0399
A Multi-Site Collaborative Training Effort to Improve Neuroimaging Accessibility and Capacity Development in Low- and Middle-Income Countries1Department of Paediatrics and Child Health, University of Cape Town, Cape Town, South Africa, 2Neuroscience Institute, University of Cape Town, Cape Town, South Africa, 3Department of Neuroimaging, King's College London, London, United Kingdom, 4Department of Medical Radiation Physics, Lund University, Lund, Sweden, 5Maternal, Newborn, and Child Health (MNCH) Discovery and Tools (D&T), Bill and Melinda Gates Foundation, Seattle, WA, United States
Synopsis
Keywords: Neuro, Low-Field MRI, Training, Capacity Development, Low- and Middle Income Countries
In a multi-site global collaboration (UNITY; Ultra-Low Field Neuroimaging In The Young) implementing the novel Hyperfine 64mT low-field MRI into research on relevant health priorities in low- and middle-income countries (LMICs), capacity development has been identified as a key objective. Following an initial training wave in foundational sites including South Africa, adapted workshops have been conducted in new consortium countries including Malawi, Ethiopia, and Ghana. This has informed the development of a strategic framework for context-specific training aimed at promoting the increased success of neuroimaging in research and clinical practice, and the sustainability of MRI technology in under-resourced settings.Introduction
Traditionally, Magnetic Resonance Imaging (MRI) is performed using high magnetic fields which are costly, requiring significant infrastructure and specialized staff. It is, therefore, an inaccessible tool for most Low- and Middle-Income Countries (LMICs) resulting in disproportionately less neuroimaging studies emerging from these regions.1,2 The Hyperfine Swoop 64mT low-field MRI system has recently become available,3 eliminating some of these challenges for less accessible and under-resourced settings.4 The system also yields practical benefits for paediatric MRI including a scanner that is quieter, mobile, and more child-friendly than conventional systems.5 Preliminary validation studies using the Hyperfine system on neurotypical children between 6 weeks and 16 years of age in high-income settings have been positive, demonstrating the potential of low-field imaging as a complement to traditional high-field MRI.4 However, the utility of these systems in detecting child brain changes associated with various pathologies and risks, many of which are more prevalent in LMICs,6-8 is unknown. Research evaluating the Hyperfine system’s ability to answer questions of clinical relevance as detected by traditional MRI is necessary, particularly in LMICs where the availability of neuroimaging has historically been limited. Additionally, to promote the long-term sustainability of feasible MRI approaches in under-resourced settings, training strategies and capacity development need to be fostered.Methods
In an effort to validate the Hyperfine MRI system’s efficacy across settings, a collaborative multi-site project, Ultra-Low Field Neuroimaging in the Young (UNITY), has been initiated and funded by the Bill and Melinda Gates Foundation. UNITY comprises 20 sites across 4 continents, with growing numbers globally. The consortium’s objective is to implement the Hyperfine Swoop as a complementary tool in ongoing research in these countries on context-specific health priorities including HIV, malnutrition, anaemia, neonatal encephalopathy, and cerebral malaria. The University of Cape Town in South Africa, having had previous paediatric high-field MRI experience, was one of the first African sites to receive a Hyperfine system. Their team have championed the incorporation of this novel tool into research on important and prevalent risk factors for child brain development (Figure 1).With the international expansion of UNITY and the inclusion of additional LMICs, training has been critical for the practical administration of the Hyperfine system, capacity development and skills acquisition, and long-term feasibility and success of low-field neuroimaging in these contexts. At the start of UNITY, an initial training wave included a video series shared by King’s College London during the COVID-19 pandemic and onsite Hyperfine installation training across the consortium for foundational sites including Cape Town. Following this, on the behalf of UNITY, the Cape Town team adopted the established peer model, and have been integral in leading the training portfolio by adapting workshops for newer sites in similar yet unique African LMICs. These include Malawi, Ethiopia, and Ghana. Training has included theoretical knowledge dissemination and resource sharing, practical demonstrations on procedures and clinical approaches, and supervised scan acquisition with paediatric patients. Based on feedback from Ghana, we have developed a structured training programme and strategic guideline for optimal training and equitable implementation of low-field neuroimaging methods in LMICs.
