0108
Efficient iT2prep-BOOST for simultaneous contrast-free 3D aortic lumen and vessel wall imaging for the assessment of thoracic aortopathy1King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Camberley, United Kingdom, 3MR Research Collaborations, Siemens Healthcare Limited, Camberely, United Kingdom, 4Biomedical Engineering, King's College London, London, United Kingdom, 5Institute for Biological and Medical Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile, 6Millennium Institute for Intelligent Healthcare Engineering, Santiago, Chile, 7School of Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile
Synopsis
Keywords: Data Acquisition, Cardiovascular, aorta
Bright- and black-blood MRI sequences are clinically acquired sequentially, for aortic lumen and vessel wall imaging respectively, in patients with thoracic aortic disease. A novel, free-breathing, 3D sequence (iT2prep-BOOST) is proposed for contrast-free simultaneous depiction of lumen and vessel wall. We clinically validated the iT2prep-BOOST in a cohort of 25 patients with thoracic aortic disease against the conventional bright-blood T2-prep bSSFP sequence and black-blood 2D HASTE. Quantitative and qualitative image quality assessment demonstrated that iT2Prep-BOOST enabled time-efficient, bright- and black-blood aortic imaging, with improved image quality compared to conventional approaches, and comparable measurements for aortic wall and lumen dimensions.Introduction
