0072
Intravoxel incoherent motion DWI with different mathematical models in predicting rectal adenoma with and without canceration1Lixia District, Jinan city, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan, Jinan, China, 2MR Research, GE Healthcare, Beijing, China
Synopsis
Keywords: Data Analysis, Cancer
This study aimed to use intravoxel incoherent motion (IVIM) DWI with different mathematical models to predict rectal adenomas with and without canceration. The parameters of different IVIM-DWI models, including apparent diffusion coefficient (ADC) from mono-exponential model, true diffusion coefficient, pseudo-diffusion coefficient and perfusion fraction from bi-exponential model, and the distributed diffusion coefficient and water molecular diffusion heterogeneity index from stretched-exponential model were compared between 31 adenoma and 29 adenoma with canceration. We found that mono-exponential derived ADC can easily predict rectal adenomas with canceration, and bi-exponential model has a better combination of sensitivity and specificity for diagnosing rectal adenoma canceration.Introduction
Colorectal cancer (CRC) is the third most common cancer worldwide1. Early detection of colorectal adenoma, a precancerous lesion of CRC, can reduce CRC incidence 2. Colonoscopy is a widely applied method for detecting rectal adenomas in clinic3. But colonoscopy cannot evaluate heterogeneity inside tumor or the invasion depth of rectal wall4. Intravoxel incoherent motion (IVIM) DWI uses multi-b values to reflect tissue dispersion and micro-perfusion5 with different mathematic models. Varied patterns of IVIM parameters, derived such as from mono-exponential model (ME), bi-exponential model (BE) and stretched-exponential model (SE), have been reported to relate with the enlargement of cell nucleus, tight arrangement of cells and proliferation of new blood vessels in cancer tissues, affecting the dispersion and pre-fusion of water molecules6,7. Moreover, IVIM has been used to identify rectal cancer patients with micro-nodal involvement before surgery. With these promising evidences, it remains however unknown if the IVIM-DWI is also feasible to predict rectal adenomas with canceration. Therefore, the main goal of study was to investigate if IVIM-DWI with different mathematical models was feasible to preoperatively predict rectal adenoma with canceration.Materials and Methods
Subjects31 adenoma patients (15 male and 16 female, mean age 61.87±10.60) and 29 adenoma with canceration patients (17 male and 12 female, mean age 62.59±13.32) were included in this study. The lesions of all patients were confirmed by postoperative pathology. Each participant underwent IVIM-DWI scanning before surgery.
MRI experiments
All patients underwent MRI measurements on a 3.0 T system (Discovery 750w; GE Healthcare) using an eight-channel phased-array body coil in the supine position. Fast spin echo (FSE) T2WIs were separately performed in the sagittal,coronal and oblique views. Axial spin-echo echo-planar-image based IVIM-DWI scanning was performed with 11 b-values applied, namely 0, 20, 50, 100, 150, 200, 400, 600, 800, 1000, and 1500 s/mm2. The number of excitation (NEX) was 2 for b values of 20, 50, 100, and 150 s/mm2 , 4 for b values of 0, 200, 400, 600, 1000 and 1500 s/mm2; and 6 for b value of 800 s/mm2 . The total scan time was 21 mins.
Image Analysis
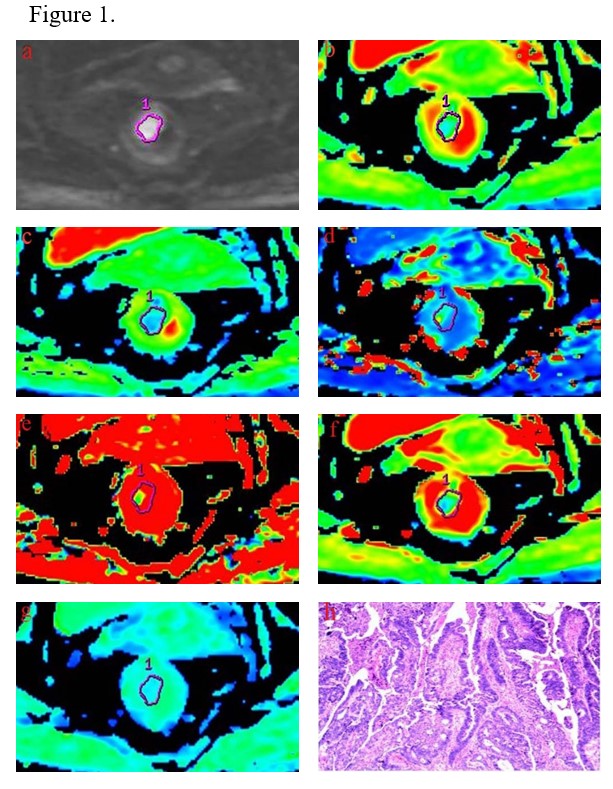
All MR data were transferred to Advantage Workstation (version AW 4.6, GE Medical Systems). IVIM-DWI data were post-processed in ME, BE and SE models with a vendor-provided software (Function tool MADC; GE Healthcare). Parametric mappings of ME-derived apparent diffusion coefficient (ADC), BE-derived true diffusion coefficient (D), pseudo-diffusion coefficient (D*), perfusion fraction (f), SE-derived distributed diffusion coefficient (DDC), and water molecular diffusion heterogeneity index (α) were obtained accordingly. Two radiologists were blinded to the clinical and pathological information, and independently drew the regions of interest (ROI)s. Referring to the T2WI, the regions-of-interest (ROIs) were manually sketched on the largest cross-sectional area of the tumor, excluding necrosis and cystic lesions, on diffusion images at b-value of 1000s/mm2. All ROIs were selected in size between 50 and 500 mm2 (Figure 1).
