0058
Free-Breathing Liver Iron Quantification Using 3D Stack-of-Radial GRE Dixon MRI at Two Field Strengths: A Preliminary Study
Xiaodong Zhong1, Stephan A.R. Kannengiesser2, Pedro Itriago Leon3, Vibhas Deshpande4, and Takeshi Yokoo5
1MR R&D Collaborations, Siemens Medical Solutions USA, Inc., Los Angeles, CA, United States, 2MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany, 3MR R&D Collaborations, Siemens Medical Solutions USA, Inc., Dallas, CA, United States, 4MR R&D Collaborations, Siemens Medical Solutions USA, Inc., Austin, CA, United States, 5Department of Radiology and Advanced Imaging Research Center, University of Texas Southwestern Medical Center, Dallas, TX, United States
1MR R&D Collaborations, Siemens Medical Solutions USA, Inc., Los Angeles, CA, United States, 2MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany, 3MR R&D Collaborations, Siemens Medical Solutions USA, Inc., Dallas, CA, United States, 4MR R&D Collaborations, Siemens Medical Solutions USA, Inc., Austin, CA, United States, 5Department of Radiology and Advanced Imaging Research Center, University of Texas Southwestern Medical Center, Dallas, TX, United States
Synopsis
Keywords: Liver, Quantitative Imaging, R2*, Iron, LIC, free-breathing
This study compared free-breathing stack-of-radial and breath-hold Cartesian multi-echo GRE MRI for liver iron quantification at 1.5T and 3T to the reference standard R2-based liver iron concentration (LIC) at 1.5T (FerriScan), in patients at risk for liver iron overload. Agreement was observed for liver iron concentration measured by free-breathing 3D stack-of-radial GRE MRI compared the reference standard R2-based LIC, as well as breath-hold 3D Cartesian GRE MRI. With further validation in larger number of iron-overloaded subjects, 3D stack-of-radial GRE MRI may allow free-breathing R2* and LIC mapping at both 1.5T and 3T.INTRODUCTION
Breath-hold 3D multi-echo Cartesian GRE MRI has been clinically used for liver iron quantification1-3. Its quantification accuracy has been recently validated in a prospective multi-center study at both 1.5T and 3T across multiple vendors, against an FDA-approved R2-based liver iron concentration (LIC) reference standard (FerriScan)4.Pediatric, elderly, and claustrophobic patients often have difficulties cooperating with breath-holding. 3D stack-of-radial imaging has been investigated for liver iron quantification using free-breathing acquisitions5-7. Respiratory motion during free-breathing can contribute to B0 field inhomogeneity and bias R2* quantification, which can be compensated with retrospective self-gating in 3D stack-of-radial imaging5-7. Free-breathing R2* quantification using 3D stack-of-radial MRI has been validated with a 2D biopsy-calibrated R2* relaxometry method at 1.5T8. However, in general it has not been validated at 3T, in the context of LIC and against FerriScan.
The purpose of this study was to compare free-breathing stack-of-radial and breath-hold Cartesian multi-echo GRE MRI for liver iron quantification at 1.5T and 3T to FerriScan LIC at 1.5T, in patients at risk for liver iron overload.
METHODS
In Vivo Liver MRI ExperimentsThis study was HIPAA-compliant and approved by the local IRB. Written informed consent was obtained. Five patients have been referred from the hematology oncology clinic for suspected liver iron overload (2 female, 77.5 ± 6.2 yrs, body mass index 25.4 ± 3.1 kg/m2) were scanned at both 1.5T and 3T (MAGNETOM Sola and Prisma, respectively, Siemens Healthcare, Erlangen, Germany).
Two acquisitions were performed at both field strengths, including a single breath-hold multi-echo 3D Cartesian GRE research application sequence4 and a free-breathing 3D stack-of-radial research application sequence7-9, both covering the whole liver. Whenever possible, the imaging parameters of these two acquisitions kept the same. At 1.5T, free-breathing axial 2D spin-echo images through the central liver sections were acquired at multiple TEs per FerriScan protocol for the reference R2-based LIC quantification. All imaging parameters are listed in Table 1.
