0348
Comparison of k-space center, FID and Pilot Tone navigators in abdominal motion tracking for optimal XD-GRASP reconstruction1Quantitative Intelligent Imaging Lab (QUIN), Department of Radiology, Boston Children's Hospital and Harvard Medical School, Boston, MA, United States, 2Advanced Clinical Imaging Technology, Siemens Healthineers International AG, Lausanne, Switzerland, 3Department of Radiology, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland, 4LTS5, École Polytechnique Fédérale de Lausanne (EPFL), Lausanne, Switzerland
Synopsis
Keywords: Motion Correction, Body
Abdominal MRI scans often require breath-holding to prevent image quality degradation, which can be challenging for patients. XD-GRASP enables generation of motion-robust images for free-breathing abdominal MRI by binning the data into respiratory phases. In this study, we compared three navigation techniques, namely k-space center, free induction decay navigators (FIDnavs) and pilot tone (PT), for XD-GRASP reconstruction. FIDnavs and PT have advantages over k-space center navigation since they are insensitive to gradient delays, independent of the imaging plane and acquired more frequently. The image quality ranking means (1=best,2=moderate,3=worst) were 1.4, 1.6 and 2 for FIDnavs, PT and k-space center, respectively.Introduction
Respiratory motion remains a major challenge for abdominal MRI, especially when imaging pediatric patients1. Recently, a radial imaging technique based on a stack-of-stars sampling trajectory has been used to bin the data into separate respiratory phases, enabling reconstruction of motion-robust images for each motion state (phase), known as XDGRASP2. Radial imaging has self-navigating properties as motion information can be extracted from