0191
MR conductivity imaging to decrease false-positive biopsy caused by breast ultrasound: comparison with DWI and abbreviated MRI1Radiology, Seoul National University Hospital, Seoul, Korea, Republic of, 2Electrical and Electronic Engineering, Yonsei university, Seoul, Korea, Republic of
Synopsis
Keywords: Breast, Electromagnetic Tissue Properties
We evaluated the role of MRI as a problem-solving tool to reduce false-positive biopsy caused by breast ultrasound. Seventy nine participants underwent MRI prior to ultrasound-guided core needle biopsy. The MRI protocol consisted of T2-weighted imaging for conductivity map reconstruction, diffusion-weighted imaging, and abbreviated contrast-enhanced MRI. The conductivity, ADC, and BI-RADS criterion lowered false-positive biopsy by 23%, 38%, and 43%, respectively, while being able to detect all cancers. Conductivity imaging showed the potential but showed lower performance than diffusion-weighted imaging and abbreviated MRI in reducing unnecessary biopsies caused by breast ultrasound.Introduction
Breast ultrasound (US) can detect mammographically occult breast cancers. Although the cancer detection rate of breast US is lower than that of breast MRI, US is advantageous because of high accessibility and lack of radiation exposure. Based on these advantages, supplemental US is widely used in women with dense breasts. The main limitations of breast US include substantial inter-observer variability and false-positive biopsy1. In this study, we evaluate the role of MRI as a problem-solving tool to reduce false-positive biopsy caused by breast US. We mainly evaluate the role of conductivity imaging as a novel imaging technique. Conductivity imaging is reconstructed using the magnetic resonance electric properties tomography (MREPT) technique, and it reflects the concentration and movement of ions2. Several studies demonstrated the potential of conductivity imaging to differentiate benign and malignant breast lesions, but the previous studies were limited due to small sample sizes and lack of reproducibility3-5. Therefore, the purpose of this study was to evaluate the performance of MR conductivity imaging in reducing false-positive biopsy caused by breast US, in comparison with relatively well-known diffusion-weighted imaging (DWI) and abbreviated MRI.Materials and Methods