Statistical analysis
All statistical analyses were performed using SPSS 26.0 (IBM, Armonk, NY, USA) and MedCalc 11.4 (MedCalc, Mariakerke, Belgium). The independent-sample t-test or Mann–Whitney U test was used to compare IVIM parameters between adenoma group and canceration group. The independent risk factors were separated using multivariate binary logistic regression analysis. Receiver operating characteristic (ROC) curve analysis was used to evaluate the diagnostic performance of each parameter by obtaining the area under the ROC curve (AUC), sensitivity, specificity and accuracy. Significant threshold was set as p < 0.05.
Results
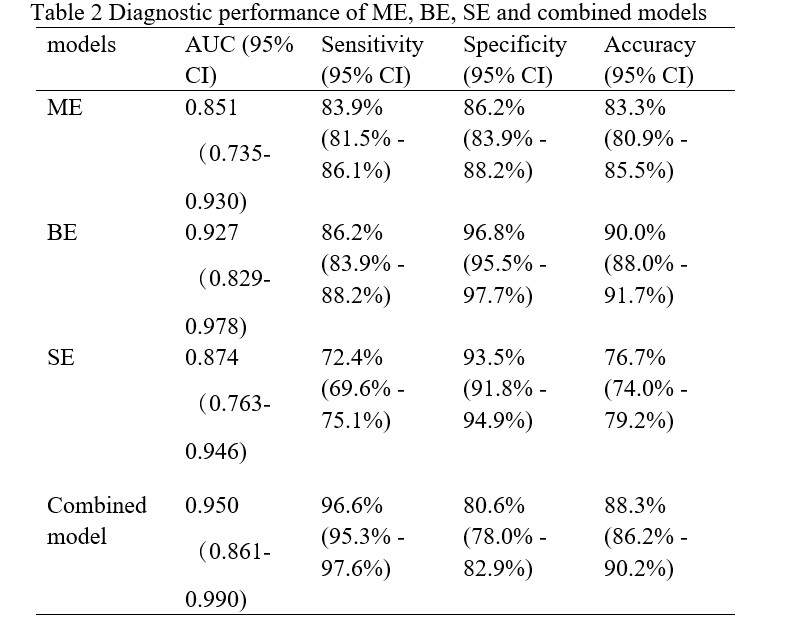
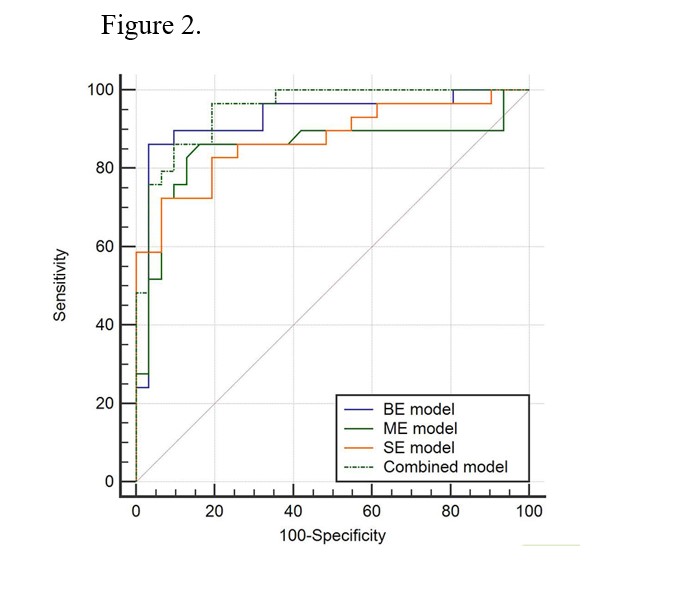
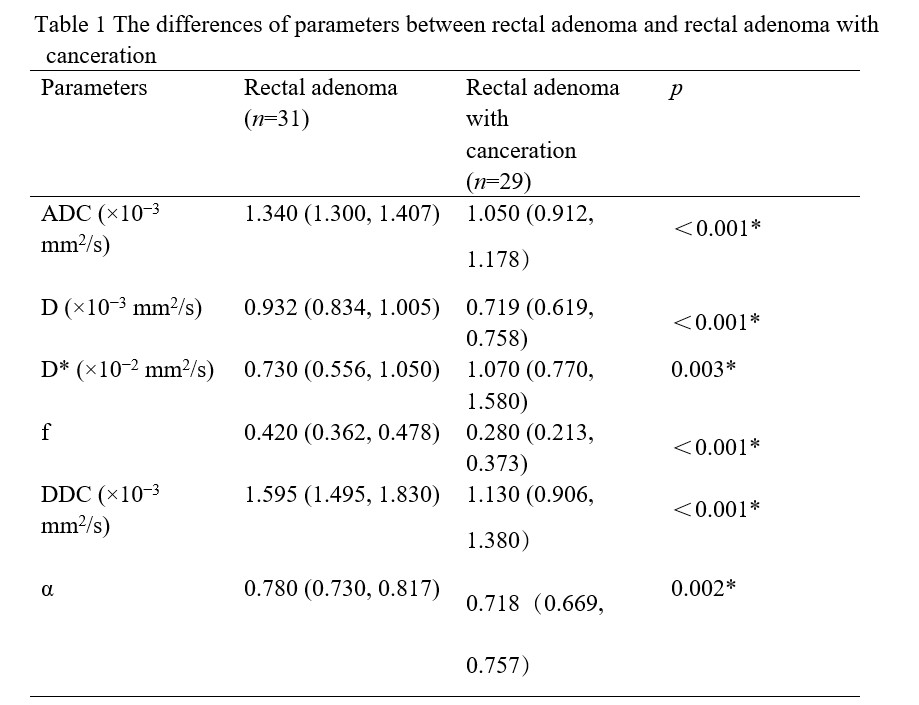
ADC, D, D*, f, DDC and α with intraclass correlation coefficient of 0.929, 0.950, 0.919, 0.912, 0.879, and 0.953 respectively, were proven to achieve excellent measurement repeatability over two radiologists. ADC, D, f, DDC and α showed lower values in canceration patients compared to those without canceration, while an opposite pattern was found in D* value (all p<0.05;Table 1). Moreover, each of ADC, D, f, and DDC values was demonstrated to be an independent risk factor for adenoma canceration (P = 0.011, 0.002, 0.031, and 0.012, respectively). Through ROC analysis, ME, BE, and SE models have showed robust diagnostic efficacies, with respective AUCs of 0.851, 0.927 and 0.874. In terms of diagnosing adenoma canceration, BE model offered a better combination of sensitivity and specificity (86.3% and 96.8%); and the combined model, which included ADC, D, f and DDC, showed the highest sensitivity (96.6%). (Table 2, Figure 2).Discussion and conclusions