Results
Thus far, Cape Town has completed 178 scans of three-month-old babies and 62 scans of three-year-old children (Figure 2) with a success rate of 71% and 74%, respectively. Based on recent UNITY methods for processing ultra-low field MRI data9, pilot paediatric Hyperfine scans were reconstructed from three orthogonally acquired non-isotropic images (axial, coronal, and sagittal) into single 1.5mm isotropic images (Figure 3) and segmented accordingly. Preliminary findings suggest moderate correlations across Hyperfine and 3T MRI systems for total intracranial volume (r=0.68, p=0.02), grey matter (r=0.65, p=0.03), and white matter (r=0.73, p=0.01).The findings of UNITY training workshops highlight the importance of both theoretical and practical training components with an emphasis on 10 key points within three categories: logistical considerations, clinical approaches, and collaborative efforts. Overall, the recommendations emphasise the importance of technical support, checklists and standard operating procedures, communication and joint organisation, sufficient training duration, training location at the host site, theoretical foundations, interactive practical demonstrations, incorporating pilot data collection, prioritizing research participants, and cross-site partnerships and teamwork. Data collection has successfully begun at all trainee sites.
Discussion
As neuroimaging technology continues to transform healthcare and research landscapes globally, there is increased recognition of the MRI need in LMICs where the burden of disease is highest. However, given reported gaps in infrastructure and resources, training opportunities, specialised skills, maintenance, and capacity in these contexts, there are ongoing challenges in ensuring sustainable MRI access. By introducing the Hyperfine low-field MRI into research on health priorities in unique LMIC contexts, UNITY may provide insight into the system’s ability to detect key neuroimaging findings associated with paediatric risk. Should this be successful, ultra-low field MRI may also be more broadly feasible as an outcome tool in current and planned intervention trials globally. Thus far, preliminary processing of Hyperfine data is promising. However, to reach planned objectives and ensure long-term sustainability of MRI access in under-resourced settings less familiar with neuroimaging methods, effective training and capacity development goals are critical. The development of a strategic framework with training guidelines represents an important step forward for neuroimaging in Africa and the broader LMIC context.Acknowledgements
We would like to thank all of the UNITY teams across sites who participated in our training workshops, and are making invaluable contributions to the goals and objectives of the consortium. We also thank the Hyperfine team for their ongoing technical support.
UNITY is supported by the Bill and Melinda Gates Foundation (BMGF; Ultralow field Neuroimaging In The Young; INV-005798). Additional funding is provided by the BMGF (INV-023509) for K.A. Donald to support low-field MRI acquisition in Cape Town, South Africa. Furthermore, J.E. Ringshaw is supported by the Wellcome Trust through an International Training Fellowship (224287/Z/21/Z).
References
1. Azhari A, Truzzi A, Neoh MJ-Y, et al. A decade of infant neuroimaging research: What have we learned and where are we going? Infant Behavior and Development 2020; 58: 101389.
2. Anazodo UC, Ng JJ, Ehiogu B, et al. A Framework for Advancing Sustainable MRI Access in Africa. NMR in Biomedicine 2022: e4846.
3. Hyperfine. Portable MR Imaging: Bringing MRI to the Patient. 2021. https://hyperfine.io.
4. Deoni S, Bruchhage MM, Beauchemin J, et al. Accessible pediatric neuroimaging using a low field strength MRI scanner. NeuroImage 2021; 238: 118273.
5. Deoni SC, Medeiros P, Deoni AT, et al. Development of a mobile low-field MRI scanner. Scientific reports 2022; 12(1): 1-9.
6. Black MM, Walker SP, Fernald LC, et al. Advancing Early Childhood Development: From Science to Scale 1: Early childhood development coming of age: Science through the life course. Lancet (London, England) 2017; 389(10064): 77.
7. Walker SP, Wachs TD, Gardner JM, et al. Child development: risk factors for adverse outcomes in developing countries. The lancet 2007; 369(9556): 145-57.
8. Donald KA, Wedderburn CJ, Barnett W, et al. Risk and protective factors for child development: An observational South African birth cohort. PLoS Medicine 2019; 16(9): e1002920.
9. Deoni SC, O'Muircheartaigh J, Ljungberg E, Huentelman M, Williams SC. Simultaneous high‐resolution T2‐weighted imaging and quantitative T 2 mapping at low magnetic field strengths using a multiple TE and multi‐orientation acquisition approach. Magnetic Resonance in Medicine 2022.
