0192
High-resolution DWI in the breast by Spatiotemporal encoding (SPEN): clinical utility in comparison with SS-EPI and RESOLVE1Kyoto University Faculty of Medicine, Kyoto, Japan, 2Diagnostic Imaging and Nuclear Medicine, Kyoto University Graduate School of Medicine, Kyoto, Japan, 3Institute for Advancement of Clinical and Translational Science (iACT), Kyoto University Hospital, Kyoto, Japan, 4Diagnostic Radiology, Kansai Electric Power Hospital, Osaka, Japan, 5Siemens Healthcare K.K., Tokyo, Japan, 6Chemical and Biological Physics, Weizmann Institute of Science, Rehovot, Israel, 7Radiology, Sheba-Medical-Center, Ramat-Gan, Israel, 8Tenri Hospital, Nara, Japan, 9Breast Surgery, Kyoto University Hospital, Kyoto, Japan
Synopsis
Keywords: Breast, Breast
This study investigated the breast lesion conspicuity and ADC reliability for 3 different DWI protocols; SPEN, SS-EPI, and RESOLVE. The in-plane resolution for SPEN and RESOLVE was 1x1mm2, and SS-EPI was 2x2mm2. SPEN showed a higher score for lesion conspicuity than SS-EPI, and a lower score than RESOLVE. ADC values in breast lesions were significantly lower in SPEN than others, presumably due to the choice of different b values, the sequences having different T1/T2 weightings, different robustness vs motions, the presence of unsuppressed fat, or different viewer systems used to analyze the data, which will need further investigation.Introduction
Dynamic contrast (DCE) MRI has been a standard method for diagnosing breast lesions. Diffusion-weighted imaging (DWI) has been widely used to improve its diagnosis, and international efforts have been made to standardize breast DWI (1). Single-shot echo-planar imaging (EPI) is the most standard technique in these DWI studies, as it can avoid motion related phase inconsistencies associated with multi-shot data. However, distortions induced along the phase-encoding (PE) direction by susceptibility and fat/water artifacts, might appear if performing breast DWI with high resolution. Recently, spatiotemporal encoding (SPEN) DWI techniques have been proposed to overcome this (2). SPEN allows one to adjust the PE bandwidth (BW) to deal with image distortions; in conjunction with self-referenced phase corrections in interleaved acquisitions, this can significantly reduce the images’ distortions. SPEN has been shown to provide a reliable characterization of breast cancer with improved distortions at sub-millimeter resolutions (3). Herein we investigated the breast lesion conspicuity and ADC reliability for 3 different DWI protocols: SS-EPI (conventional DWI), SPEN, and RESOLVE (readout segmentation of long variable echo-trains: Readout segmented EPI).Materials & Methods
This prospective study was approved by the institutional review board of Kyoto University hospital, and included 65 women who were suspected of breast tumors. Forty-seven lesions were further analyzed (37 malignant, ten benign). Breast MRI was performed using a 3-T system (MAGNETOM Prisma, Siemens) equipped with a dedicated 18-channel breast array coil. Three different types of diffusion-weighted images were acquired, and the detailed information is shown in Table 1. SPEN scans were post processed off line, using Matlab-based packages (https://www.weizmann.ac.il/chembiophys/Frydman_group/software).Quantitative evaluation: A dedicated breast phantom with five different test substances covering the range of ADC values exhibiting typical malignant and benign breast lesions was prepared and scanned (4) and the ADC values were measured. ADC values for the three different DWI protocols in Table 1, were measured in all 47 lesions.
Qualitative evaluation: Three breast radiologists evaluated lesion conspicuity using the semi-quantitative score, ranging from 4 (excellent) to -0 (not visible), and modified BI-RADS lexicon for breast DWI based on lesion morphology and distribution was also assessed (5). Inter-observer agreement regarding BI-RADS lexicons was calculated by using kappa statistics. ADC values or scores between different DWI protocols were compared using the Wilcoxon test with Bonferroni correction. Statistical analyses were performed using MedCalc Software, Mariakierke, Belgium.
Results
Figure 1 (left) demonstrates the ADC values arising from SPEN, SS-EPI, and RESOLVE in the breast phantom, showing no differences in the measured ADC values for the different DWI sequences. Figure 1 (right) summarizes the ADC values measured in all lesions; ADC values arising from SPEN were significantly lower than those from SS-EPI or RESOLVE (p<0.01).A representative breast cancer case analyzed by SPEN, SS-EPI, and RESOLVE DWI sequences is shown in Figure 2. The morphology of the cancer tumor is clearly delineated in SPEN and RESOLVE, while its contrast is relatively obscure in SS-EPI.