Image Reconstruction and Data Analysis
For each subject, scanner-inline DICOM images of the 2D spin-echo acquisitions were sent to an independent core laboratory (Resonance Health), which returned a report with the reference R2-based LIC value. The report included an image of a mid-level liver slice showing the segmented regions of interests (ROIs) used for the R2-based LIC measurement.
Raw data of the breath-hold 3D Cartesian and free-breathing 3D stack-of-radial acquisitions were saved and retrospectively reconstructed offline using the vendor image reconstruction framework to generate DICOM files of echo images and maps, where mono-exponential fitting of magnitude data was used to calculate R2*. To compensate the motion influence on free-breathing stack-of-radial data, self-gating was applied to accept data acquired near end-expiration with a 40% acceptance rate5-6. No noise compensation was performed in the current work.
The ROI placement and analysis were performed by an MRI researcher with more than 10 years of abdominal MRI research experience using ImageJ 1.52n (National Institutes of Health, Bethesda, MD, USA). In the breath-hold 3D Cartesian images and the free-breathing 3D stack-of-radial images at each field strength, the slice shown on the FerriScan report was identified based on the 2nd echo image, and matching ROIs were placed correspondingly with care to avoid vessels and artifacts. LIC maps (unit: mg/g dry tissue) were converted from the R2* maps (unit: s-1) using the equation at 1.5T9: LIC=0.028×R2*-0.45 and at 3T9,10: LIC=0.015×R2*-0.3. LIC values are measured in ROIs and compared to the references using Bland-Altman Analysis with mean difference (MD) and limits of agreement (LoA=MD±1.96×SD).
RESULTS
Figure 1 shows a representative 2D FerriScan LIC map, segmented liver ROI, and corresponding LIC maps from breath-hold Cartesian and free-breathing stack-of-radial sequences at 1.5T and 3T.Because one subject had very high iron overload (>43 mg/g dry tissue as in the FerriScan report) which is beyond the expected dynamic range of both breath-hold Cartesian and free-breathing stack-of-radial methods in this study (Figure 2), this subject was excluded for Bland-Altman analysis.
Figure 3 shows the Bland-Altman agreement plots of the LIC values for breath-hold Cartesian and free-breathing stack-of-radial methods at different field strengths vs the FerriScan LIC values. Additionally, Figure 4 shows agreement between the LIC values by free-breathing 3D stack-of-radial at different field strengths and by breath-hold 3D Cartesian at 1.5T, as well as agreement of the free-breathing 3D stack-of-radial LIC values between 3T and 1.5T.
DISCUSSION AND CONCLUSION
Limitations in this preliminary study includes small number of subjects and incomplete coverage of expected iron overload severity. The clinical study is still ongoing and the final cohort will include a complete range of iron overload severity. The current acquisition protocol generated large errors in a subject with extreme iron overload, due to the insufficient of signal in the acquired echo images (initial TE 0.90 ms at 1.5T). Protocol optimization and further technical refinements may improve iron quantification accuracy in patients with severe and extreme iron overload.In summary, this preliminary study demonstrated agreement of liver iron concentration measured by free-breathing 3D stack-of-radial GRE MRI compared the reference standard R2-based liver iron concentration (FerriScan), as well as breath-hold 3D Cartesian GRE MRI. With further validation in larger number of iron-overloaded subjects, 3D stack-of-radial GRE MRI may allow free-breathing R2* and LIC mapping at both 1.5T and 3T.
