0146
AMIDE PROTON TRANSFER IMAGING-ARTERIAL SPIN LABELING MISMATCH – A NEW IMAGING BIOMARKER FOR PILOCYTIC ASTROCYTOMA
Adhithyan Rajendran1, Chidambaranathan Natesan2, Lavanya Yegnaraman2, Rakesh Jalali3, Rashmi Rao4, Manikandan Mariyapillai5, Prashant Jawahar1, Roopesh Kumar6, Srinivas Chilukuri7, and Sushma Patil8
1Radiology, Apollo Proton Cancer Centre, Chennai, India, 2Radiology, Apollo Hospitals Greams Road, Chennai, India, 3Radiation Oncology, Apollo Proton Cancer Centre, chennai, India, 4Radiology, Philips India Ltd, Bangalore, India, 5Philips India Ltd, Chennai, India, 6Neurosurgery, Apollo Proton Cancer Centre, Chennai, India, 7Radiation Oncology, Apollo Proton Cancer Centre, Chennai, India, 8Pathology, Apollo Proton Cancer Centre, Chennai, India
1Radiology, Apollo Proton Cancer Centre, Chennai, India, 2Radiology, Apollo Hospitals Greams Road, Chennai, India, 3Radiation Oncology, Apollo Proton Cancer Centre, chennai, India, 4Radiology, Philips India Ltd, Bangalore, India, 5Philips India Ltd, Chennai, India, 6Neurosurgery, Apollo Proton Cancer Centre, Chennai, India, 7Radiation Oncology, Apollo Proton Cancer Centre, Chennai, India, 8Pathology, Apollo Proton Cancer Centre, Chennai, India
Synopsis
Keywords: Tumors, CEST & MT, Amide Proton Transfer Imaging
Atypical features of Pilocytic astrocytoma (PA) on conventional MR imaging are often challenging and can be mistaken as High-grade glioma. Advanced Novel techniques of Amide Proton Transfer (APT) and Arterial spin labelling (ASL) have shown promising results in the grading of gliomas. This study to explore the added value and utility in characterizing the atypical form of PA, if these two non-contrast techniques are combined in the clinical practice. Mismatch between APT and ASL signals, was seen in all the cases of PA and this unique imaging appearance of APT ASL imaging mismatch could be a biomarker for pilocytic astrocytoma.INTRODUCTION
Pilocytic astrocytoma, (PA) classified as grade I by the World Health Organisation, classically appears as a cystic mass with solid enhancing mural nodule on MR Imaging. In one third of cases, PA may overlap with those features of higher grade neoplasms having infiltration of surrounding tissues, intratumoral hemorrhage, intense enhancement on post contrast images, and leptomeningeal dissemination. So, PA can be often be mistaken as high-grade glioma, which has completely different therapeutic strategies and prognoses. Amide Proton Transfer weighted (APTw) MRI is a new, unique, contrast-agent free brain MR imaging technique based on presence of endogenous cellular proteins to produce an MR signal that directly correlates with cell proliferation, a marker of tumor activity1,2. Arterial spin labeling (ASL) as a non-contrast MRI perfusion technique has been used for evaluating the degree on the angiogenesis of the brain tumor and it helps in the grading of glioma3. No prior studies involving the Amide proton tensor imaging of pilocytic astrocytomas was available. Hence, this study to determine the utility of both the physiological and molecular based techniques in characterizing Pilocytic astrocytomaMATERIALS AND METHODS
Subjects: After institutional ethical committee approval, this study was performed. All patients gave written informed general consent. In this retrospective study, we included 75 patients in this study, with 25 patients diagnosed with histo-pathologically proven grade 1 pilocytic astrocytoma; 25 patients with histo-pathologically proven grade 2 and grade 3 glioma (astrocytoma, oligodendroglioma, Pleomorphic xanthoastrocytomas): 25 patients with non-Pilocytic astrocytoma posterior fossa tumors (ependymoma, medulloblastoma, diffuse midline glioma, astrocytoma, Embryonal tumor with Multilayered Rosettes, Atypical teratoid/rhabdoid tumors). Pilocytic astrocytomas were histopathologically diagnosed by conventional stains and with BFAF mutation. Consecutive patient studies acquired between Jan 2019 and Oct 2022 at a single tertiary institution were reviewed. Inclusion criteria: Purely solid or predominantly solid (> 75%) intra-cranial and intra-axial tumours were included, as any cystic lesions irrespective of the