Another representative case of breast cancer (SPEN, SS-EPI, and RESOLVE) is presented in Figure 3. The rim shape of breast cancer is clearly delineated in both SPEN and RESOLVE compared to SS-EPI. RESOLVE shows the irregular margin more in detail than SPEN. This might reflect the onset of saturation in the SPEN scans, leading to a compromise in SNR.
Averaged lesion conspicuity scores provided by three radiologists are shown in Figure 4. The scores were significantly higher in RESOLVE compared to SPEN or SS-EPI (p<0.01, 0.01). The score for SPEN was significantly higher than for SS-EPI (p<0.01).
Agreements for reported DWI lexicons (lesion morphology and distribution) among three readers were fair to substantial (0.34-0.78).
Discussion & Conclusion
This study investigated the breast lesion conspicuity and ADC reliability for 3 different DWI protocols; SPEN, SS-EPI, and RESOLVE. Even though there was no difference in a phantom study, ADC values in breast lesions were significantly lower in SPEN than in SS-EPI or RESOLVE. This ADC difference found in lesions might be due to different b values used in this study (lower ADC values with high b values in general (6)), the sequences having different T1/T2 weightings, different robustness vs motions, or due to the presence of unsuppressed fat; all of these will need further investigation, particularly if ADC thresholds are to be used for lesion classification. In some cases, RESOLVE tended to have better lesion delineation than SPEN in the DWIs; however, this might also be partially due to the different viewer systems used to analyze the data. Previous literature indicates better lesion conspicuity on the K map in SPEN than in SS-EPI (3); further investigation is also required to validate the tendency. Due to time constraints SPEN was only used to collect three slices in this study –almost the same time as required in the SS-EPI analyses, while it took 5 mins for high-resolution RESOLVE. In conclusion: the SPEN sequence provided good characterization of breast tumors with 1x1mm2 in-plane resolution, even in some cases high resolution RESOLVE provided better lesion conspicuity and delineation.Acknowledgements
This work was supported by JSPS KAKENHI Grant Number 21K07618.References
1. Baltzer P, Mann RM, Iima M, Sigmund EE, Clauser P, Gilbert FJ, et al. Diffusion-weighted imaging of the breast-a consensus and mission statement from the EUSOBI International Breast Diffusion-Weighted Imaging working group. Eur Radiol. 2020 Mar;30(3):1436–50.
2. Solomon E, Liberman G, Nissan N, Furman-Haran E, Sklair-Levy M, Frydman L. Diffusion-weighted breast MRI of malignancies with submillimeter resolution and immunity to artifacts by spatiotemporal encoding at 3T. Magn Reson Med. 2020 Sep;84(3):1391–403.
3. Otikovs M, Nissan N, Furman-Haran E, Anaby D, Allweis TM, Agassi R, et al. Diffusivity in breast malignancies analyzed for b > 1000 s/mm2 at 1 mm in-plane resolutions: Insight from Gaussian and non-Gaussian behaviors. J Magn Reson Imaging. 2021 Jun;53(6):1913–25.
4. Iima M, Kataoka M, Honda M, Ohashi A, Ohno Kishimoto A, Ota R, et al. The Rate of Apparent Diffusion Coefficient Change With Diffusion Time on Breast Diffusion-Weighted Imaging Depends on Breast Tumor Types and Molecular Prognostic Biomarker Expression. Invest Radiol. 2021 Aug 1;56(8):501–8.
5. Kishimoto AO, Kataoka M, Iima M, Honda M, Miyake KK, Ohashi A, et al. Evaluation of malignant breast lesions using high-resolution readout-segmented diffusion-weighted echo-planar imaging: Comparison with pathology. Magn Reson Med Sci. 2021 Jun 1;20(2):204–15.
6. Iima M, Partridge SC, Le Bihan D. Six DWI questions you always wanted to know but were afraid to ask: clinical relevance for breast diffusion MRI. Eur Radiol. 2020 May;30(5):2561–70.