the central k-space signal of each radial line. However, the k-space center is often inaccurate due to gradient delays, eddy currents and depends on slice orientation and position3-5. Moreover, if multiple slices are acquired in a 3D sequence, k-space center navigator’s temporal resolution is limited, resulting in less frequent measurements than the physiological motion. Unlike k-space center-based navigators, free induction decay navigators (FIDnavs) measure the k-space center directly without any spatial encoding and have been shown to provide accurate motion measurement and correction6-8. Recently, a small wireless RF transmitter that generates a reference signal called Pilot-Tone (PT) was shown to be capable of capturing physiological motion changes4,9,10. The PT signal can be detected simultaneously with the MRI signal, and can be used as an alternative navigator. In this study, we compared the use of three different navigators, namely k-space center, FIDnav and PT, for binning the respiratory motion into motion states for XD-GRASP reconstruction.Methods
FIDnavs (ADC duration=0.4ms, TNav=2 ms) were inserted into a golden angle-ordered radial stack-of-stars sequence. PT transmitter box was placed on the patient table next to the hip of the volunteer. Five volunteers (3 female, age range=32-41 years) were scanned at 3T (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) following written, informed consent. Spine and body matrix coils were used. Volunteers were asked to perform irregular breathing in one scan and normal/shallow breathing (no motion) in another scan. Data were acquired in both axial and coronal imaging orientations. K-space center, FIDnavs, and PT navigation signals were captured in the same scan for each breathing experiment