In this single center prospective study, we screened women from the biopsy scheduling database from October 2020 to august 2022 who were scheduled for US-guided core needle biopsy for breast lesions with BI-RADS category 4 on breast US. Exclusion criteria were claustrophobia, implant bag insertion status, bilateral mastectomy status, neoadjuvant chemotherapy reception status, lesions 5mm or less on breast US, and refusal of study participation. Breast MRI was performed prior to biopsy using a 3T MRI scanner. The MRI protocol sequentially consisted of nonfat-suppressed T2-weighted turbo spin echo sequence for conductivity map reconstruction, rs-EPI DWI with b=0 and 800s/mm2, and abbreviated MRI with one pre-contrast and one post-contrast T1 sequence. Conductivity was reconstructed with the phase-based MREPT and B1--based coil combination technique. A 25x25 2D kernel and the weighted polynomial fitting technique was used. A breast radiologist with 9 years of experience reviewed MRI without knowing biopsy results. All patients proceeded biopsy regardless of MRI findings, and the biopsy results were the reference standards. Two measurement methods were used for conductivity analysis: a whole 2D region-of-interest (ROI) method drew ROIs on all images that lesions are seen, and a single 2D ROI method drew a ROI on one image with the largest lesion diameter. Using the matlab interface, ROIs were manually drawn on T2-weigthed images or contrast-enhanced T1-weighted images. The ROIs were automatically propagated to the conductivity maps. The maximum and mean conductivity values within the ROIs were recorded. For the ADC measurement, the hotspot method recommended by the EUSOBI guideline was used6. A small round ROI was drawn on the darkest part of the tumor while avoiding cystic or necrotic