Acknowledgements
This study was supported in part by Siemens Medical Solutions USA, Inc. We thank Michael Fulkerson for coordinating this study at the University of Texas Southwestern Medical Center.References
1. Yu H, Shimakawa A, McKenzie CA, Brodsky E, Brittain JH, Reeder SB. Multiecho water‐fat separation and simultaneous R2* estimation with multifrequency fat spectrum modeling. Magn Reson Med. 2008;60:1122-1134.2. Hernando D, Levin YS, Sirlin CB, Reeder SB. Quantification of liver iron with MRI: state of the art and remaining challenges. J Magn Reson Imaging. 2014;40:1003-1021.
3. Zhong X, Nickel MD, Kannengiesser SAR, Dale BM, Kiefer B, Bashir MR. Liver fat quantification using a multi‐step adaptive fitting approach with multi‐echo GRE imaging. Magn Reson Med. 2014;72:1353-1365.
4. Hernando D, Zhao R, Yuan Q, Aliyari Ghasabeh M, Ruschke S, Miao X, Karampinos DC, Mao L, Harris DT, Mattison RJ, Jeng MR, Pedrosa I, Kamel IR, Vasanawala S, Yokoo T, Reeder SB. Multicenter Reproducibility of Liver Iron Quantification with 1.5-T and 3.0-T MRI. Radiology 2022:213256. doi: 10.1148/radiol.213256. Epub ahead of print.
5. Zhong X, Armstrong T, Nickel MD, et al. Effect of respiratory motion on free‐breathing 3D stack‐of‐radial liver R2* relaxometry and improved quantification accuracy using self-gating. Magn Reson Med 2020;83:1964-1978.
6. Zhong X, Hu HH, Armstrong T, Li X, Lee YH, Tsao TC, Nickel MD, Kannengiesser SAR, Dale BM, Deshpande V, Kiefer B, Wu HH. Free-breathing volumetric liver R2* and proton density fat fraction quantification in pediatric patients using stack-of-radial MRI with self-gating motion compensation. 2021;53:118-129.
7. Armstrong T, Zhong X, Shih SF, Felker E, Lu DS, Dale BM, Wu HH. Free-breathing 3D stack-of-radial MRI quantification of liver fat and R2* in adults with fatty liver disease. Magn Reson Imaging 2022;85:141-152.
8. Rohani SC, Morin CE, Zhong X, Kannengiesser S, Shrestha U, Goode C, Holtrop J, Khan A, Loeffler RB, Hankins JS, Hillenbrand CM, Tipirneni-Sajja A. Hepatic Iron Quantification Using a Free-Breathing 3D Radial Gradient Echo Technique and Validation With a 2D Biopsy-Calibrated R2* Relaxometry Method. J Magn Reson Imaging 2022;55:1407-1416.
9. Hankins JS, McCarville MB, Loeffler RB, Smeltzer MP, Onciu M, Hoffer FA, Li CS, Wang WC, Ware RE, Hillenbrand CM. R2* magnetic resonance imaging of the liver in patients with iron overload. Blood 2009;113:4853-4855.
10. Storey P, Thompson AA, Carqueville CL, Wood JC, de Freitas RA, Rigsby CK. R2* imaging of transfusional iron burden at 3T and comparison with 1.5T. J Magn Reson Imaging 2007;25:540-547.
11. Breuer FA, Blaimer M, Mueller MF, Seiberlich N, Heidemann RM, Griswold MA, Jakob PM. Controlled aliasing in volumetric parallel imaging (2D CAIPIRINHA). Magn Reson Med 2006;55:549-556.