In this study, significantly different IVIM parameters of ADC, D, f, and DDC were revealed between adenoma and adenoma with canceration. We speculated that the nuclei of canceration cells are enlarged, the cells are closely arranged, and new blood vessels are increased, thus affecting the dispersion and micro-perfusion. Furthermore, the ME, BE and SEM models employed in this study all provided robust performances in diagnosing adenoma canceration. Among these, ME-derived ADC was considered to be an easy and effective method in predicting adenomas with canceration, and BE model offered a better combination of sensitivity and specificity. In conclusion, ADC values can be used to predict rectal adenomas with canceration. Increasing the complexity of the IVIM-DWI model unable to dramatically increase diagnostic effectiveness.Acknowledgements
My special thanks go to thank Dr. Weiqiang Dou of GE Healthcare for careful review of my dissertation and his valuable comments.References
1.Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7-30.
2. Chan SCH, Liang JQ. Advances in tests for colorectal cancer screening and diagnosis. Expert Rev Mol Diagn. 2022;22(4):449-60.
3. Kouladouros K, Baral J. Transanal endoscopic microsurgical submucosal dissection (TEM-ESD) for recurrent rectal adenomas. Dig Dis. 2022.
4. Chen Y, Li B, Jiang Z, et al. Multi-parameter diffusion and perfusion magnetic resonance imaging and radiomics nomogram for preoperative evaluation of aquaporin-1 expression in rectal cancer. Abdom Radiol (NY). 2022;47(4):1276-90.
5. Le Bihan D, Breton E, Lallemand D, et al. MR imaging of intravoxel incoherent motions: application to diffusion and perfusion in neurologic disorders. Radiology. 1986;161(2):401-7.
6. Zhang Q, Ouyang H, Ye F, et al. Multiple mathematical models of diffusion-weighted imaging for endometrial cancer characterization: Correlation with prognosis-related risk factors. Eur J Radiol. 2020;130:109102.
7. Zhu Q, Ren C, Xu JJ, et al. Whole-lesion histogram analysis of mono-exponential and bi-exponential diffusion-weighted imaging in differentiating lung cancer from benign pulmonary lesions using 3 T MRI. Clin Radiol. 2021;76(11):846-53.
Figures