and imaging orientation. The total scan time was 2.5 and 3.1 minutes for coronal and axial scans, respectively. Imaging parameters were TE/TR/FA = 1.49ms/4ms/9˚, 32 coronal slices or 44 axial slices with slice Partial Fourier = 6/8, voxel size = 1.2x1.2x3mm3 and 1326 radial spokes. All three navigator signals were extracted from the raw data. Principal component analysis and coil clustering were applied to select the most representative physiological motion signal2,4. XD-GRASP reconstructions were performed by binning into six motion states based on each navigation signal, namely k-space center, FIDnavs, and PT. A panel of experienced radiologists sorted two motion states of each scan according to their image quality and the severity of motion artifacts. Reviewers were blinded to the navigation type used for binning (i.e., k-space center, FIDnavs, or PT).Results
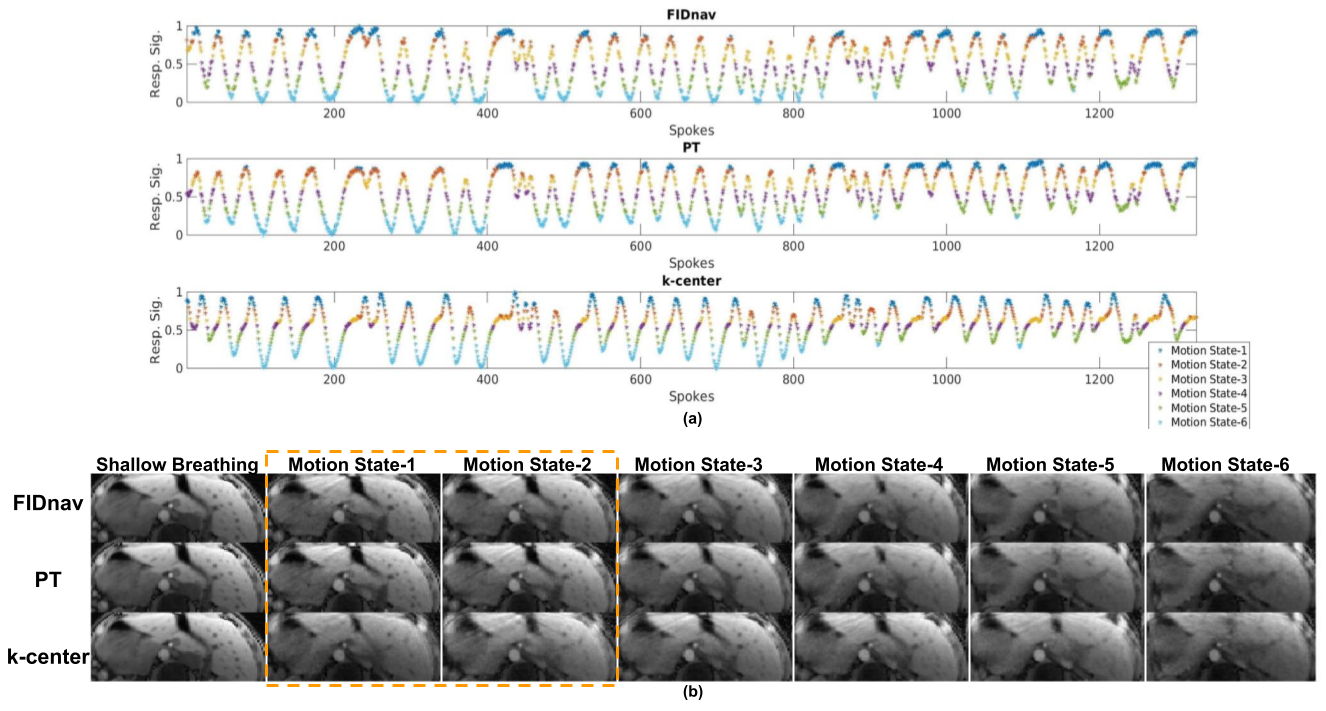
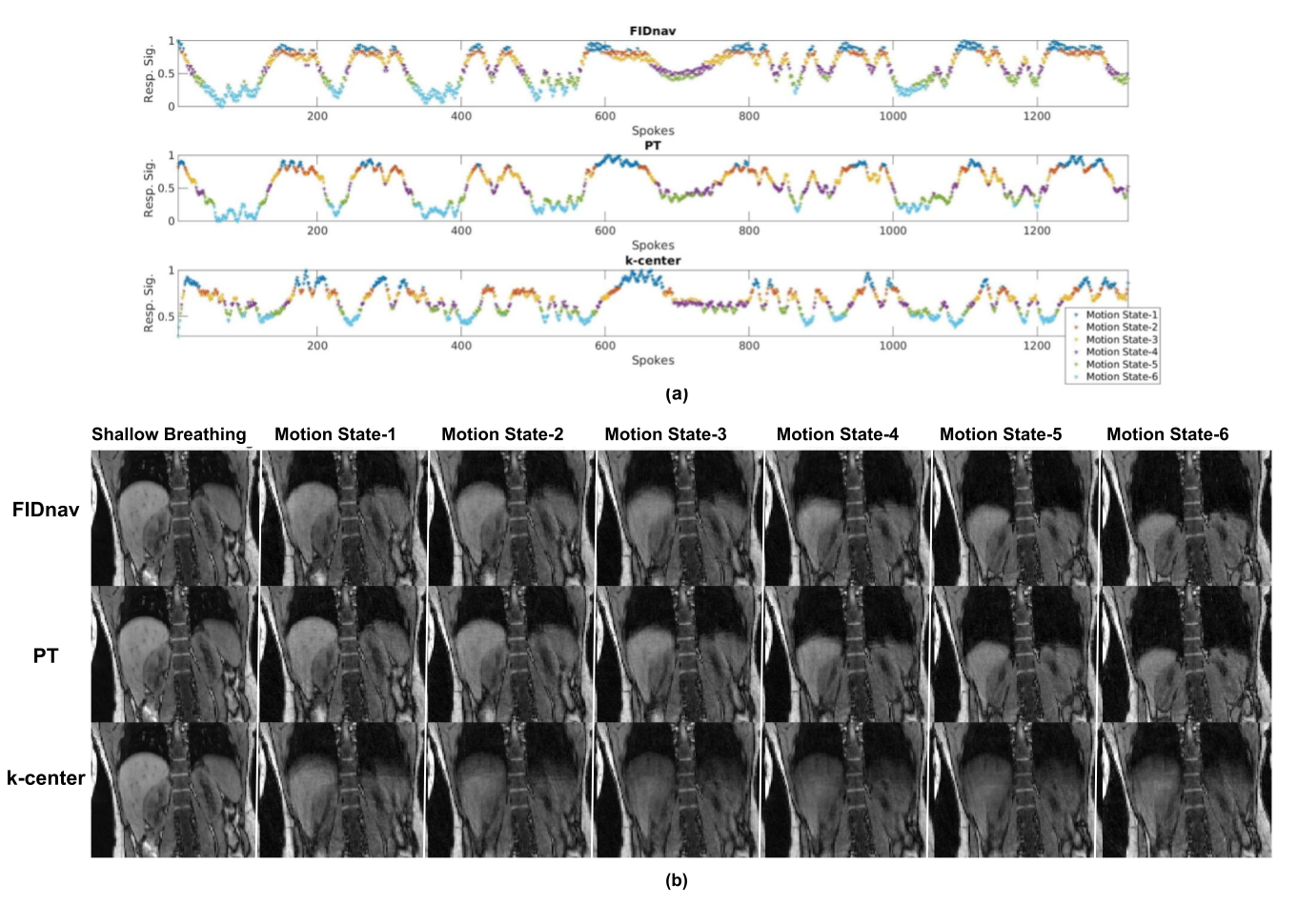
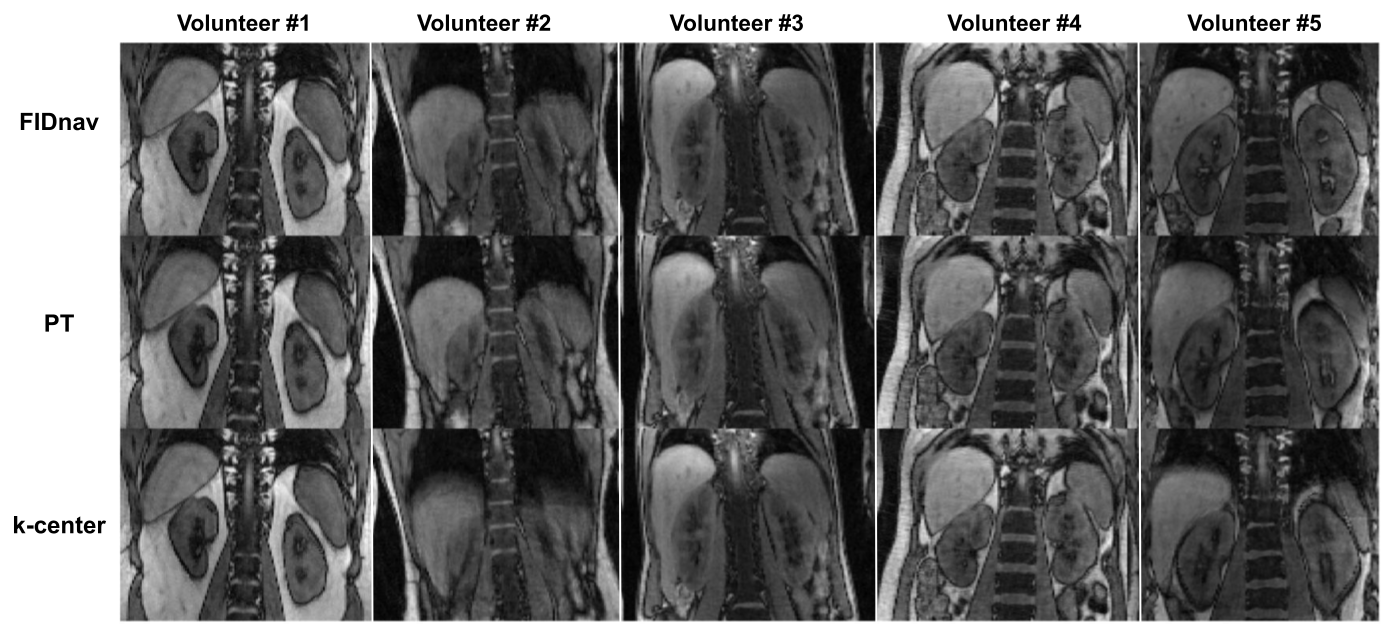
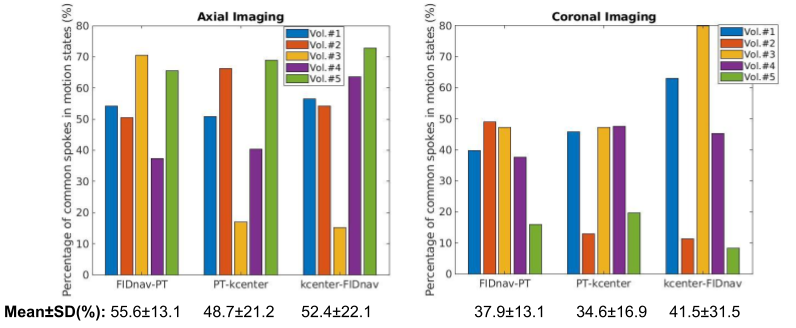
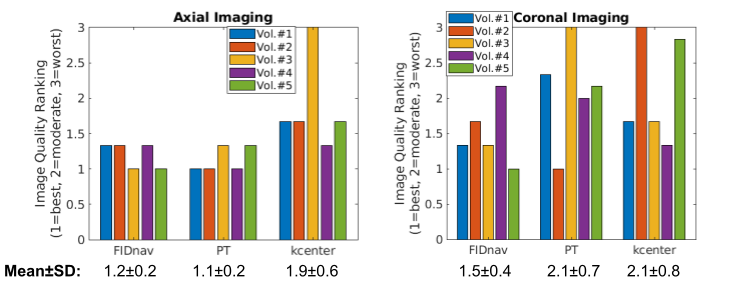
XD-GRASP reconstructions with binning based on each method are shown for axial (Figure 1) and coronal (Figure 2) acquisitions. It can be observed that FIDnav and PT navigation provide motion-robust axial images of the liver, whereas blurring and motion artifacts are still present with k-space center navigation. Figure 3 shows the end of expiration states for all 5 volunteers, highlighting motion artifacts for k- space center navigation for volunteers #2 and #5. Figure 4 compares the difference of binning based on different navigators and the percentage of data points that were placed into the same bin when using different navigators were reported. Figure 5 shows the image quality rankings for XD-GRASP reconstructions using each navigator. High standard deviation was observed for image quality ranking of k-space center navigated XD-GRASP reconstruction across volunteers for both axial and coronal imaging.Discussion and Conclusion
