0342
Characterize right ventricle deformation pattern in pulmonary arterial hypertension using layer-specific strain cardiovascular MRI1State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2MR Collaboration, Siemens Healthineers Ltd, Beijing, China, 3Siemens Shenzhen Magnetic Resonance Ltd, Shenzhen, China, 4Magnetic Resonance, Siemens Healthcare, Erlangen, Germany, 5Emergency Center, State Key Laboratory of Cardiovascular Disease, Key Laboratory of Pulmonary Vascular Medicine, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 6Center of Pulmonary Vascular Disease, State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
Synopsis
Keywords: Myocardium, Rare disease, Strain, right ventricle
This is the first study to describe the distribution pattern of right ventricular layer-specific strain/strain rate in pulmonary arterial hypertension patients by processing cine cardiovascular MR images using a deformation registration algorithm based strain analysis software.Introduction
When right ventricle (RV) is under pressure overload, most commonly secondary to pulmonary hypertension, hypertrophy and reorientation of RV myocyte would happen1 and might finally lead to RV dysfunction. However, in spite of the clinical importance of RV deformation in pulmonary arterial hypertension (PAH), the layer-specific strain/strain rate distribution patterns in RV measured by cardiovascular magnetic resonance imaging (CMR) have not been reported.Methods
As a sub-cohort from a real-world observation based Chinese national prospective multi-center observational registry study 1, newly diagnosed PAH patients were prospectively recruited between January 2011 and December 2017. All enrolled patients received right heart catheterization (RHC) and CMR scanning within one week at the baseline. CMR was performed on a 1.5 T scanner (MAGNETOM Avanto, Siemens Healthcare, Erlangen, Germany). Breath-hold short-axis cine images encompassing the whole left ventricle (LV) and RV from apex to base were acquired using balanced steady-state free-precession (bSSFP) sequence (repetition time/echo time, 3.2 ms/1.6 ms; temporal resolution, 34 ms; flip angle, 60 degrees; field of view, 280 x 340 mm2; matrix, 150 x 256; voxel size, 1.9mm x 1.3mm; slice thickness, 8 mm). Acquired CMR images were analyzed using a prototype software (Trufi Strain V2.1, Siemens Healthcare, Princeton, USA). This software uses a deformation registration algorithm to calculate the myocardial strain on a pixel basis, which could be used to analyze the layer-specific strain and strain rate based on cine CMR (DRA-CMR). In this research, RV Peak Strain, Peak Systolic Strain Rate (SSR), Peak Early Diastolic Strain Rate (DSRE), Peak Late Diastolic Strain Rate (DSRL) in the radial, circumferential and longitudinal direction were studied at three layers [endocardial wall (ew), middle wall (mw) and epicardial wall (epiw)] and the whole RV myocardium. The representative radial strain and strain rate analysis results were shown in figure 1.Results
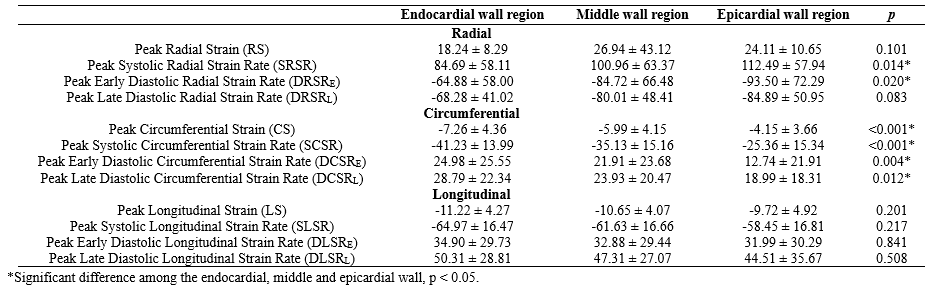
Eighty-two newly-diagnosed PAH patients were enrolled and the median follow-up time was 2014 days (range from 26 to 3990 days). Twenty-nine (35.37%) patients had all-caused death at the end of this study.In the radial direction, obvious transmural gradients were found in Peak Systolic Radial Strain Rate (SRSR, ew: 84.69 ± 58.11%, mw: 100.96 ± 63.37%, epiw: 112.49 ± 57.94%, p = 0.014) and Peak Early Diastolic Radial Strain Rate (DRSRE, ew: -64.88 ± 58.00%, mw: -84.72 ± 66.48%, epiw: -93.50 ± 72.29%, p = 0.020) within RV. In the circumferential direction, there were incremental transmural gradients in Peak Circumferential Strain (CS, ew: -7.26 ± 4.36 %, mw: -5.99 ± 4.15 %, epiw: -4.15 ± 3.66 %, p < 0.001), Peak Systolic Circumferential Strain Rate (SCSR, ew: -41.23 ± 13.99 %, mw: -35.13 ± 15.16 %, epiw: -25.36 ± 15.34 %, p < 0.001), Peak Early Diastolic Circumferential Strain Rate (DCSRE, ew: 24.98 ± 25.55 %, mw: 21.91 ± 23.68 %, epiw: 12.74 ± 21.91 %, p = 0.004) and Peak Late Diastolic Circumferential Strain Rate (DCSRL, ew: 28.79 ± 22.34 %, mw: 23.93 ± 20.47 %, epiw: 18.99 ± 18.31 %, p = 0.012) from epicardial to endocardial walls. However, in the longitudinal direction, no obviously homogeneous transmural gradients were found among three layers (Table 1).
