0111
Simultaneous Brain and Neck Time of Flight using Spiral Multiband with Localized Quadratic Encoding1Mayo Clinic, Rochester, MN, United States, 2Philips Healthcare, Rochester, MN, United States
Synopsis
Keywords: New Trajectories & Spatial Encoding Methods, Blood vessels
A spiral multiband localized quadratic encoding (LQE) method is proposed to achieve simultaneous brain and neck time of flight MRA within a single 2.5-minute scan. LQE acquisition is efficient for both SNR and in-flow enhancement. Multi-band LQE enables increased coverage with no increase in scan time, but can introduce venous signal contamination. We propose a multi-band LQE approach with TONE and partial-Fourier slice selection to reduce the venous signal and achieve simultaneous time-of-flight MRA of intracranial and carotid arteries.Introduction
Time-of-flight MR angiography of intracranial and carotid arteries are often performed separately due to scan time and resolution constraints. In this work, we developed a novel spiral acquisition scheme to achieve simultaneous brain and neck time of flight MRA within a 2.5-minute scan using the combination of simultaneous multi-slice and localized quadratic encoding (LQE). Spiral LQE has been demonstrated to produce intracranial time of flight MRA with improved SNR and in-flow enhancement1. The simultaneous multi-slice/slab technique2 can be added to this approach to enable greater coverage without compromising scan time. However, to preserve the in-flow signal in the brain (top slabs), venous saturation bands cannot be positioned in between the simultaneously excited slabs, thus resulting in venous signal contamination in the neck. We propose to exploit TONE3 and partial-Fourier slice selection4 to mitigate the corruption from venous signal. In vivo human experiments have been conducted to demonstrate the feasibility of the proposed method for fast MRA of brain and neck arteries.Methods
Localized quadratic encoding5,6 is a technique that linearly sweeps the excitation RF frequency across a corresponding slab of thickness of $$$Mδ$$$, where $$$δ$$$ is the width of RF excitation without the frequency sweep, as well as (typically) the center-to-center spacing of these excited slabs. The overlapping slabs can then be deconvolved to have a resolution (thickness) of $$$δ$$$ by removing a quadratic phase (imposed by the frequency sweep) along the slice direction in k-space:$$H(k)=Ce^{i\pi M(\frac{k}{\gamma G\tau})^2}, \left| k \right|<0.5K_m,$$
where $$$M$$$ is the time-bandwidth product of the RF pulse, $$$K_m$$$ denotes k-space coverage, $$$G$$$ is the slice selection gradient and $$$\tau$$$ the pulse duration.
1) Data acquisition. With the integration of simultaneous multi-slice technique, a multiband LQE pulse was designed to linearly sweep over multiple slabs at different locations simultaneously. Phase differences in the signal from different slabs were imposed by the excitation rf pulse to provide additional incoherence that allowed the separation of these slices with minimal SNR penalty. TONE was implemented with linearly descending flip angles from the top to the bottom of each slab. Partial-Fourier slice selection was also implemented to move the k-space center downwards the bottom of each slab7. Acquisitions were carried out sequentially in the head to foot direction.
2) Image reconstruction. Multiband reconstruction was first performed to reconstruct the spiral images from the multichannel k-space data. Afterwards, the quadratic phase term along slice direction was removed from the reconstructed volumes. Finally, a deblurring procedure8 was conducted to correct the off-resonance effect and POCS-based partial Fourier was carried out to recover full resolution along slice before maximum intensity projection (MIP) was applied to visualize the in-flow artery signals.
