0299
On-site construction of a point-of-care low-field MRI system in Africa
Johnes Obungoloch1, Ivan Muhumuza1, Wouter Teeuwisse2, Joshua Harper3, Martin van Gijzen4, Steven Schiff5, Andrew Webb2, and Thomas O'Reilly2
1Mberara University of Science and Technology, Mberara, Uganda, 2Leiden University Medical Center, Leiden, Netherlands, 3Universidad Paraguayo Alemana, Asuncion, Paraguay, 4Delft Institute of Applied Mathematics, Delft, Netherlands, 5Yale University, New Haven, CT, United States
1Mberara University of Science and Technology, Mberara, Uganda, 2Leiden University Medical Center, Leiden, Netherlands, 3Universidad Paraguayo Alemana, Asuncion, Paraguay, 4Delft Institute of Applied Mathematics, Delft, Netherlands, 5Yale University, New Haven, CT, United States
Synopsis
Keywords: Low-Field MRI, Low-Field MRI
Point-of-care (POC) low-field MRI systems have a large potential to increase the accessibility and sustainability of MRI in low- and middle-income countries (LMICs). An important step in translating scientific developments from high-income countries to LMICs is technology that can be assembled or constructed locally. We describe the construction and testing of a POC system on site in Africa. All components to assemble a 50 mT Halbach magnet based system, together with the necessary tools, were air-freighted from The Netherlands to Uganda. With four instructors and six untrained personnel, the complete project from delivery to first image took approximately 11 days.Introduction
The lack of MRI facilities, both clinical and research, in the African continent has been highlighted in several recent articles (1-3). In (3) four crucial challenges were highlighted: access and availability, personnel training and education, research capacity and sustainable technology. One approach that can potentially address many of these recommendations is low-field MRI. In order to fulfill these requirements, the system must be designed to be affordable, but equally importantly to be understandable and repairable by, for example, local medical physicists and/or electricians. In September 2022, a team of researchers from the Netherlands and Paraguay worked with local students and professionals at the Mbarara University of Science and Technology (MUST) to construct, on site, the first custom-built point-of-care MRI system in Africa. This work addresses the question of how does one, in a practical manner, attempt to reproduce academic developments in the area of low-field MRI design and construction (4-6) into a practical product which can be manufactured and assembled on-site, in this case in Uganda. Logistics, training, knowledge transfer, and infrastructural capabilities are the focus of this paper, rather than device optimization and design as in standard publications. We aim to give a realistic assessment of the challenges in transferring knowledge from high-resource to lower-resource environments.Construction and testing
Shipped components for magnet construction were twenty-five PMMA rings produced via a computerized numerical control (CNC) mill, M4 and M5 threaded brass rods (length 382 and 504 mm, respectively), brass nuts and washers (M3, M4, M5), fifty 2 mm thick PMMA “lids” for the magnet rings, glue, and 4089 12 x 12 x 12 mm3 NdFeB N-48 magnets. On a practical level one should bear in mind that facilities for delivery after shipping may be somewhat limited. As an example, the 325 kg crate was delivered with a van that could just accommodate it, as shown in Figure 1, and did not have a hydraulic lift. Because a fork lift was not available on site we ended up opening the crate in the back of the van at night and carrying out items one piece at a time into the laboratory. The critical steps in magnet construction are ensuring the correct orientations of the thousands of small magnets, and very accurate spacing of the individual rings of mgets, as shown in Figure 2: typical accuracies of 0.05 mm can be achieved using digital or analogue calipers. An open source (https://github.com/LUMC-LowFieldMRI/ GradientDesignTool) was used to obtain three-dimensional wire patterns for the gradient coils. These were printed using PLA formers with thickness 5-6 mm and groove depth 2.7 mm such that coated 2.1 mm2 wire could snugly be placed in the grooves. In order to facilitate modularity the inner y- and z-coils were fabricated in four different quadrants, with the outer x-coil fabricated as two halves, as shown in Figure 3. Approximate printing times using an Raise3D Pro2/3 Plus 3D printer were 5 or 8 days per segment for Z- and Y-gradient or X-gradient respectively. In the laboratory in Uganda, the stages involved in producing the gradient coils were removal of residual plastic in the grooves (1.5 h