0338
Combination of irregular pulsation and aneurysm wall enhancement improved the diagnostic efficiency of symptomatic intracranial aneurysm1Ren ji Hospital, School of Medicine, Shanghai Jiaotong University, Shanghai, China, 2University of Washington, Seattle, WA, United States
Synopsis
Keywords: Vessels, Vessels
Both aneurysm wall enhancement (AWE) and irregular pulsation have been suggested as potential candidates for intracranial aneurysms (IAs) instability. However, no studies have compared irregular pulsation and AWE for evaluation symptoms in unruptured IAs. By using vessel wall MRI and four-dimensional computed tomography angiography, we found combination of aneurysm wall enhancement and irregular pulsation improve the diagnostic efficiency of symptomatic intracranial aneurysm compared with irregular pulsation or AWE alone. Further longitudinal studies are needed to validate the role of the two imaging markers in predicting aneurysm growth and rupture.INTRODUCTION
Intracranial aneurysms (IAs) are relatively common life-threatening diseases with a prevalence of 3%-5% in adults. Evaluation and stratification of aneurysm rupture risk is still clinical challenging. It is important to identify novel indicators that may improve the current risk assessment of IAs. Recent studies suggested aneurysm wall enhancement (AWE) as identified by contrast-enhanced vessel wall MRI (VWMRI) more frequently observed in unstable (ruptured, symptomatic, or growing) rather than in stable (asymptomatic or nonevolving) IAs. Another potential novel imaging feature of aneurysm vulnerability is irregular pulsation detected by four-dimensional CT angiography (4D-CTA) with electrocardiographic gated reconstruction, possibly arising from a focal weakening of the aneurysm wall and can lead to aneurysm rupture or growth. This study aims to investigate the relationship between irregular pulsation and AWE, and compare their diagnostic advantages in symptomatic IAs in a larger cohort of patients using comprehensive and multivariate analysis.METHODS