lesion types can have raised APT values. Patients who have undergone both Amide transfer imaging (APT) and arterial spin labeling imaging (ASL) were included. Cystic lesion with mural nodule, with classical imaging appearance of pilocytic astrocytoma were excluded.MRI imaging: Imaging was done in 3T MRI scanner (Ingenia Elition, Philips Healthcare, the Netherlands) with a 32 channel receive-only head coil array. Following sequences were acquired: 3D T1-weighted turbo field echo, 3D T2 FLAIR weighted turbo field echo, diffusion-weighted imaging, susceptibility weighted imaging, 3D pseudo continuous arterial spin labeling (ASL) perfusion imaging, Amide Proton transfer imaging (APTw) imaging, dynamic susceptibility perfusion imaging, Multivoxel MR spectroscopy, post-contrast 3D T1-weighted turbo field echo. We used a clinically approved APTw sequence acquired in transverse oblique orientation parallel to the intercommissural line. 12 slices protocol avoiding paranasal sinues (to avoid artifacts) were acquired.
Image analysis: APTw and other imaging sequences in Digital Imaging and Communications in Medicine (DICOM) files were loaded into the work station and were aligned symmetrically. Subsequently, two readers (with 9 years and 35 years of experience) manually segmented the neoplasms. Imaging features of the tumours in all the sequences were analysed.
RESULTS
In Amide proton tensor imaging, all the 25 subjects with PA tumor cases showed diffuse homogenously increased MTRasym values reaching >=4. All the PA lesions showed low CBF in ASL. Mismatch was seen between the APT MTRasym and ASL CBF was seen in all the cases (Figures 1 to 5) of Pilocytic astrocytoma. In none of the remaining 50 patients (posterior fossa tumors and grade 2 or 3 glioma), there was mismatch between the APT MTRasym and ASL CBF..
DISCUSSION
APTw is used for grading of the gliomas. No prior studies involving the Amide proton transfer imaging of pilocytic astrocytomas was available. Many times, the solid appearing pilocytic astrocytomas mimics astrocytoma, diffuse midline glioma, ependymoma, medulloblastoma depending upon the locations. Imaging appearance of cyst with mural nodule of pilocytic astrocytoma is classical imaging feature, however, in many of the cases the classic imaging appearance is lacking, with presence of solid appearing mass lesions.In our study, solid or predominantly solid pilocytic astrocytomas were found to have particular imaging appearance in Amide Proton Transfer imaging and ASL imaging. All the Pilocytic astrocytoma tumours showed homogeneous significantly high APT values and low signal in ASL. This unique imaging appearance of mismatch between amide proton transfer and ASL perfusion imaging could be a biomarker for Pilocytic tumor. The high proton transfer values in pilocytic astrocytoma in this study may be due to high intracellular and extracellular matrix protein content. Low CBF in ASL in the pilocytic astrocytoma may be due its low grade nature. The differentiation of pilocytic astrocytoma from other high-grade tumor like diffuse midline glioma, ependymoma is very important because the prognosis space is significantly different between the pilocytic astrocytoma and other tumours. In many instances, direct radiotherapy is given to brainstem glioma without histopathological confirmation of the tumor. In those cases, the mismatch sign is very helpful to diagnose the low-grade pilocytic astrocytoma. More over these two techniques (both APTw and ASL) are non-contrast sequences, having distinct advantages in children.
CONCLUSION
Unique imaging appearance of mismatch between Amide proton transfer and ASL perfusion imaging could be a potential biomarker for Pilocytic tumor.Acknowledgements
No acknowledgement found.References
1) Togao O, Keupp J, Hiwatashi A, et al. Amide proton transfer imaging of brain tumors using a self-corrected 3D fast spin-echo Dixon method: comparison with separate B0 correction. Magn Reson Med 2017; 77: 2272–2279.2) Togao O, Hiwatashi A, Keupp J, et al. Amide proton transfer imaging of diffuse gliomas: effect of saturation pulse length in parallel transmission-based technique. PLoS One 2016; 11: e0155925.