Recently published clinical guidelines proposed the acquisition of both bright-blood and black-blood MRI for the comprehensive assessment of thoracic aortic disease1,2. 2D breath-held turbo-spin echo sequences (TSE) enable vessel wall imaging and the 3D diaphragmatic navigator-gated T2-prepared balanced Steady State Free Precession (T2-prep bSSFP) bright-blood sequences allow luminal assessment. Limitations of the current approaches include prolonged scan times, due to the diaphragmatic navigation and the sequential acquisition of the two contrasts, along with potential patient discomfort due to breath-holds. Additionally, image misregistration between contrasts might impede robust clinical interpretation. To overcome those limitations, we sought to investigate the feasibility and evaluate the performance of a novel accelerated and respiratory motion-compensated 3D cardiac MRI technique for simultaneous contrast-free bright- and black-blood aortic imaging (iT2Prep-BOOST)3.Methods
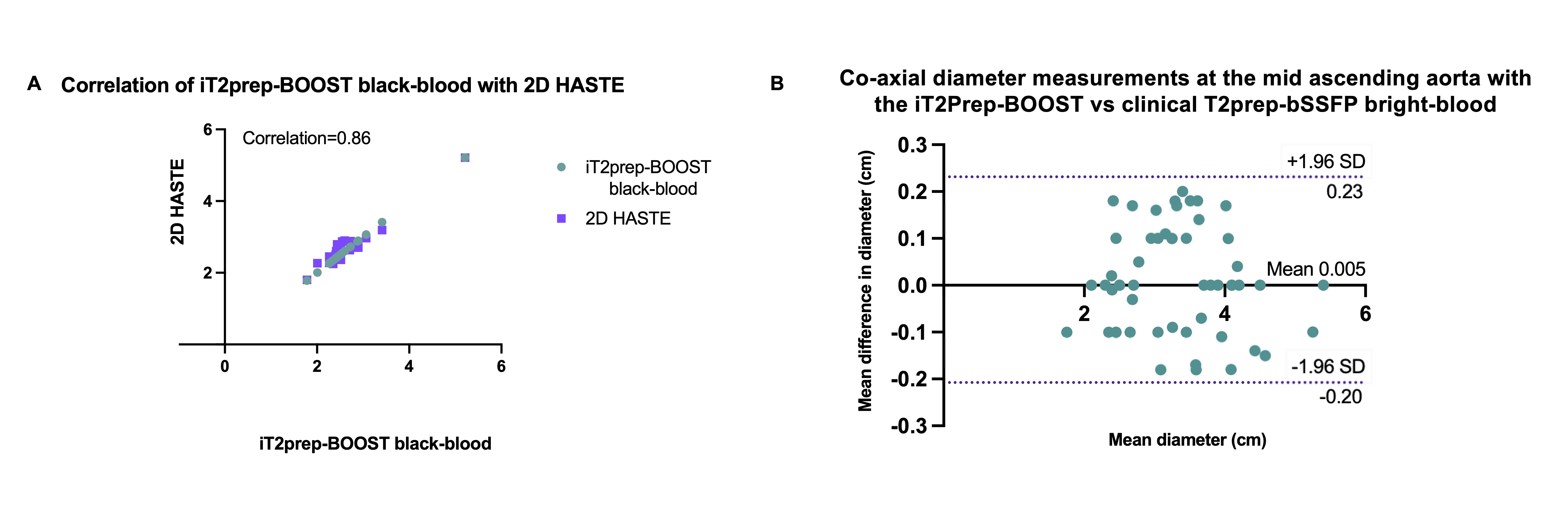
Twenty-five patients with aortopathy (14 male, 31±10 years old) were scanned at a 1.5T system (MAGNETOM Aera, Siemens Healthcare, Germany). The proposed 3D free-breathing, ECG-triggered bSSFP iT2prep-BOOST sequence (Fig.1) utilises an interleaved acquisition framework, where a T2 prepared- Inversion Recovery (T2Prep-IR) module is applied before data acquisition in odd heartbeats and no preparation is applied in even heartbeats3. Subsequently 3D HD-PROST denoising was performed off-line4. The first bright-blood dataset can be used for lumen visualization, while subtraction of the two bright-blood datasets is used to create the black-blood dataset for vessel wall visualization. Main acquisition parameters included: coronal orientation, 1.3mm3 