per segment), placement of insulated wire and supergluing into place (1 hour per segment), as shown in Figure 3. The MR spectrometer used to obtain initial images, Figure 4, was the magnetic resonance control system (MarCos) (14) developed by a consortium of international researchers, details of which are available in open repositories (https://github.com/yvives/PhysioMRI_GUI, https://github.com/vnegnev/marcos_extras/wiki). The three-channel gradient amplifier is an open-source design (https://github.com/LUMC-LowFieldMRI/GradientAmplifier) capable of providing up to ~15 Amps with a peak voltage of 13 V. For the small solenoidal coil, a low power RF amplifier can be used, in this case a Mini-Circuits zx60-100vh+ with a maximum output power of 1 watt. Figure 5 shows an approximate timeline for the build. This is intended as a guide, and should be reconciled with the fact that two instructors were present the entire time, with extensive experience of all aspects of the system construction. Six untrained persons performed the majority of the construction.Discussion
This work shows the feasibility and challenges associated with translating academic advances in point-of-care MRI to locations in which accessibility and sustainability are absolute enabling factors. Rather than simply shipping a finished product, we believe that the fact that the assembly and testing procedures took place entirely on location ensures a much greater transfer of knowledge, and the possibility for this knowledge to be passed on. In addition to being able to fabricate further systems, the ability to adjust, improve and repair such a system is enormously enhanced by the from-ground construction approach. Nevertheless, despite all of the funding, support and organization that went into getting us to this point, there are very substantial challenges that remain to successfully bring such a technology to the point of regulatory approval, health-care evaluation and commercial dissemination. These challenges are heightened within the largely unexplored terrain of open-source technology such as this.Acknowledgements
This work was funded by the National Institutes of Health (2R01HD085853), the Dutch Science Foundation (NWO grants WOTRO Joint SDG Research Programme W 07.303.101, Stevin Preis 14997), and the European Research Council (Horizon 2020 ERC Advanced PASMAR 101021218).References
1. Ogbole GI, Adeyomoye AO, Badu-Peprah A, Mensah Y, Nzeh DA. Survey of magnetic resonance imaging availability in West Africa. Pan Afr Med J 2018;30:240. 2. Geethanath S, Vaughan JT, Jr. Accessible magnetic resonance imaging: A review. J Magn Reson Imaging 2019. 3. Anazodo UC, Ng JJ, Ehiogu B, Obungoloch J, Fatade A, Mutsaerts H, Secca MF, Diop M, Opadele A, Alexander DC, Dada MO, Ogbole G, Nunes R, Figueiredo P, Figini M, Aribisala B, Awojoyogbe BO, Aduluwa H, Sprenger C, Wagner R, Olakunle A, Romeo D, Sun Y, Fezeu F, Orunmuyi AT, Geethanath S, Gulani V, Nganga EC, Adeleke S, Ntobeuko N, Minja FJ, Webb AG, Asllani I, Dako F, Conesortium for Advancement of MRIE, Research in A. A Framework for Advancing Sustainable MRI Access in Africa. NMR Biomed 2022:e4846. 4. de Vos B, Parsa J, Abdulrazaq Z, Teeuwisse WM, Van Speybroeck CDE, de Gans DH, Remis RF, O'Reilly T, Webb AG. Design, Characterisation and Performance of an Improved Portable and Sustainable Low-Field MRI System. Front Phys-Lausanne 2021;9. 5. O'Reilly T, Teeuwisse WM, de Gans D, Koolstra K, Webb AG. In vivo 3D brain and extremity MRI at 50 mT using a permanent magnet Halbach array. Magn Reson Med 2021;85(1):495-505. 6. Guallart-Naval T, Algarin JM, Pellicer-Guridi R, Galve F, Vives-Gilabert Y, Bosch R, Pallas E, Gonzalez JM, Rigla JP, Martinez P, Lloris FJ, Borreguero J, Marcos-Perucho A, Negnevitsky V, Marti-Bonmati L, Rios A, Benlloch JM, Alonso J. Portable magnetic resonance imaging of patients indoors, outdoors and at home. Sci Rep-Uk 2022;12(1).Figures

(left)
Crate containing all components including assembly tools, overall size 1.2 x
1.0 x 0.8 m and weight 325 kg. (center) Final delivery after two weeks en route
via taxi from the closest airport 5 hours away. (right) Illustration of
individual plastic rings for the magnet.

Magnet
assembly. (left) Brass rods are used to align each of the rings of the magnets.
Nuts are used as spacers between each ring. The forces between each ring are
significant but not dangerous. (center) After each ring is threaded onto the
rods, the position of each nut is carefully adjusted so that there is equal
spacing between each of the rings, and they are precisely aligned parallel to
each other. (right) The completed magnet consisting of 25 rings, the central 17
containing two layers of magnets, and the front/back three rings having three
layers.