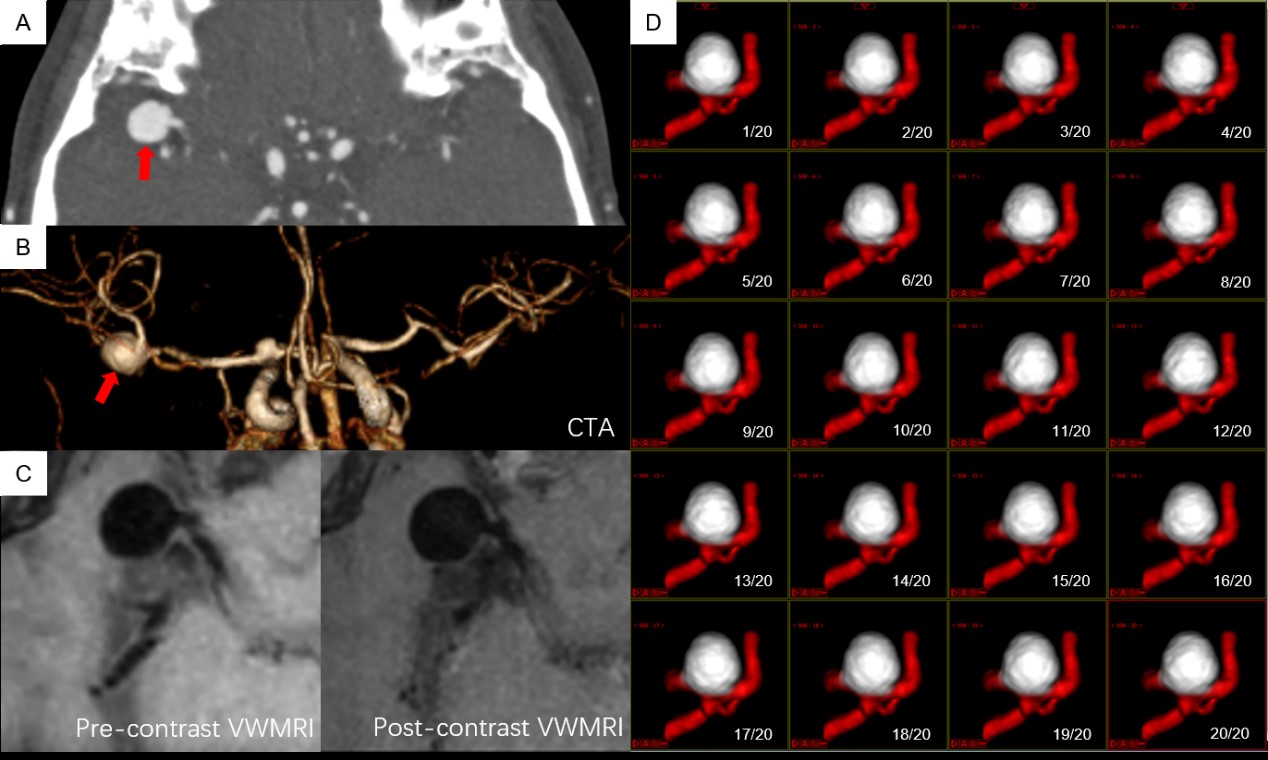
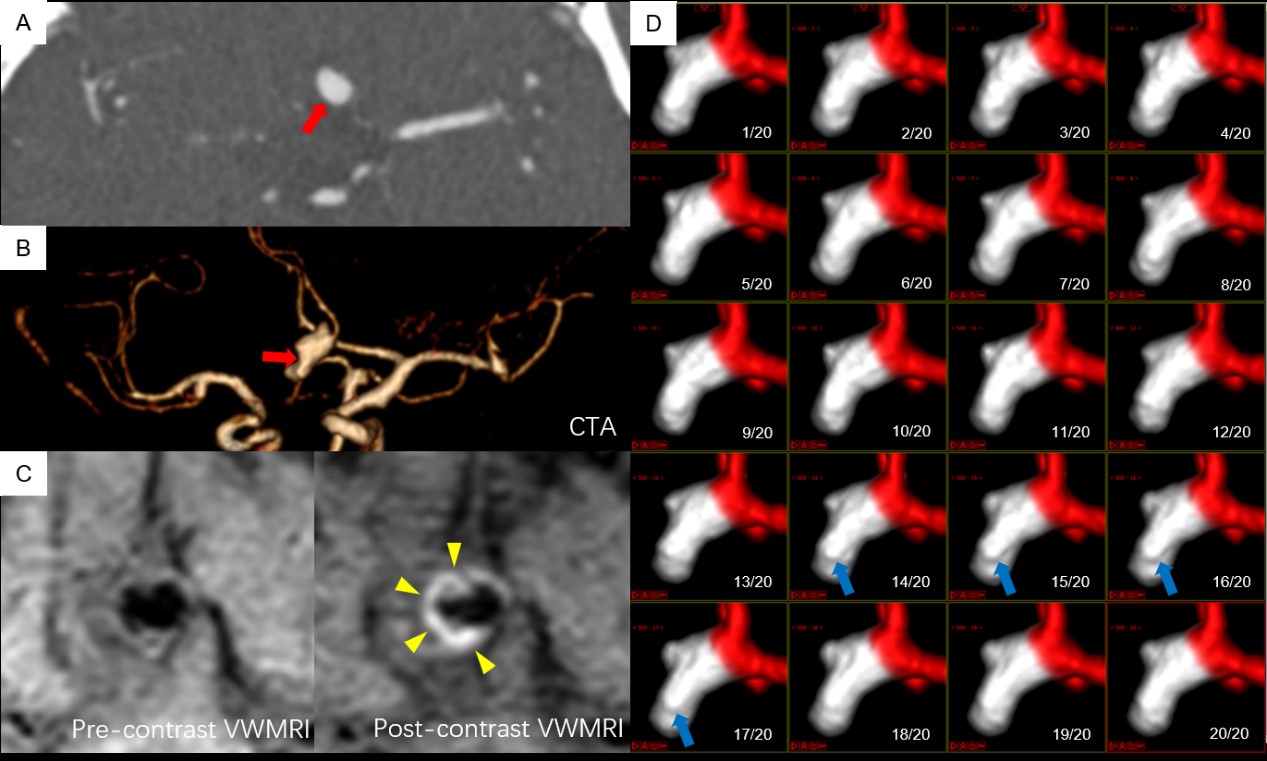
This retrospective study included consecutive patients with IAs who underwent 4D-CTA and VW-MRI between January 2017 to July 2021. 4D-CTA was performed on a 320-detector row CT scanner (Aquilion ONE VISION, Canon Medical System Corporation, Otawara, Japan). Vessel wall MRI was performed on a 3.0T MR scanner (Prisma, Siemens Healthcare or Ingenia, Philips Healthcare or Prisma). The imaging protocols for MR scanning on Ingenia and Prisma were as follows respectively: 1) T1WI volume isotropic turbo spin-echo acquisition (T1-VISTA) sequence with following parameters: TR/TE 800/20msec, number of slices 80, field of view 250mm×162mm, voxel size 0.6mm×0.6mm×0.6mm, acquisition matrix 416×269, and scan time 5 minutes 2 seconds. 2) T1-weighted 3D black-blood fast spin echo with variable flip angle trains (SPACE) sequence with following parameters: TR/TE 1000/15msec, number of slices 240, field of view 193mm× 193mm, voxel size 0.6mm× 0.6mm× 0.6 mm, acquisition matrix 320× 320, and scan time 9 minutes 13 seconds. Post-contrast VW-MRI sequence was acquired 5 minutes after Gadolinium-based contrast agent (Magnevist, Bayer Healthcare, Berlin, German) injection (with a dose of 0.1 mmol/kg, at a rate of 1.5ml/s). Geometric and morphologic parameters were measured and the presence of irregular pulsation (defined as a temporary focal protuberance ≥1 mm on more than three successive frames) was identified on 4D-CTA movies. AWE was estimated on VW-MRI and classified as 4 grades (grade 0 for none or questionable focal trace enhancement, grade 1 for focal thick [<1mm] enhancement, grade 2 for thin [maximum thickness, ≤1 mm] circumferential wall enhancement, or grade 3 for thick [maximum thickness, ≥1 mm] circumferential wall enhancement). Quantitative aneurysm wall enhancement was analyzed by wall enhancement index (WEI). $$WEI=(〖SI〗_(wall-post)/〖SI〗_(CSF-post) -〖SI〗_(wall-pre)/〖SI〗_(CSF-pre) )/(〖SI〗_(wall-pre)/〖SI〗_(CSF-pre) )$$ where “pre” indicated pre-contrast, “post” indicated post-contrast and CSF indicated cerebrospinal fluid.RESULTS