Employing FIDnavs or PT for binning into motion states decreased the motion artifacts and blurring compared to using k-space center navigator (Figure 1-3). In addition, it is observed that PT and FIDnav-based binnings were more consistent across subjects with each other compared to k-space center-based binning (Figure 4). As shown in Figure 5, XD-GRASP reconstructions that employed FIDnavs as navigators, ranked as the ones with the best mean image quality (ranking=1.4), followed by PT (ranking=1.6) and finally k-space center (ranking=2.0). This result is reasonable due to inaccuracy of k-space center measurements caused by system imperfections, dependence on slice orientation and coarser sampling. Coronal imaging with PT ranked worse than axial imaging with PT. The reason of this might be that the extraction of PT navigator in coronal imaging is more challenging and may overlap with the MRI signal deployed by the tissue compared to axial imaging. Furthermore, when in-plane imaging is not located at iso-center in radial imaging, PT spectral peak in image shifts with every spoke angle, hence a rigorous peak detection algorithm is essential4. Future work may involve fusion of navigator signals for improving their robustness for binning.Acknowledgements
This work was supported in part by NIH grants R01 EB019483, R01 NS121657, R01 DK125561, R21 DK123569, R21 EB02962, S10OD025111 and a pilot grant (PP-1905-34002) from the National Multiple Sclerosis Society. We thank the Center for Advanced Imaging Innovation and Research (CAI2R) at NYU for supplying the 3T Pilot Tone device used in this work.References