3)Troudi, A.; Tensaouti,F et al Arterial Spin Labeling Perfusion in Pediatric Brain Tumors: A Review of Techniques, Quality Control, and Quantification. Cancers 2022, 14, 4734.
Figures
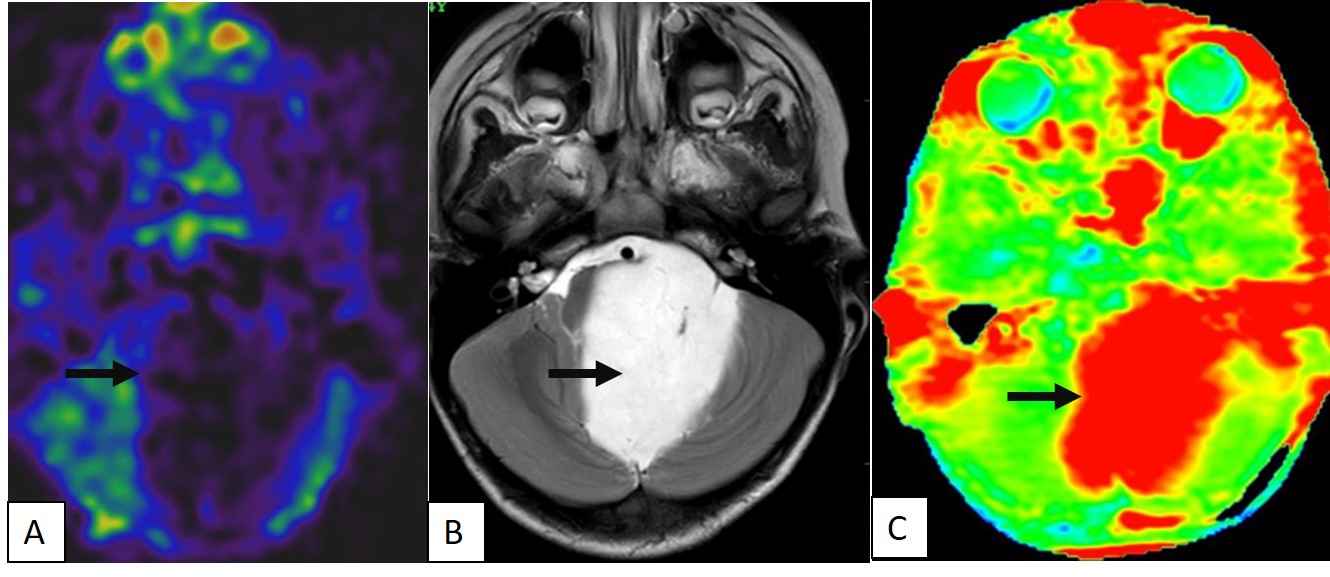
A well-defined T2 hyperintense (B) large solid non cystic mass lesion seen involving the left side pons, left cerebellar hemisphere. Lesion showed diffuse hypoperfusion in ASL (A) and diffuse high values in Amide Proton Transfer Imaging(C). This is a histologically proven Grade 1 Pilocytic Astrocytoma.