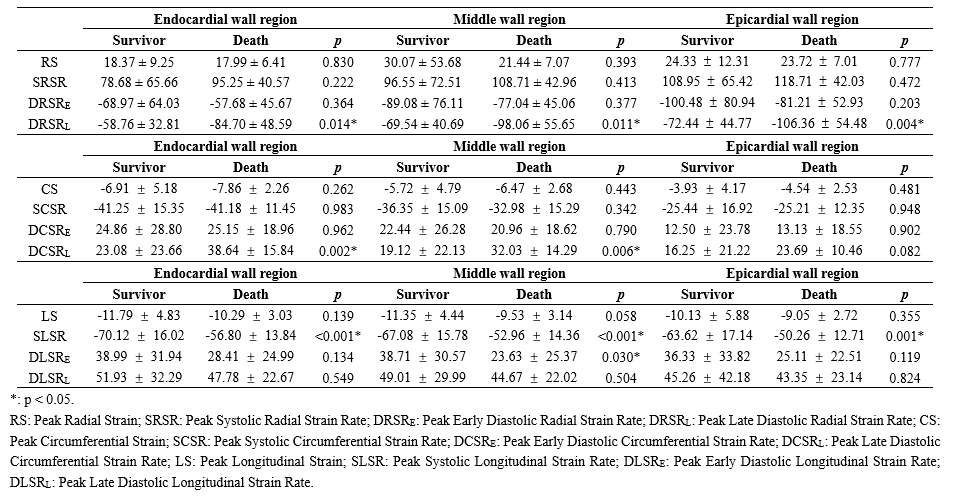
In survivors, obvious increasing transmural gradients from epicardial to endocardial wall were found in CS, SCSR and DCSRE (Table 2). However, in deceased patients, besides the consistent increasing transmural gradients in CS and SCSR, a descending transmural gradient in Peak Radial Strain (RS) and an increasing transmural gradient in DCSRL were also found.
Discussion
When the RV is overloaded, the orientation of the RV free wall changes from a longitudinal to a lateral direction2, resulting in RV more dependent on transverse wall movement3. In the present study, we found long-term deceased patients had a distinct descending transmural gradient in Peak Radial Strain and an obvious increasing transmural gradient in DCSRL from epicardial to endocardial wall. We speculated that the changes of Peak Radial Strain and DCSRL distribution patterns in RV layers might indicate the existence of RV dysfunction at the baseline.Conclusion
DRA-CMR could detect transmural gradients of RV circumferential strain and strain rate in PAH patients, which may help to early detect the existence of RV dysfunctionAcknowledgements
This study was supported by grants from National Key Research and Development Program of China (No. 2016YFC1304400) and Youth Found of Fuwai Hospital (Grant number: 2022-FWQN06).References
1. Quan, R. Characteristics , goal-oriented treatments and survival of pulmonary arterial hypertension in China : Insights from a national multicentre prospective registry. 1–12 (2022) doi:10.1111/resp.14247.
2. Pettersen, E. et al. Contraction Pattern of the Systemic Right Ventricle. Shift From Longitudinal to Circumferential Shortening and Absent Global Ventricular Torsion. J. Am. Coll. Cardiol. 49, 2450–2456 (2007).
3. Kind, T. et al. Right ventricular ejection fraction is better reflected by transverse rather than longitudinal wall motion in pulmonary hypertension. J. Cardiovasc. Magn. Reson. 12, 1–11 (2010).
4. Trip, P. et al. Clinical relevance of right ventricular diastolic stiffness in pulmonary hypertension. Eur. Respir. J. 45, 1603–1612 (2015).
Figures
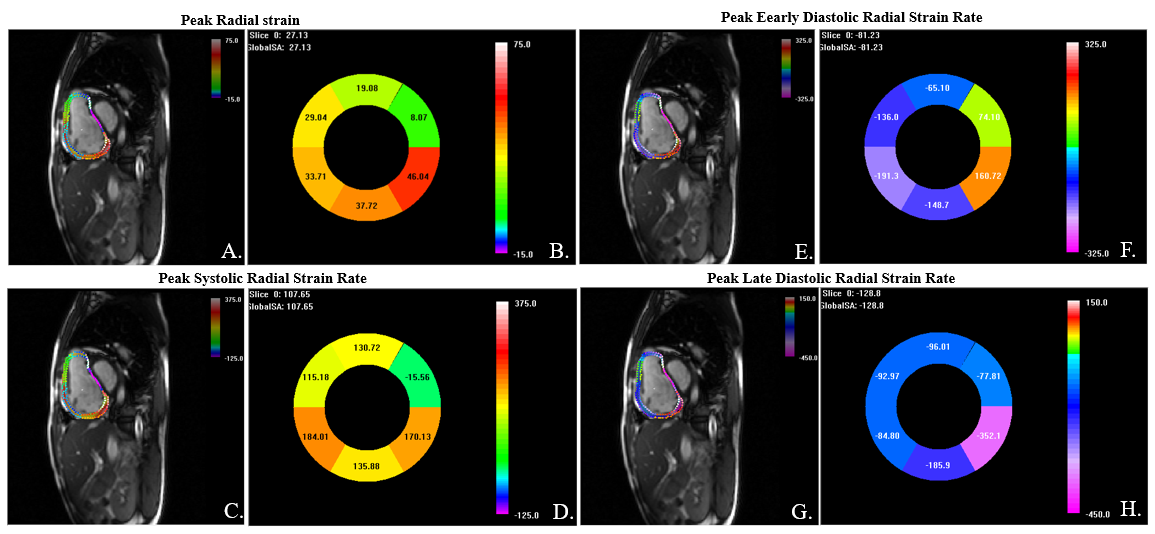
Figure 1. RV layer-specific radial strain and strain rate analysis by DRA-CMR.
The Trufi-strain software would track the endocardial and epicardial contours throughout a cardiac cycle automatically and divided the myocardium into three layers. Strain and strain rate values are shown in situ on three layers (A, C, E, G). Strain and strain rate values of six segments are shown in the “Bull’s eye” (B, F, D, H).