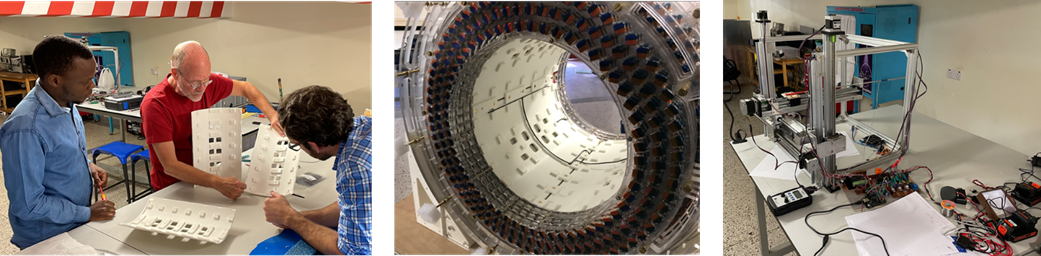
Installation
of gradient set and system characterization.
(left) The design consists of interlocking components which click into
place. (center) Before the final gradient set is inserted the wiring that
connects the two halves and the gradient amplifier is installed. (right) After
installation of the gradients a 3D robot is used to map the magnetic field.
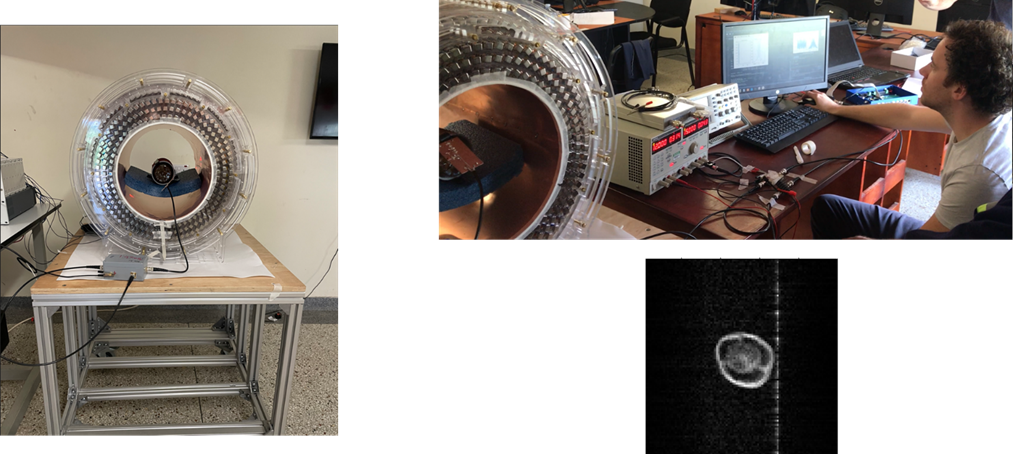
Completed
system, with 10 cm diameter RF solenoidal coil placed in the center and a bell
pepper used as the sample. A Marcos open-source console is used to acquire the
data, with a small low-power minicircuits amplifier used for the RF. The first
image, showing a zipper artifact to illustrate that the data are real!
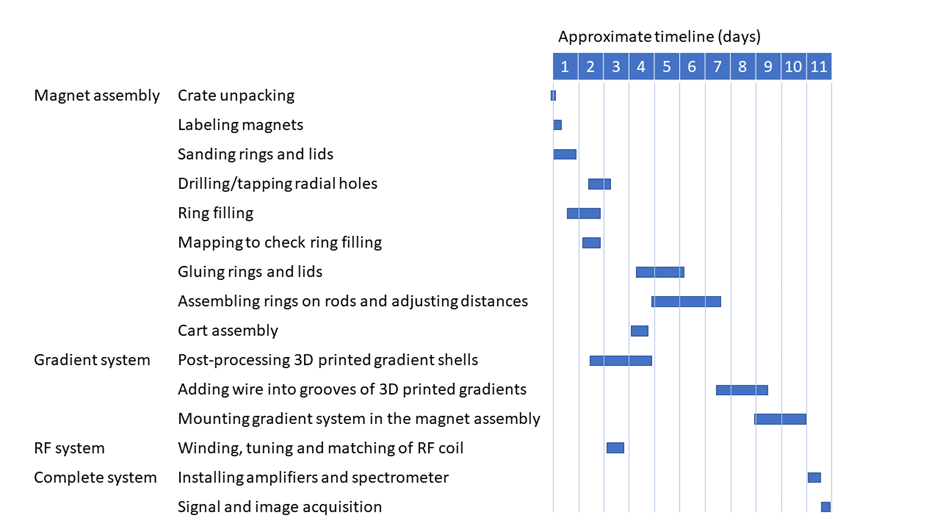
Approximate
time-line for the build in Uganda, with four instructors and six students –
work days were ~10 hours per day with 1-2 hours per day taken up by
instruction.
DOI: https://doi.org/10.58530/2023/0299