Figures

Figure 1. Photographic image of the Hyperfine Swoop 64mT MRI system being used for paediatric neuroimaging acquisition at the University of Cape Town
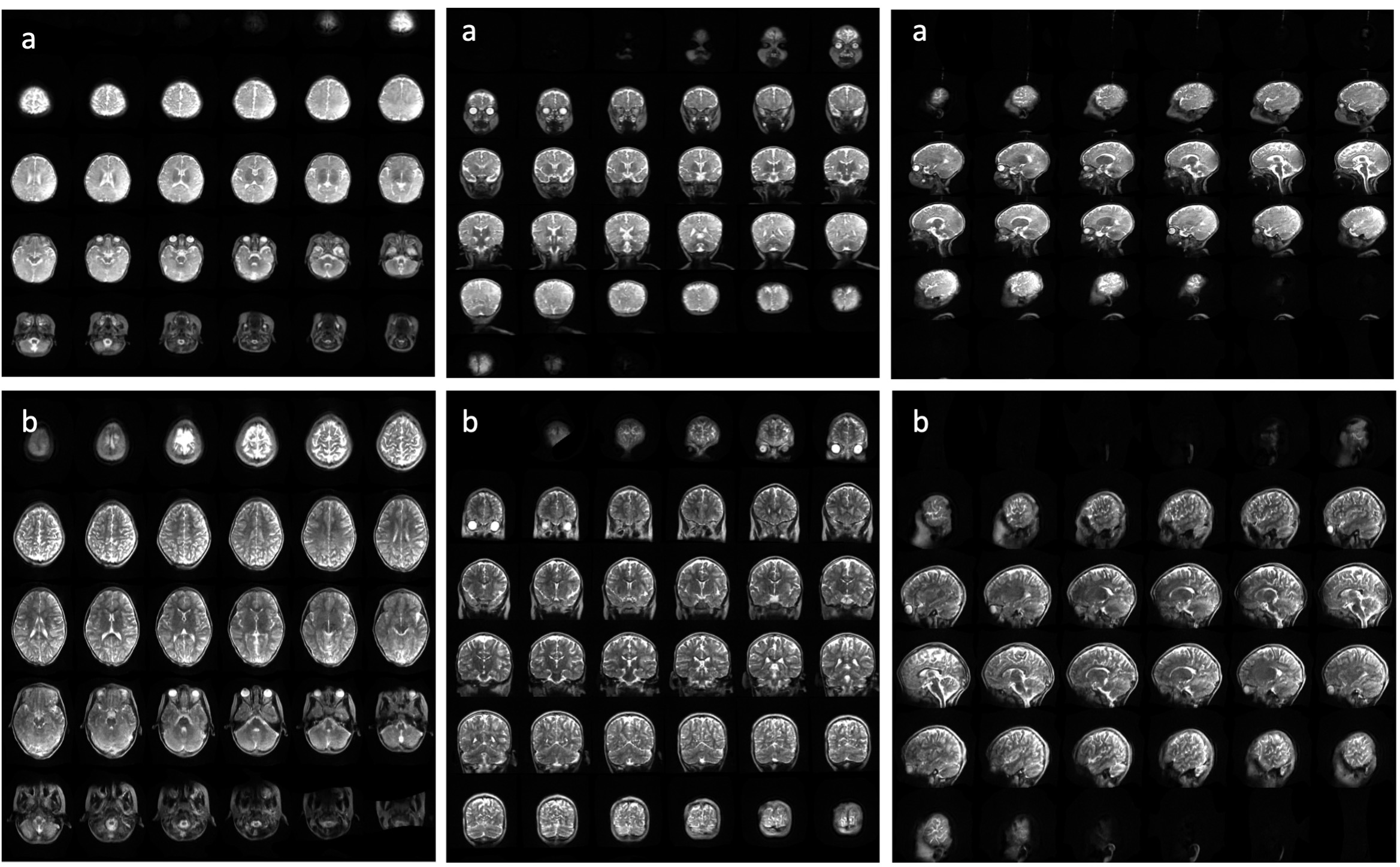
Figure 2. Example of a Hyperfine Swoop 64mT T2-weighted paediatric brain MRI in axial (left), coronal (middle), and sagittal planes (right) at 3 months (a) and 3 years of age (b)