portions, or normal parenchyma. On abbreviated MRI, BI-RADS category was assessed according to the ECOG-ACRIN 1141 guideline7. Conductivity and ADC parameters of benign and malignant breast lesions were compared using the Mann-Whitney U test and areas under the ROC curves. The performance of each MRI protocol in reducing false-positive biopsy were evaluated using the following hypothetical criteria: lowest conductivity value, highest ADC value amongst malignant breast lesions, and BI-RADS category 2 or 3 on abbreviated MRI.Results
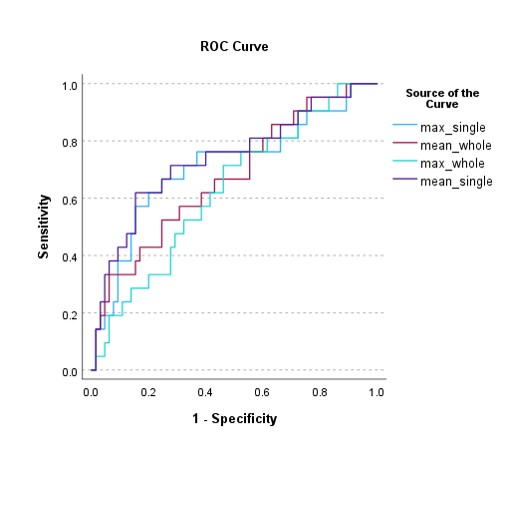
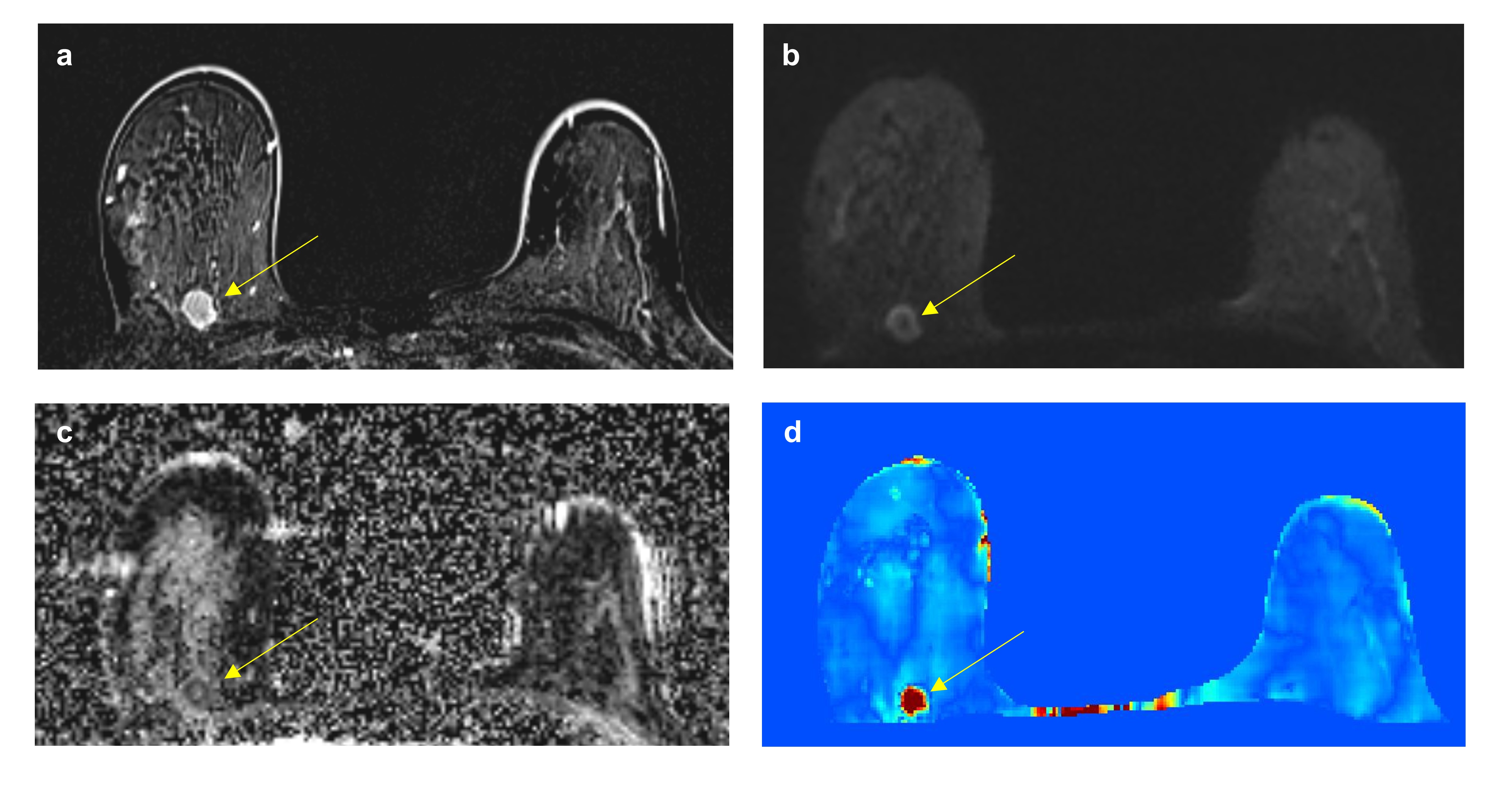
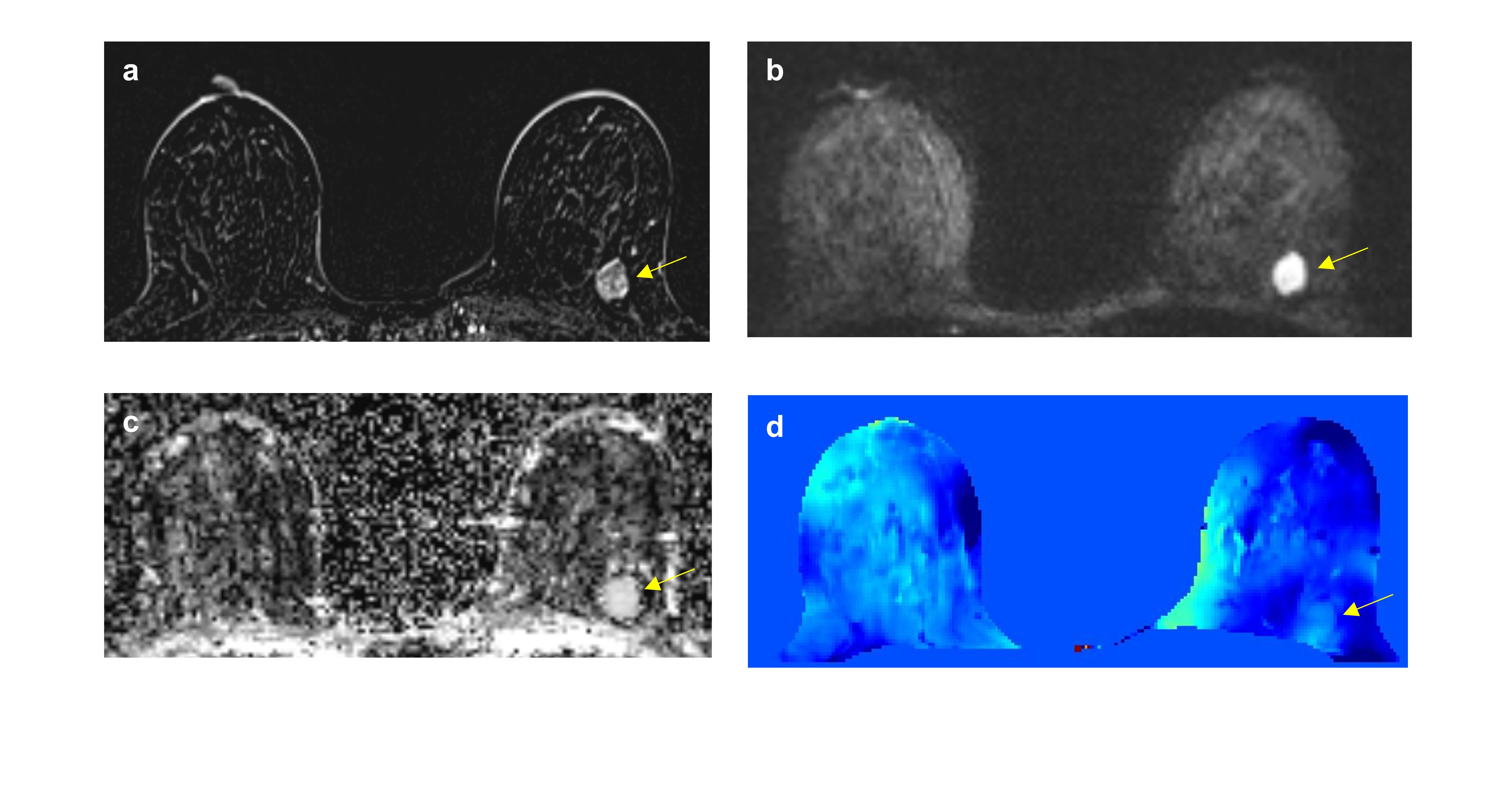
The total number of study participants were 79, and the number of breast lesions were 86. The median age was 44 years (ranges, 21-71), and the median breast lesion size on US was 2cm. 21 cancers were detected in study participants, where 16 were invasive ductal carcinoma and 5 were ductal carcinoma in situ. Both maximum and mean conductivity values obtained from the whole ROI demonstrated higher values in malignant than benign lesions (Fig 1a-b). This was also true for the single ROI method (Fig 1c-d). When comparing AUCs among the conductivity parameters, mean conductivity of the single ROI showed the highest AUC of 0.74 (Fig 2). Therefore, in the subsequent analyses, we used this mean conductivity obtained from the single ROI. ADC showed significantly lower values in malignant than benign lesions (Fig 1e). AUC of ADC was 0.89, which was higher than that of mean conductivity, although it did not reach a statistically significant level (0.89 vs 0.74, P = 0.05). On abbreviated MRI, all 21 cancers were correctly assessed as BI-RADS category 4 or 5. 43% (28/65) of benign lesions were correctly assessed as BI-RADS 2 or 3, but 57% (37/65) were still considered suspicious. The hypothetical criteria lowered false-positive biopsy while being able to detect all cancers (Fig 3). The conductivity (< 0.105S/m), ADC (> 1.59x10-3 mm2/s), and BI-RADS 2 or 3 criterion lowered false-positive biopsy by 23% (15/65), 38% (25/65), and 43% (28/65), respectively (Fig 4).Conclusion