Results and Discussion
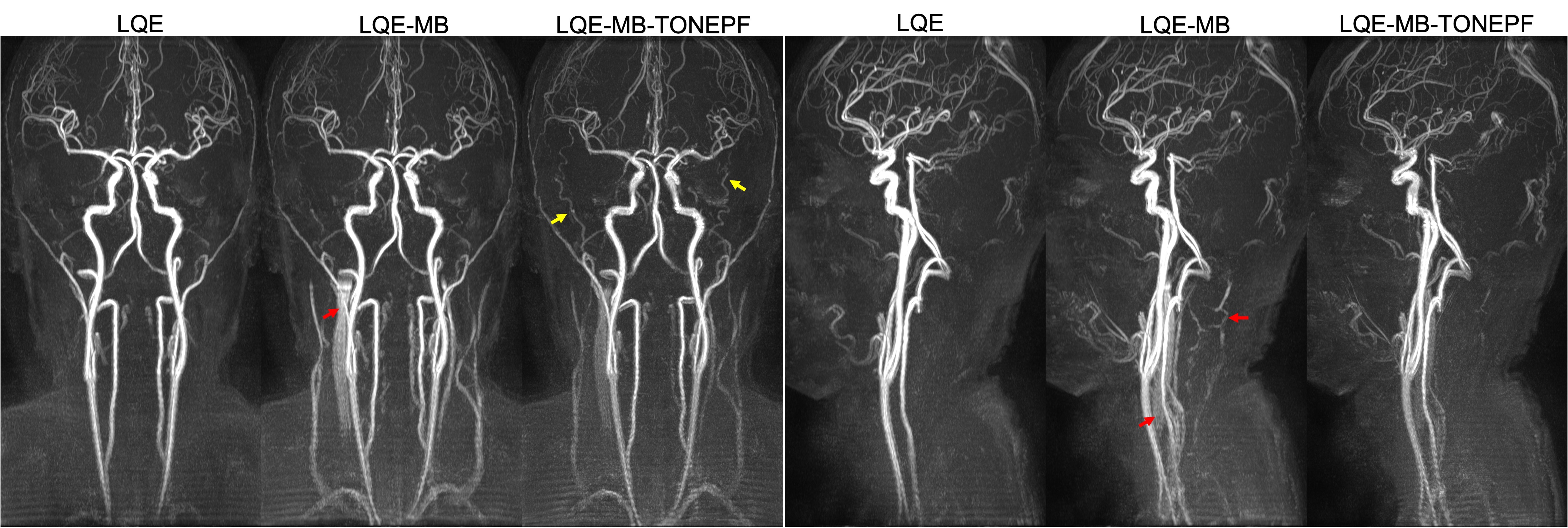
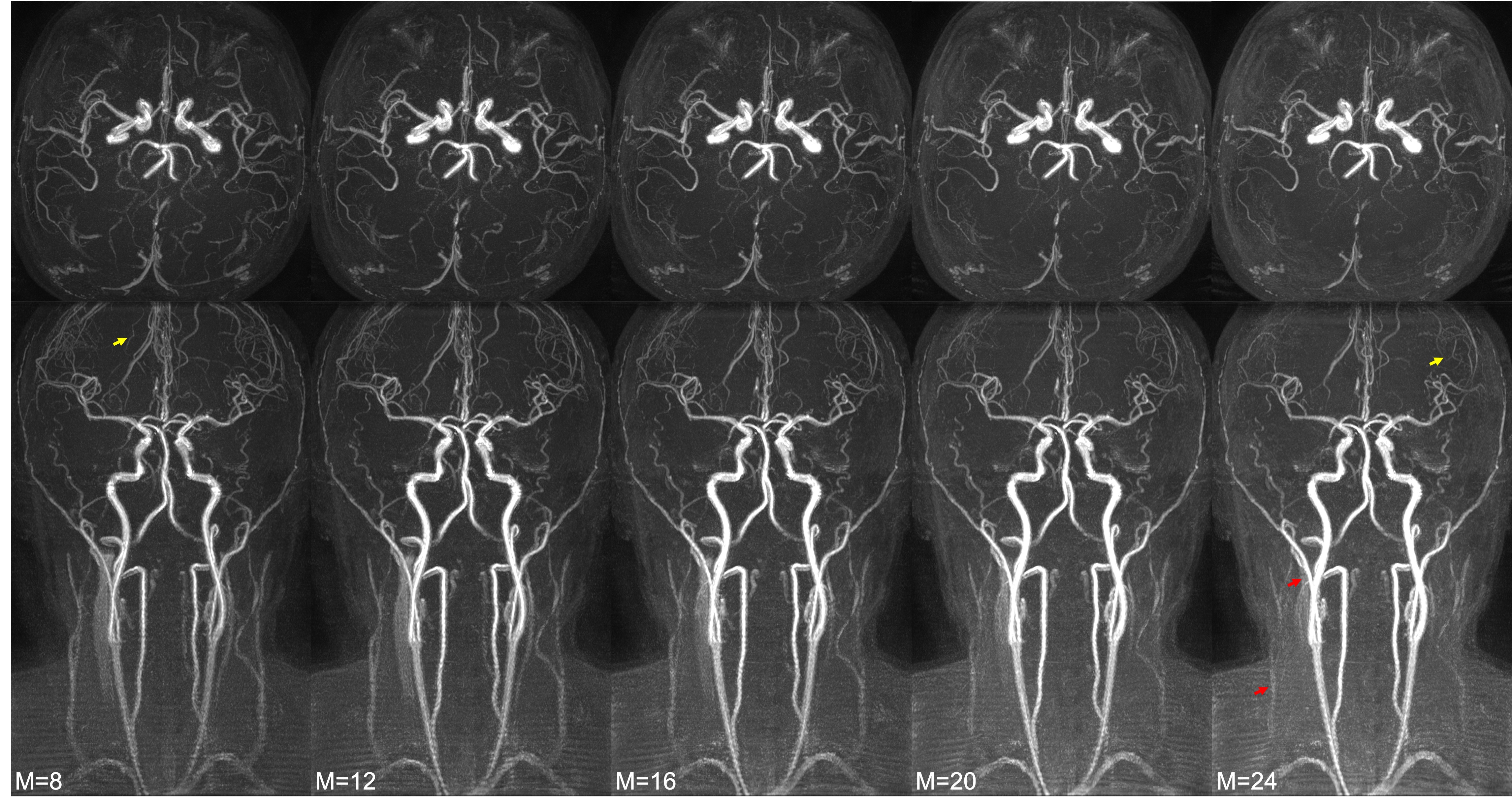
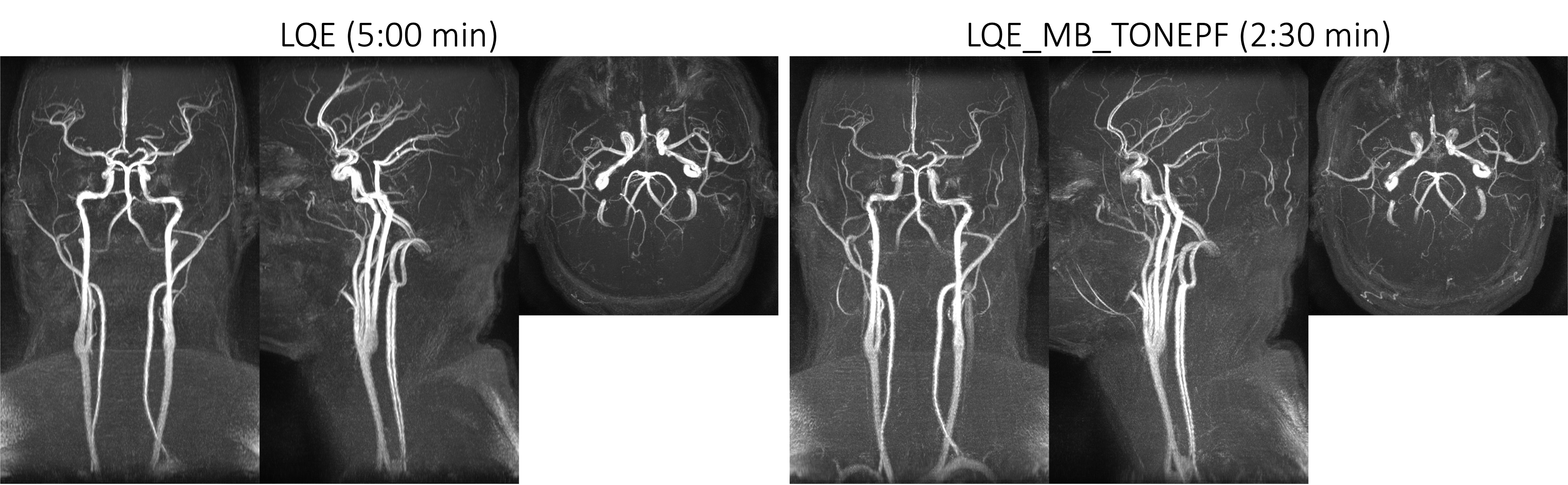
In vivo experiments were performed on two healthy subjects on a 3T MR scanner using a 16-channel head and neck coil with the approval of institutional review board. Scan parameters are as follows: FOV 200×200×270 mm3, resolution 0.7×0.7×1.4 mm3, TR 23ms, TE 3.45 ms, FA 30°, MB factor 2, spiral readout time 6 ms, TONE 45° to 15°, partial-Fourier slice selection 75% (i.e., k-space center moved downward 25% resulting in total 75% k-space coverage). Field inhomogeneity and coil sensitivity maps were obtained from separate low-resolution Cartesian scans. A moving venous saturation band was applied above the top image slab. Flow compensation was used to mitigate blood signal loss due to phase cancelation. Different values of $$$M$$$ values were implemented for comparison.Figure 1 shows the MIP results from different LQE sequences. Specifically, multi-band LQE reduced the scan time by half, but