isotropic resolution, FOV=300x400x104-156mm3, T2prep=40ms, TI=110ms, TE/TR=1.41/3.24ms. Acquisition time and image quality of the research sequence was compared against the clinical sequences, which included the T2prep-bSSFP sequence [sagittal orientation, 1.4mm3 isotropic resolution, FOV=240×400×134-168mm3, T2prep=40ms] and 2D breath-held Half-Fourier Acquisition Single-shot Turbo spin Echo (HASTE) [axial orientation, 1.6mm in-plane resolution, 8mm slice thickness]. Two blinded experts recorded their diagnostic confidence using 4-point Likert scale (3≥ diagnostic). Co-axial vascular dimensions at the level of the mid ascending aorta were obtained with both methods and compared between the readers using Bland-Altman analysis. One additional patient was scanned with the proposed approach and with CT to investigate the feasibility in chronic dissection patients.Results
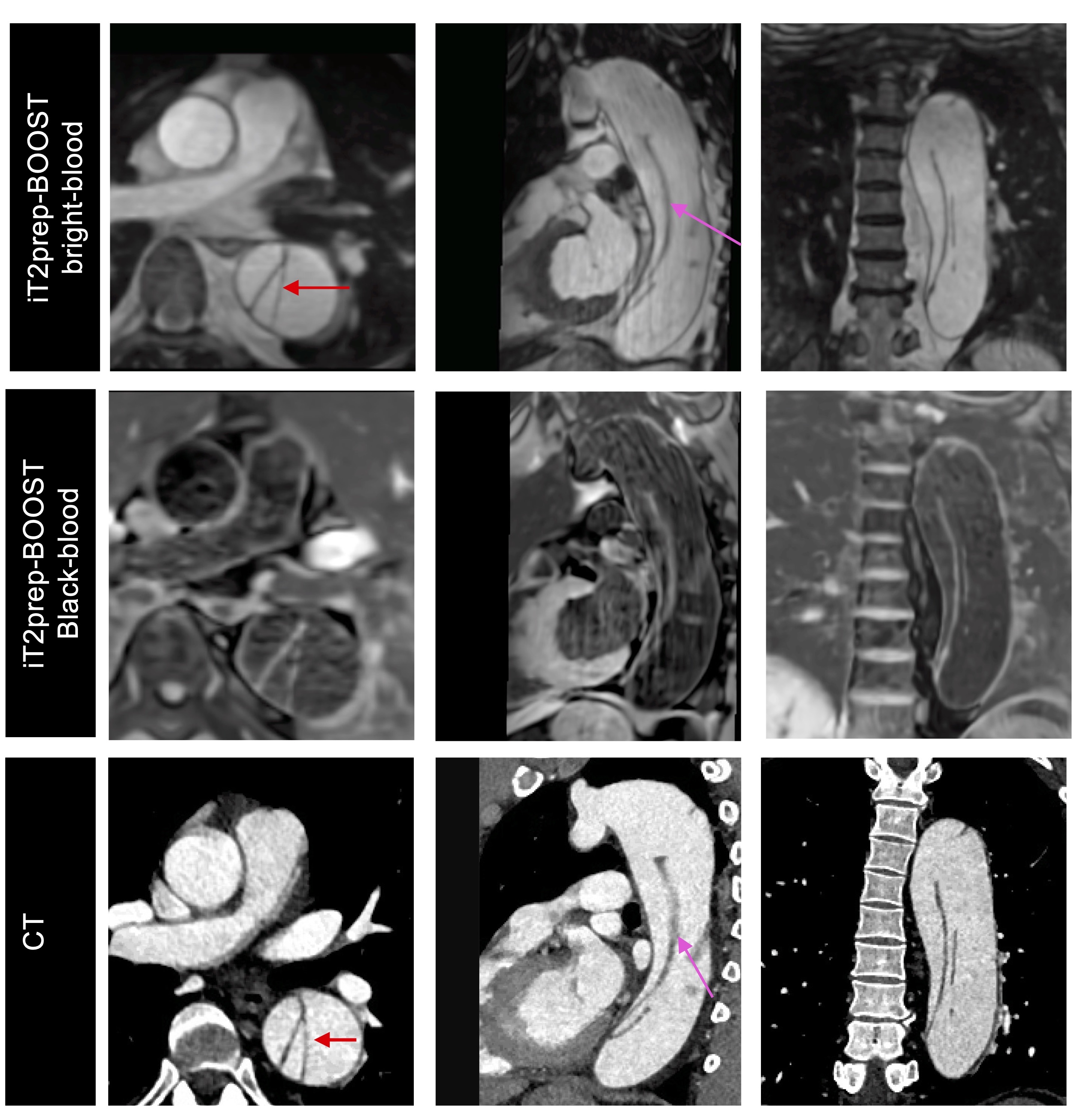
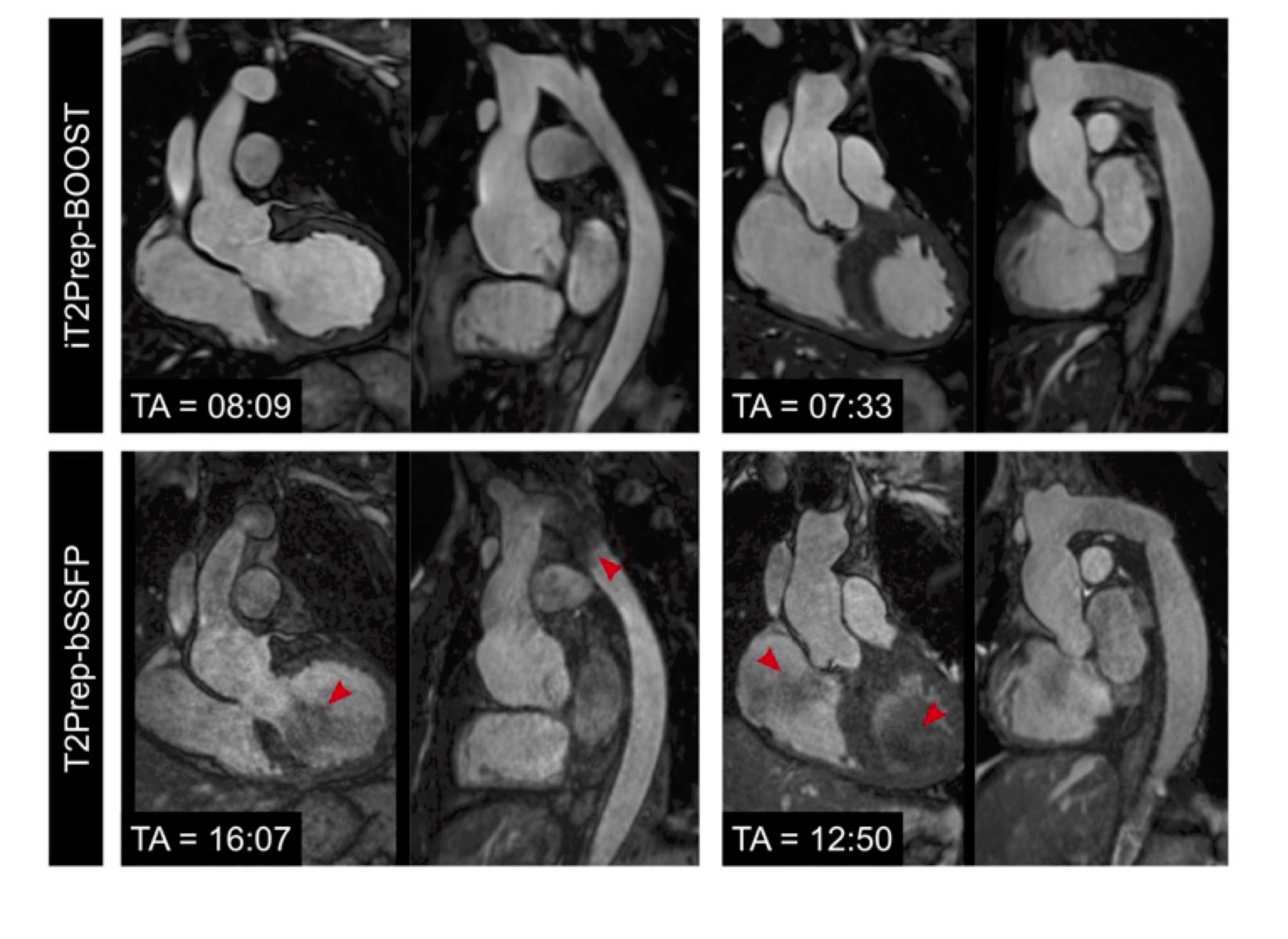
The average scan time for the proposed 3D iT2Prep-BOOST method was 8.0±1.5min versus 13.2±3.2 min for the conventional sequences (including both T2prep bSSFP and HASTE), (P<0.001). Diagnostic confidence was higher for the proposed approach compared to the clinical sequence for both reviewers (Reviewer 1: 4(3.5, 4) vs 3(2.5, 3), P=0.007; Reviewer 2: 4(4, 4) vs 4 (3, 4), P=0.009). Good image quality of the aortic luminal signal can be observed with the proposed bright-blood technique, which is comparable or superior to the conventional T2prep bSSFP (Fig.2). Additionally, the proposed sequence generates black-blood vessel wall image with improved coverage compared