Our study confirms excellent performances of DWI and abbreviated MRI in reducing unnecessary biopsies caused by breast US. Conductivity imaging shows the potential but shows lower performance than DWI and abbreviated MRI. If conductivity imaging is to be used in actual future clinical practice, more efforts should be made to develop an automated reconstruction process similar to ADC mapping and to overcome technical limitations such as low signal-to-noise ratio, boundary artifacts, and chemical shift artifacts.Acknowledgements
This study was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2020R1F1A1074903).References
1. Lee JM, Arao RF, Sprague BL, et al. Performance of Screening Ultrasonography as an Adjunct to Screening Mammography in Women Across the Spectrum of Breast Cancer Risk. JAMA Intern Med 2019;179(5):658-667.
2. Katscher U, Kim DH, Seo JK. Recent progress and future challenges in MR electric properties tomography. Comput Math Methods Med 2013;2013:546562.
3. Suh J, Kim JH, Kim SY, et al. Noncontrast-Enhanced MR-Based Conductivity Imaging for Breast Cancer Detection and Lesion Differentiation. J Magn Reson Imaging 2021;54(2):631-645.
4. Shin J, Kim MJ, Lee J, et al. Initial study on in vivo conductivity mapping of breast cancer using MRI. J Magn Reson Imaging 2015;42(2):371-378.
5. Mori N, Tsuchiya K, Sheth D, et al. Diagnostic value of electric properties tomography (EPT) for differentiating benign from malignant breast lesions: comparison with standard dynamic contrast-enhanced MRI. Eur Radiol 2019;29(4):1778-1786.
6. Baltzer P, Mann RM, Iima M, et al. Diffusion-weighted imaging of the breast-a consensus and mission statement from the EUSOBI International Breast Diffusion-Weighted Imaging working group. Eur Radiol 2020;30(3):1436-1450.
7. Comstock CE, Gatsonis C, Newstead GM, et al. Comparison of Abbreviated Breast MRI vs Digital Breast Tomosynthesis for Breast Cancer Detection Among Women With Dense Breasts Undergoing Screening. JAMA 2020;323(8):746-756.
Figures