonance imaging (DIR-MRI) and dynamic contrast enhanced magnetic resonance imaging (DCE-MRI) in detection of prostate cancer: A pilot study. Radiography (Lond), 2020, 26(3): 234-239. DOI:10.1016/j.radi.2019.12.012.
6.Maitra, R, Riddles, JJ. Synthetic magnetic resonance imaging revisited. IEEE T MED IMAGING. 2010; 29 (3): 895-902. doi: 10.1109/TMI.2009.2039487
Figures