1. Chavhan, Govind B., Paul S. Babyn, and Shreyas S. Vasanawala. "Abdominal MR imaging in children: motion compensation, sequence optimization, and protocol organization." Radiographics 33.3 (2013): 703-719.
2. Feng, Li, et al. "XD-GRASP: golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing." Magnetic resonance in medicine 75.2 (2016): 775-788.
3. Stemkens B, Benkert T, Chandarana H, et al. Adaptive bulk motion exclusion for improved robustness of abdominal magnetic resonance imaging. NMR Biomed. 2017;30(11).
4. Solomon, Eddy, et al. "Free-breathing radial imaging using a pilot-tone radiofrequency transmitter for detection of respiratory motion." Magnetic resonance in medicine 85.5 (2021): 2672-2685.
5. Ariyurek C, Wallace TE, Kober T, Kurugol S, Afacan O. Prospective motion correction in kidney MRI using FID navigators. Magn Reson Med. 2023;89:276-285.
6. Brau ACS, Brittain JH. Generalized self-navigated motion detection technique: Preliminary investigation in abdominal imaging. Magn Reson Med. 2006;55(2):263-270.
7. Kober T, Marques JP, Gruetter R, Krueger G. Head motion detection using FID navigators. Magn Reson Med. 2011;66(1):135-143.
8. Wallace TE, Afacan O, Waszak M, Kober T, Warfield SK. Head motion measurement and correction using FID navigators. Magnetic Resonance in Medicine. 2019;81(1):258-274.
9. Ludwig, Juliane, et al. "Pilot tone–based motion correction for prospective respiratory compensated cardiac cine MRI." Magnetic Resonance in Medicine 85.5 (2021): 2403-2416.
10. Falcão, M. B. L. et al. Pilot tone navigation for respiratory and cardiac motion-resolved free-running 5D flow MRI. Magn Reson Med 87, 718–732 (2022).
Figures