Figures
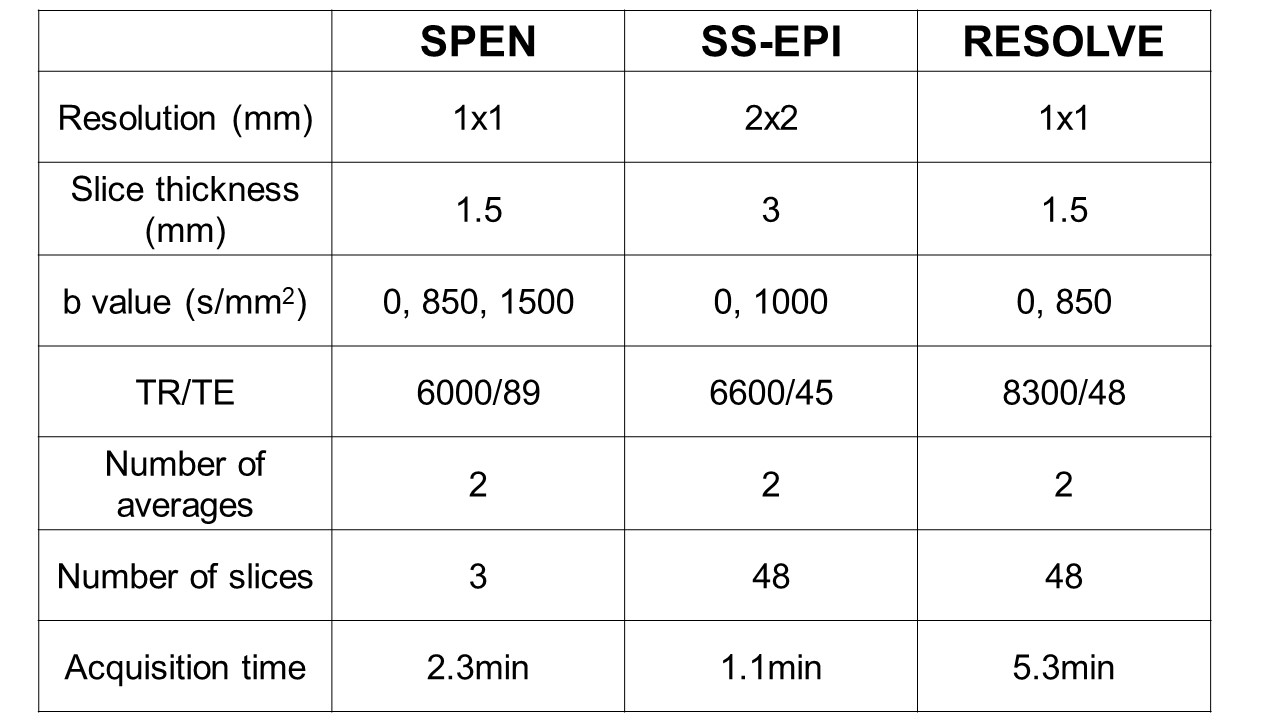
Table 1: 3 different DWI acquisition protocols
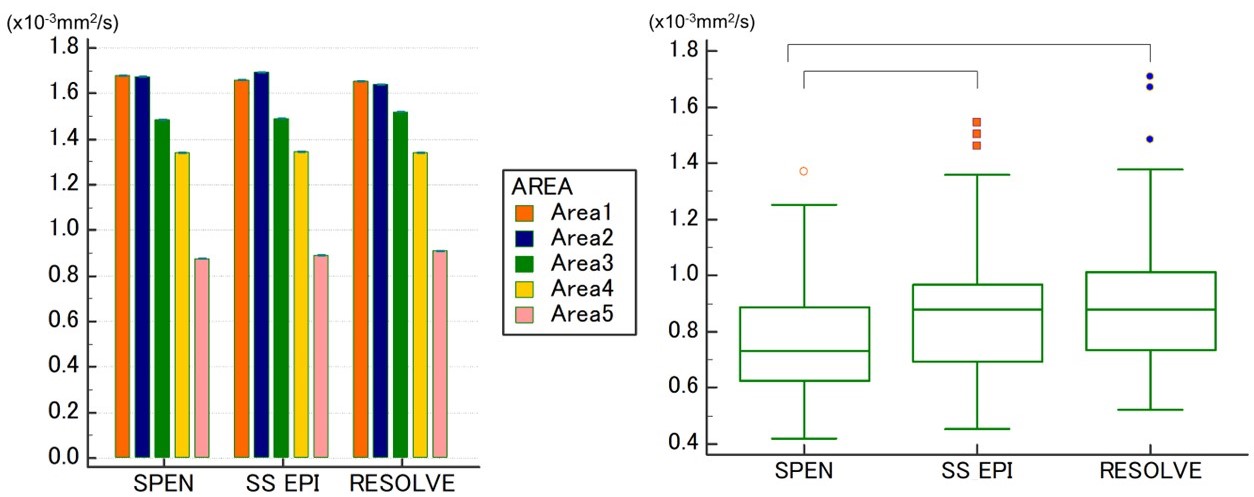
Figure 1: (Left) ADC phantom results showing good agreement among the three tested protocols (Table 1). (Right) Box-and-whisker plot of the ADC values arising in all lesions by the three tested protocols. Results were calculated based on b = 0,850,1500 s/mm2 for SPEN, 0, 1000 s/mm2 for SS-EPI, and 0, 850 s/mm2 for RESOLVE.