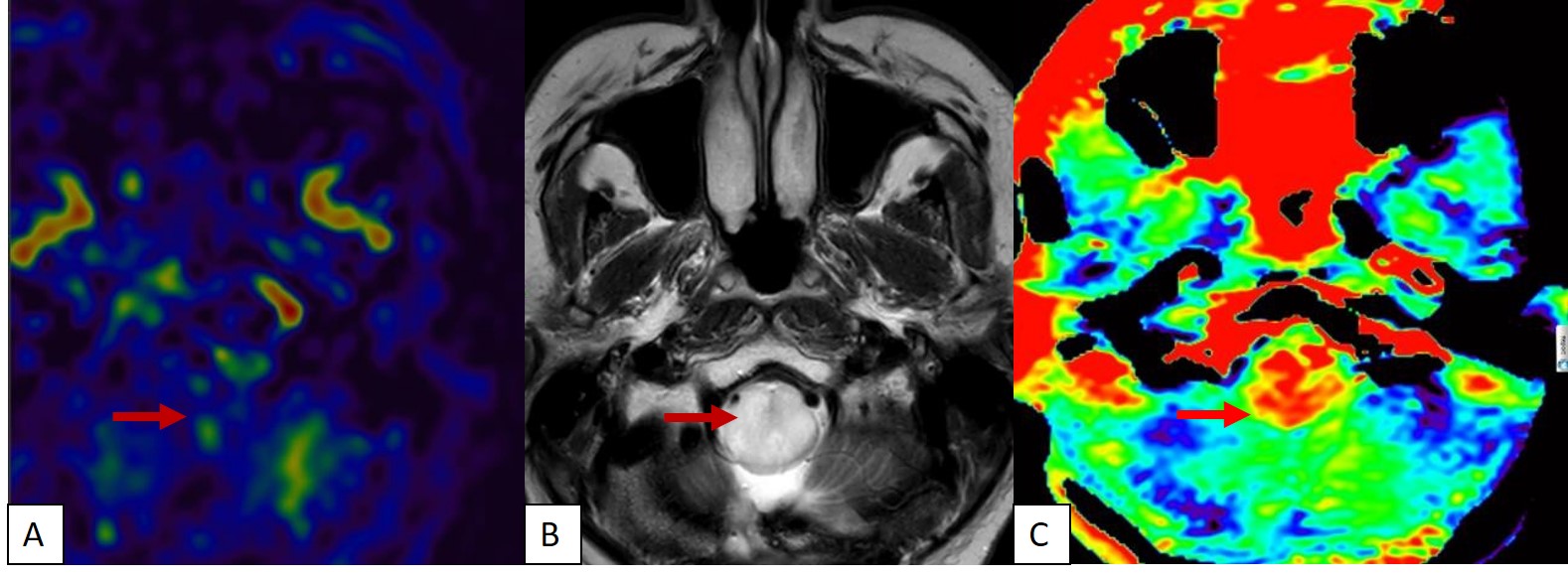
A T2 hyperintense (B) solid expansile mass lesion seen involving the medulla. Lesion showed diffuse hypoperfusion in ASL (A) and diffuse high values (C) in Amide Proton Transfer Imaging. This is a histologically proven Grade 1 Pilocytic Astrocytoma.
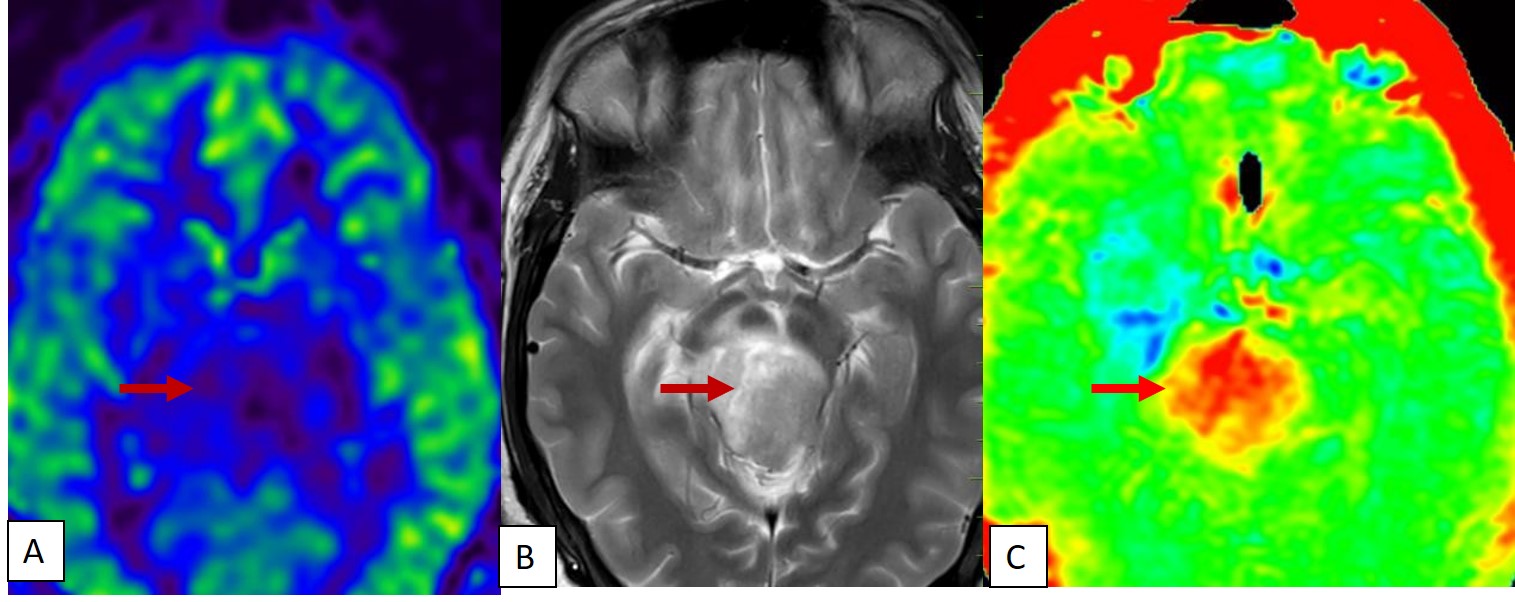
A T2 hyperintense solid expansile mass lesion (B) seen involving the midbrain. Lesion