to the conventional 2D HASTE (Fig.3). The iT2Prep-BOOST black-blood images can be reformatted into any plane of interest, achieving uniform blood suppression. Imaging of the aortic dissection with the proposed iT2prep-BOOST demonstrated comparable results to CT, which is the clinical gold standard in our institution (Fig. 4). Aortic lumen diameter and vessel wall thickness measurements in bright and black-blood images were in good agreement with conventional imaging (Fig. 5).Discussion
We have here introduced an accelerated iT2Prep-BOOST sequence that provides excellent depiction of the aortic lumen and wall, with a predictable scan time of ~8min. This approach holds promise for forthcoming clinical adoption for the comprehensive assessment of thoracic aortic disease.Acknowledgements
This work was supported by the following grants: (1) EPSRC P/V044087/1; (2) BHF programme grant RG/20/1/34802, (3) Wellcome/EPSRC Centre for Medical Engineering (WT 203148/Z/16/Z), (4) Millennium Institute for Intelligent Healthcare Engineering ICN2021_004, (5) FONDECYT 1210637 and 1210638, (6) IMPACT, Center of Interventional Medicine for Precision and Advanced Cellular Therapy, ANID FB210024.References
1. Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine [published correction appears in Circulation. 2010 Jul 27;122(4):e410]. Circulation. 2010;121(13):e266-e369. doi:10.1161/CIR.0b013e3181d4739e.
2. Kramer CM, Barkhausen J, Bucciarelli-Ducci C, Flamm SD, Kim RJ, Nagel E. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J Cardiovasc Magn Reson. 2020;22(1):17. Published 2020 Feb 24. doi:10.1186/s12968-020-00607-1.