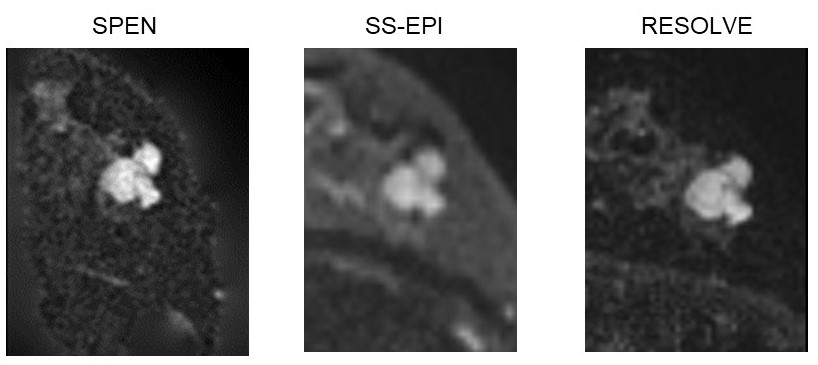
Figure 2: Representative case of breast cancer, as evidenced by DWI scans performed by the indicated sequences using b-values in the 850 s/mm2 for SPEN and RESOLVE, and 1000 s/mm2 for SS-EPI.
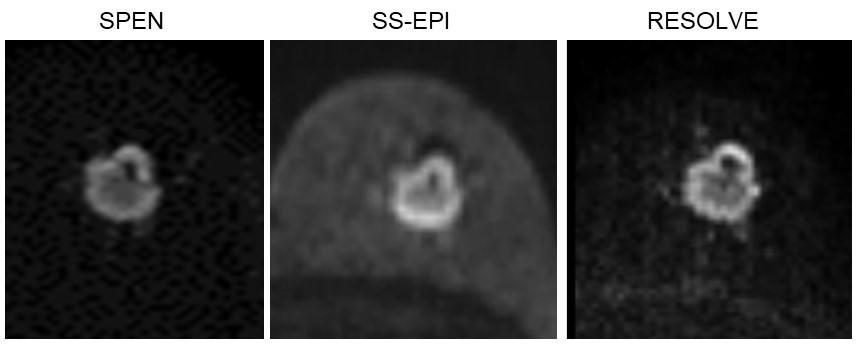
Figure 3: Representative case of a breast cancer evidencing rim enhancement, as scanned by DWI scans performed using the indicated sequences. The parameters were as in Figure 2.
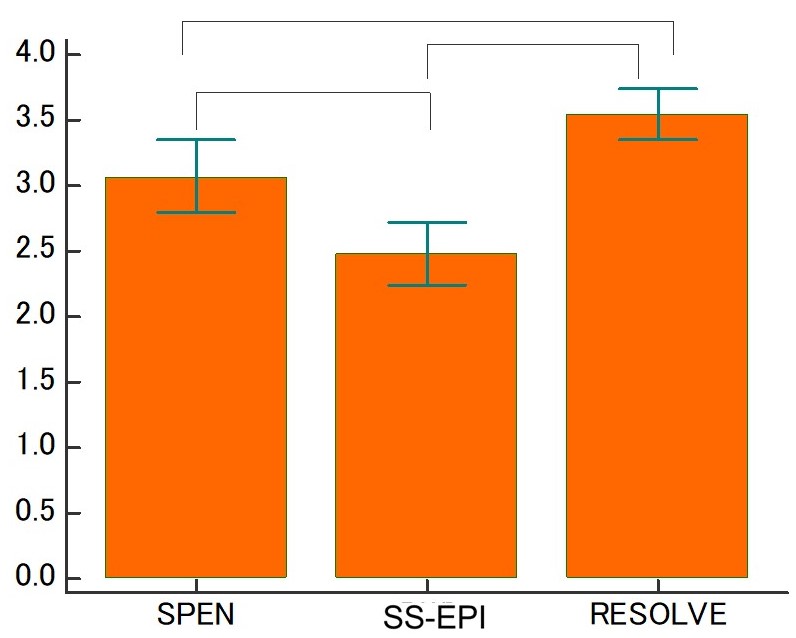
Figure 4: Averaged lesion conspicuity scores by three radiologists. (4 (excellent) to -0 (not visible))