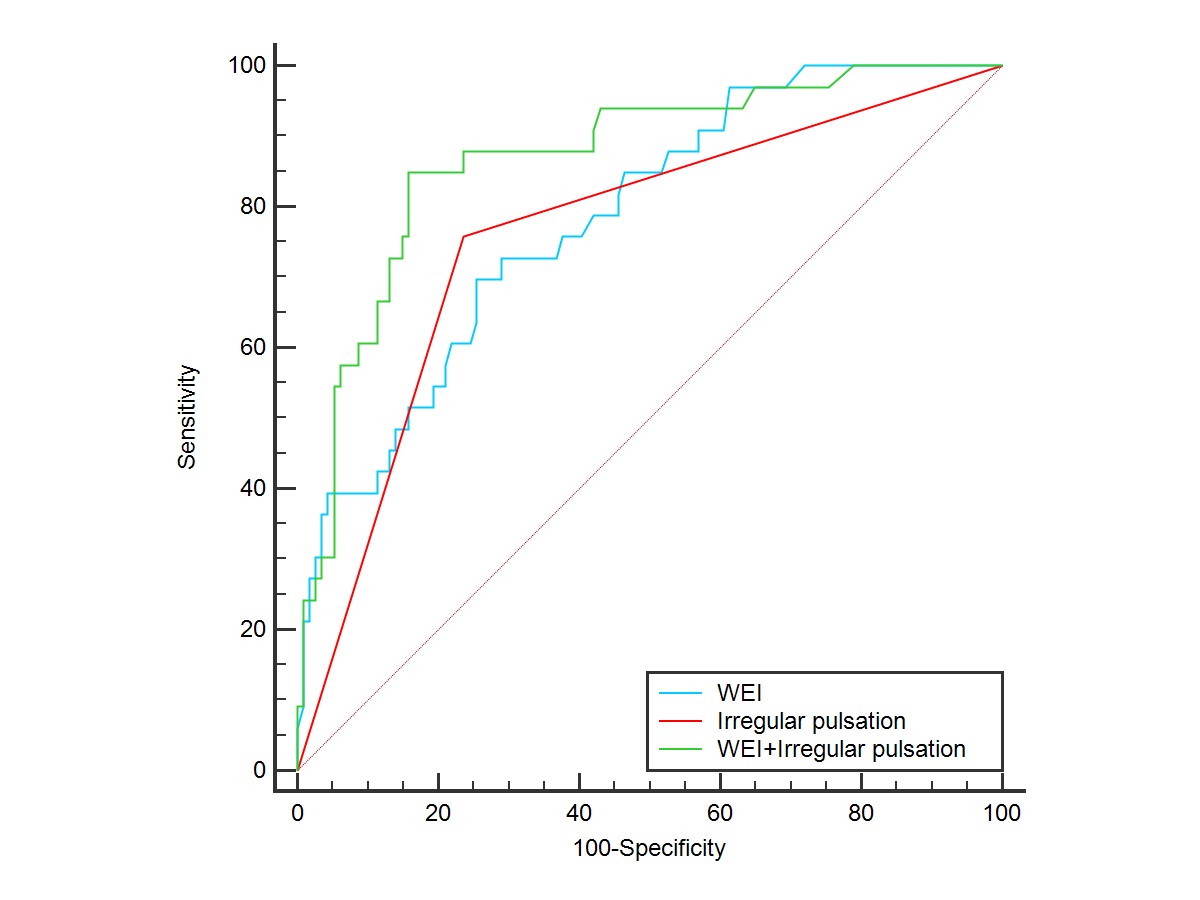
One hundred and thirty-two patients with 147 aneurysms, including 114 asymptomatic and 33 symptomatic aneurysms were included in the study. The prevalence of irregular pulsation was much higher in the symptomatic aneurysms compared to the asymptomatic group (75.8% vs. 23.7%, P <0.001). Asymptomatic IAs more frequently did not show AWE as compared to symptomatic IAs, and AWE, especially grade 3 was more frequently observed in symptomatic than asymptomatic IAs (both P <0.001). Symptomatic IAs had significantly higher WEI than asymptomatic aneurysms (median [interquartile range], 0.8 [0.4–1.9] versus 0.2 [0.1–0.6], P <0.001). The combination of irregular pulsation and WEI achieved the highest AUC of 0.87, with optimized sensitivity of 84.8% and specificity of 84.2% compared with irregular pulsation or WEI alone (P =0.01 and P <0.001, respectively).DISCUSSION
Recent studies showed both aneurysm wall enhancement as identified by VWMRI and irregular pulsation detected by 4D-CTA were promising for identification of unstable aneurysms and they are gaining increasing attention. Aneurysm wall enhancement possibly indicates vasa vasorum which is an indirect marker of inflammation. Persistent inflammation of aneurysm wall involves increased elastic lamina breakdown and may thereby cause focal weakening of the wall, perhaps explaining the formation of irregular pulsation. These two different imaging characteristics of aneurysm instability may be linked or complementary to each other. The combination of irregular pulsation and aneurysm wall enhancement improved the reliability of the identification of symptomatic aneurysms with a higher AUC than each factor in isolation.CONCLUSION
Combination of irregular pulsation and aneurysm wall enhancement improve the diagnostic efficiency of symptomatic intracranial aneurysm. These two imaging markers should be validated in future longitudinal studies for their values in predicting aneurysm growth and rupture.Acknowledgements