3. Milotta G, Ginami G, Cruz G, Neji R, Prieto C, Botnar RM. Simultaneous 3D whole-heart bright-blood and black blood imaging for cardiovascular anatomy and wall assessment with interleaved T2 prep-IR. Magn Reson Med. 2019;82(1):312-325. doi:10.1002/mrm.27734
4. Bustin A, Lima da Cruz G, Jaubert O, Lopez K, Botnar RM, Prieto C. High-dimensionality undersampled patch-based reconstruction (HD-PROST) for accelerated multi-contrast MRI. Magn Reson Med. 2019;81(6):3705-3719. doi:10.1002/mrm.27694
Figures
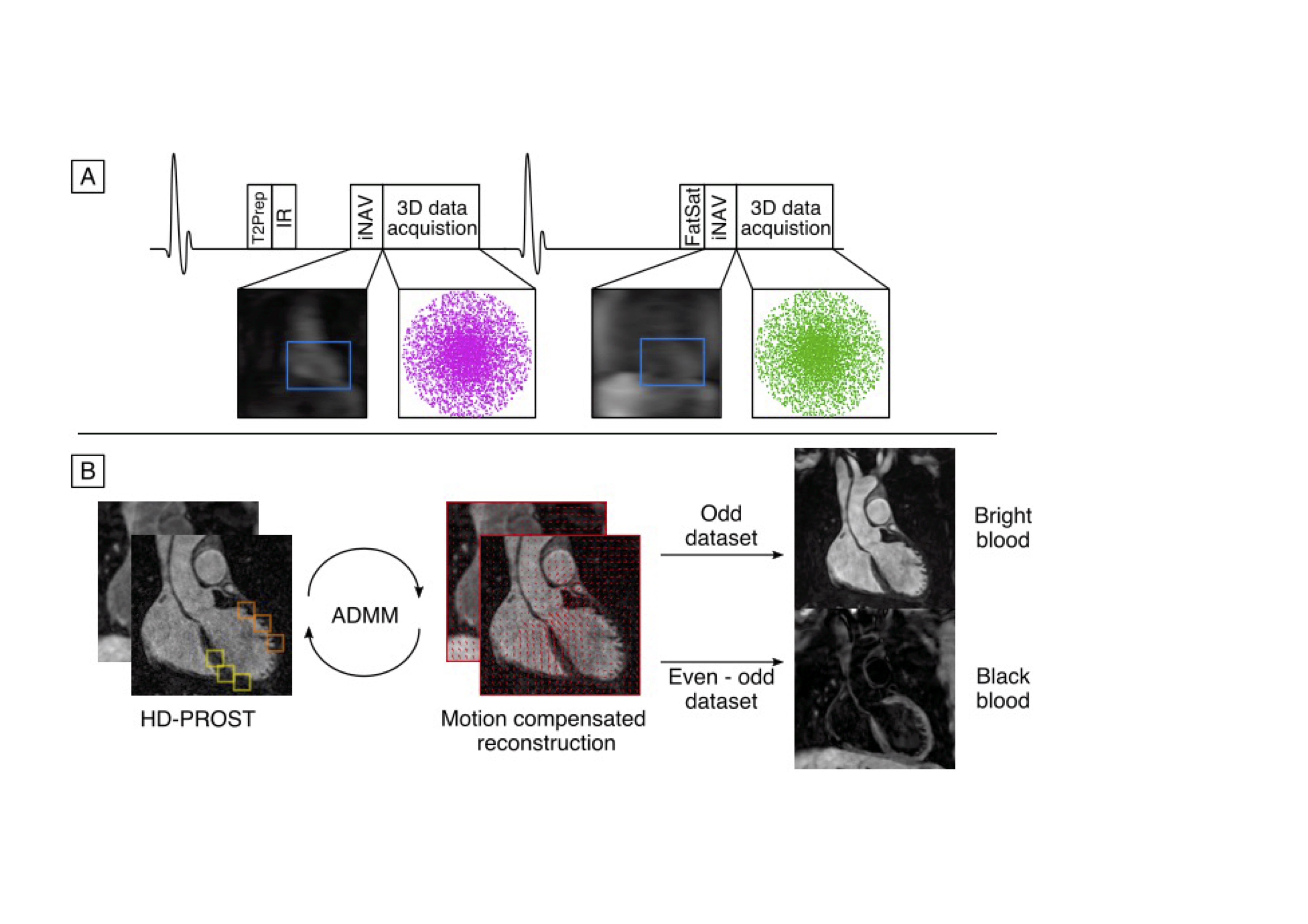
A.Data are acquired with a 4-fold undersampled variable-density Cartesian trajectory with an interleaved framework, where a T2Prep-IR precedes the data acquisition in odd heartbeats and no preparation is applied in even heartbeats. Beat-to-beat 2D translational and bin-to-bin 3D non-rigid respiratory motion are estimated from the iNAVs. B. Low-rank patch-based denoising (HD-PROST) is performed off-line. Bright-blood data (odd heartbeats) are utilised for lumen and black-blood data (generated by direct subtraction of even and odd heartbeats) for vessel wall visualization.