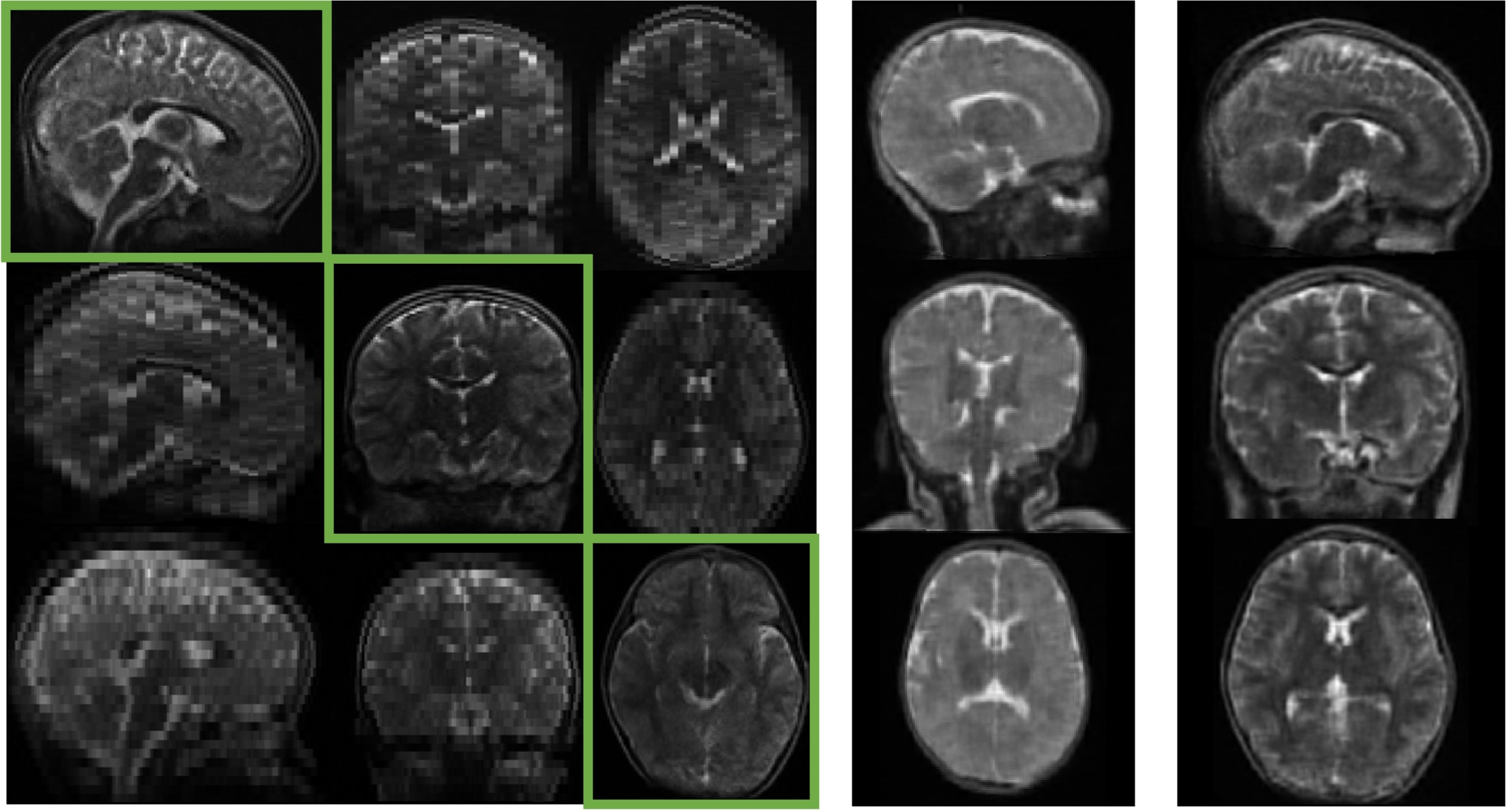
Figure 3. Reconstruction of Hyperfine Swoop 64mT orthogonally acquired non-isotropic images (axial, coronal, and sagittal) into a single 1.5mm isotropic image with Advanced Normalization Tools (ANTs) using an age-matched infant 3T atlas (NIHPD) for paediatric MRI. Results are shown in the child brain at 3 months of age (a) and 3 years of age (b).