No acknowledgement found.References
1 Hackenberg, K. A. M., Hänggi, D. and Etminan, N., Unruptured Intracranial Aneurysms, STROKE, 2018, 49: 2268-2275.
2 Fu, Q., Wang, Y., Zhang, Y., Zhang, Y., Guo, X., Xu, H., Yao, Z., Wang, M., Levitt, M. R., Mossa-Basha, M., Zhu, J., Cheng, J., Guan, S. and Zhu, C., Qualitative and Quantitative Wall Enhancement on Magnetic Resonance Imaging Is Associated With Symptoms of Unruptured Intracranial Aneurysms, STROKE, 2021, 52: 213-222.
3 Shimonaga, K., Matsushige, T., Ishii, D., Sakamoto, S., Hosogai, M., Kawasumi, T., Kaneko, M., Ono, C. and Kurisu, K., Clinicopathological Insights From Vessel Wall Imaging of Unruptured Intracranial Aneurysms, STROKE, 2018, 49: 2516-2519.
4 Zhang, J., Li, X., Zhao, B., Zhang, J., Sun, B., Wang, L., Tian, J., Mossa-Basha, M., Kim, L. J., Yan, J., Wan, J., Xu, J., Zhou, Y., Zhao, H. and Zhu, C., Irregular pulsation of aneurysmal wall is associated with symptomatic and ruptured intracranial aneurysms, J NEUROINTERV SURG, 2022: 2021-18381.
5 Zhang, J., Li, X., Zhao, B., Zhang, J., Sun, B., Wang, L., Ding, S., Liu, X., Yan, J., Mossa-Basha, M., Liu, X., Wan, J., Zhao, H., Xu, J. and Zhu, C., Irregular pulsation of intracranial unruptured aneurysm detected by four-dimensional CT angiography is associated with increased estimated rupture risk and conventional risk factors, J NEUROINTERV SURG, 2021, 13: 854-859.
6 Edjlali, M., Guédon, A., Ben Hassen, W., Boulouis, G., Benzakoun, J., Rodriguez-Régent, C., Trystram, D., Nataf, F., Meder, J., Turski, P., Oppenheim, C. and Naggara, O., Circumferential Thick Enhancement at Vessel Wall MRI Has High Specificity for Intracranial Aneurysm Instability, RADIOLOGY, 2018, 289: 181-187.
7 Zhong, W., Su, W., Li, T., Tan, X., Chen, C., Wang, Q., Wang, D., Su, W. and Wang, Y., Aneurysm Wall Enhancement in Unruptured Intracranial Aneurysms: A Histopathological Evaluation, J AM HEART ASSOC, 2021, 10.
Figures