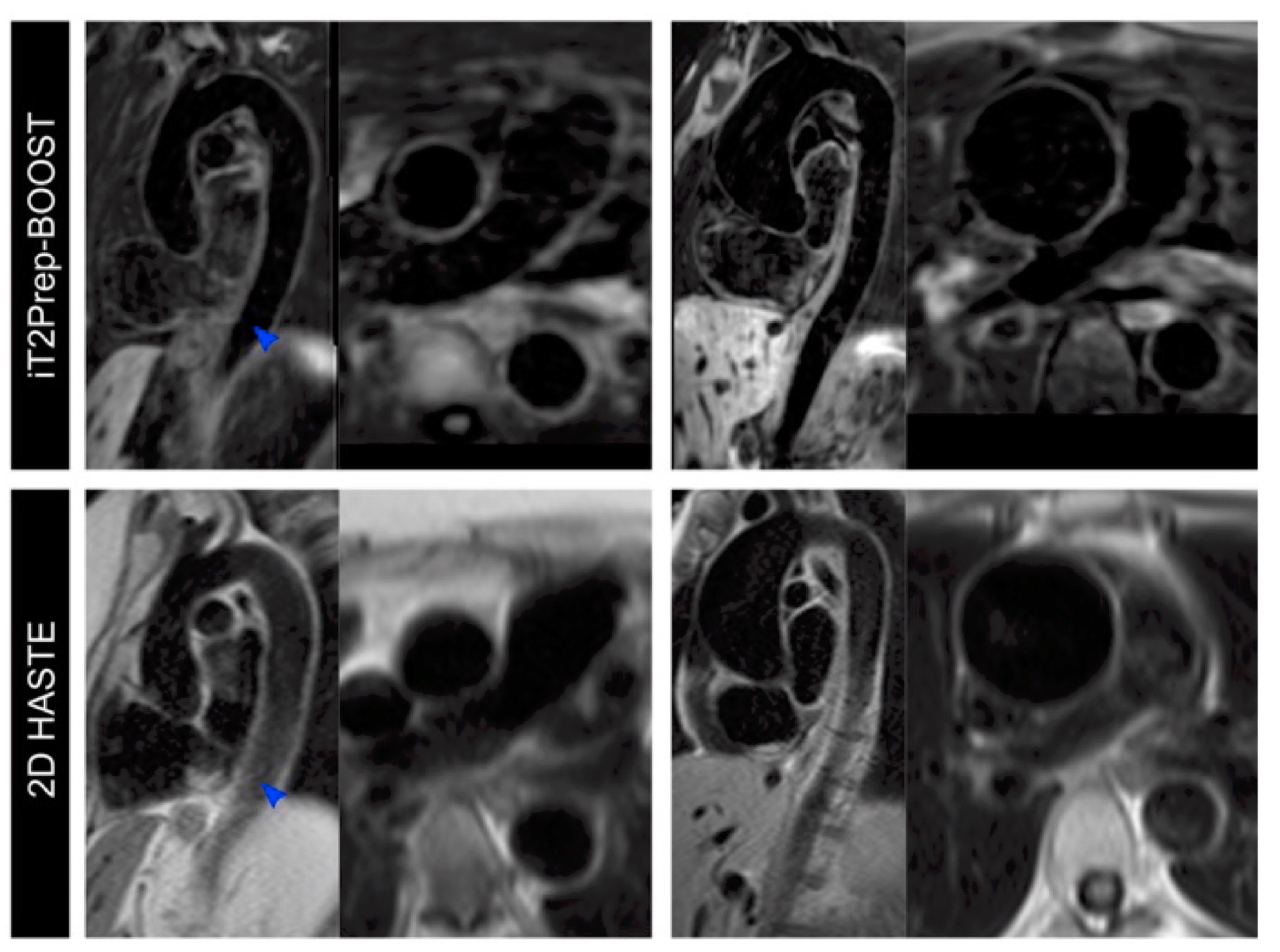
Black-blood images acquired with the proposed iT2Prep-BOOST (top row) compared to the conventional 2D HASTE (bottom row) for two patients.The iT2prep-BOOST images demonstrate sharp demarcation of the vessel wall and uniform blood suppression.
A. 62-year-old patient with Marfan’s syndrome.
B. Aortic aneurysm in a 37-year-old patient with bicuspid aortic valve. Image quality is degraded by insufficient blood suppression in the sagittal oblique views of the 2D HASTE, due to the complex flow patterns in the tortuous descending aorta (blue arrows).