introduced venous signal contamination. The proposed method managed to substantially reduce the venous signal by using TONE and partial-Fourier slice selection with the same scan time, while yielding higher resolution along slice direction. The effect of M in the proposed method is illustrated in Fig. 2. As can be seen, larger M leads to both increased in-flow and background signal as well as improved venous signal suppression, but at the cost of reduced signal for small (slow flowing) vessels in the brain. Results from the other subject are displayed in Fig. 3., demonstrating the feasibility of our method for fast simultaneous head and neck MRA.
Conclusion
A novel LQE-based data acquisition and processing scheme was developed to achieve simultaneous brain and neck MRA within a single 2.5 minute scan. Future work includes further optimizing the scan parameters for the brain and neck respectively to achieve an improved balance between in-flow SNR and venous signal contamination.Acknowledgements
This work was supported in part by Royal Philips.References
1. Wang D, et al. Spiral Time of Flight with Sliding Slice Localized Quadratic Encoding. ISMRM 2019. p0759.
2. Schulz J, et al. Multiband Multislab 3D Time-of-Flight MagneticResonance Angiography for Reduced AcquisitionTime and Improved Sensitivity. Magn Reson Med. 2016;75:1662–1668.
3. Atkinson D, et al. ImprovedMR angiography: magnetization transfer suppression withvariable flip angle excitation and increased resolution. Radiology 1994;190:890-894.
4. Pipe JG. Flow effects in localized quadratic, partial Fourier MRA. Magn Reson Med. 1999;41:309- 314.
5. Pipe JG. Spatial Encoding and reconstruction in MRI with quadratic phase profiles. Magn Reson Med. 1995;33:24- 33.
6. Pipe JG. Analysis of localized quadratic encoding and reconstruction. Magn Reson Med. 1996;36:137- 146.
7. Pipe JG. Asymmetric Sampling Along kslice-seleinct in Two-Dimensional Multislice MRI. Magn Reson Med. 1998;39:625-634.
8. Wang D, et al. Joint water-fat separation and deblurring for spiral imaging. Magn Reson Med. 2018;79:3218- 3228.
Figures