showed diffuse hypoperfusion in ASL (A) and diffuse high values (C) in Amide Proton Transfer Imaging. This is a histologically proven Grade 1 Pilocytic Astrocytoma.
A T2 hyperintense (B) predominantly solid mass lesion seen involving the cerebellum, left middle cerebellar peduncle Lesion showed diffuse hypoperfusion in ASL (A) and diffuse high values in Amide Proton Transfer Imaging (C). This is a histologically proven Grade 1 Pilocytic Astrocytoma.
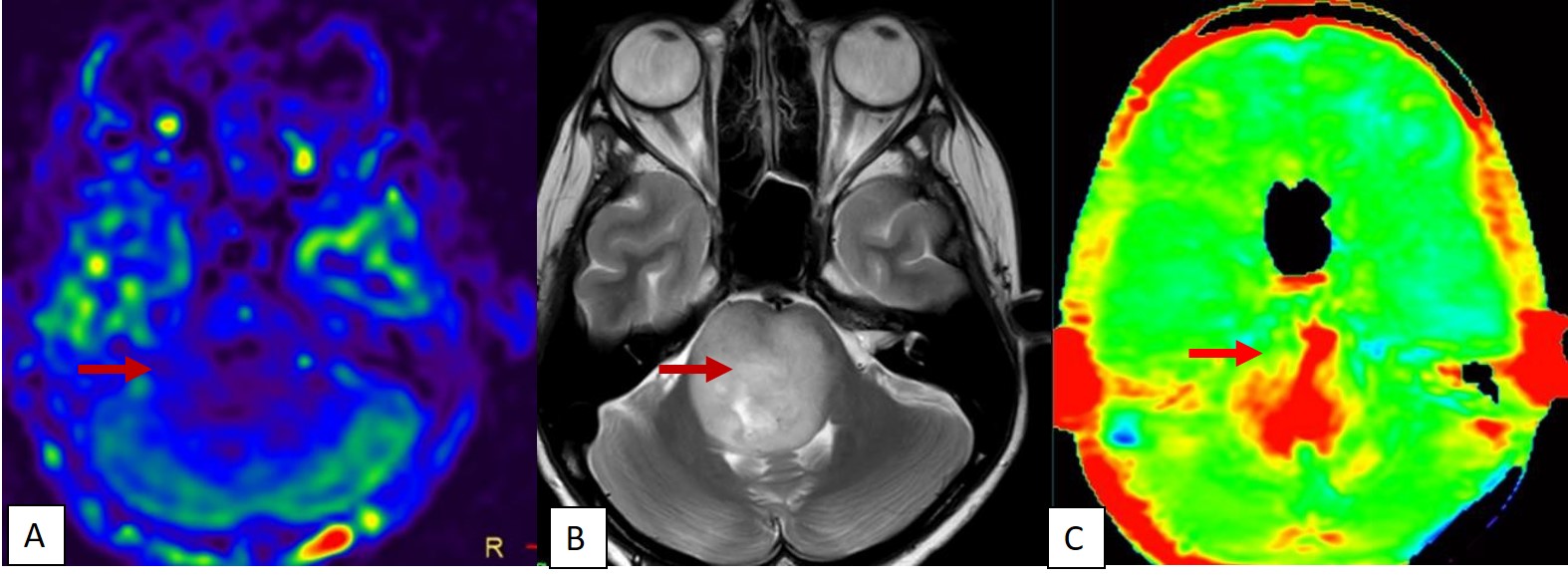
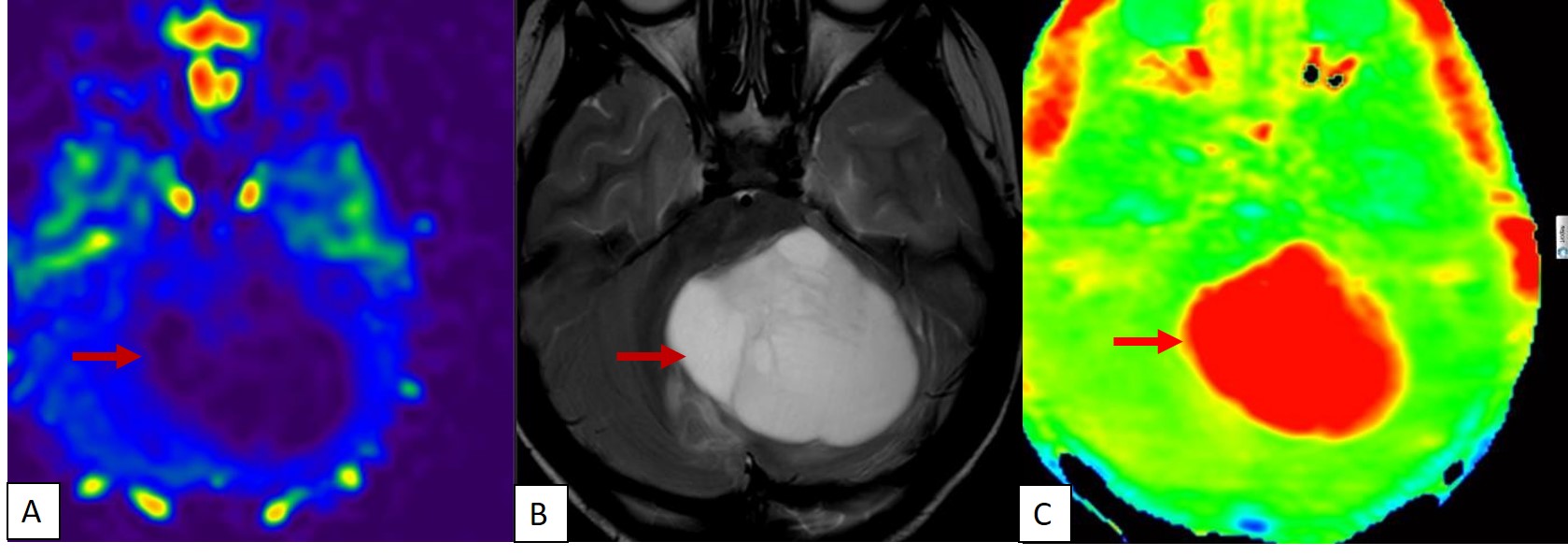
A T2 hyperintense (B) solid expansile mass lesion seen involving the Pons. Lesion showed diffuse hypoperfusion in ASL (A) and diffuse high values in Amide Proton Transfer Imaging. (C) This is a histologically proven Grade 1 Pilocytic Astrocytoma.
DOI: https://doi.org/10.58530/2023/0146