Figures
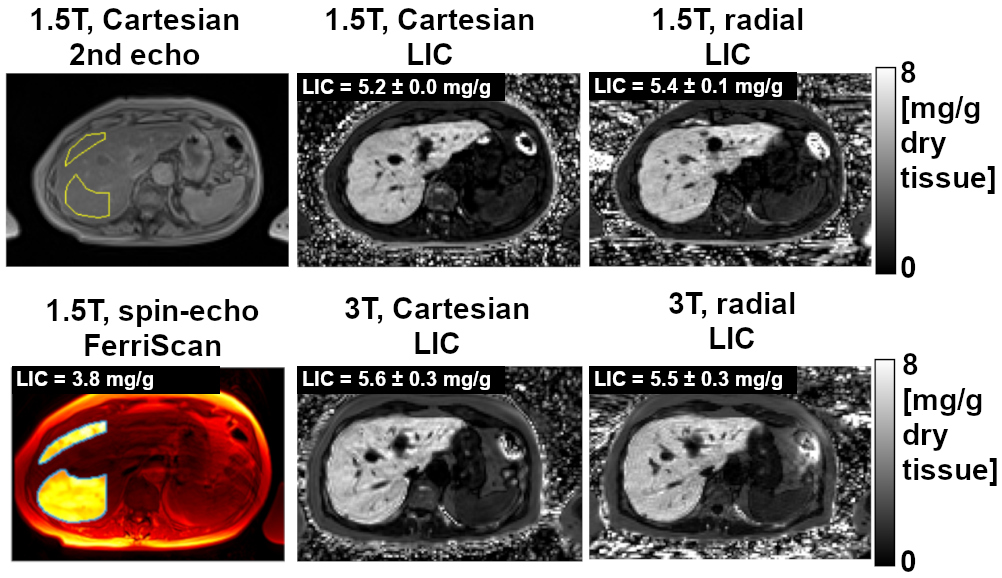
Figure 1
Representative 2D FerriScan
LIC map, segmented liver ROI, and corresponding LIC maps from breath-hold Cartesian
and free-breathing stack-of-radial sequences at 1.5T and 3T of one patient.
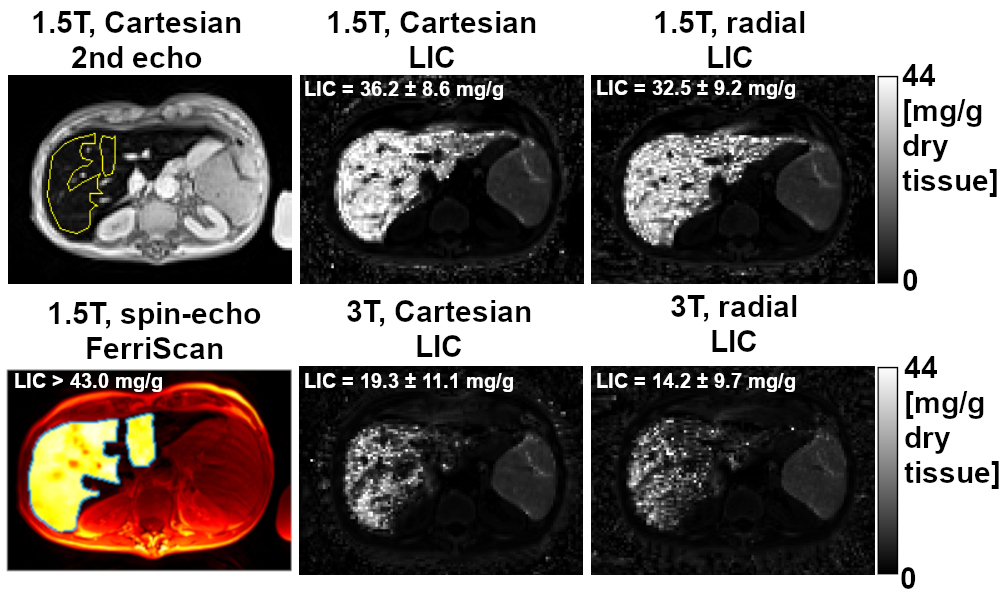
Figure 2
2D FerriScan
LIC map, segmented liver ROI, and corresponding LIC maps from breath-hold Cartesian
and free-breathing stack-of-radial sequences at 1.5T and 3T of one patient with
very high iron overload. This patient was excluded from Bland-Altman analysis.
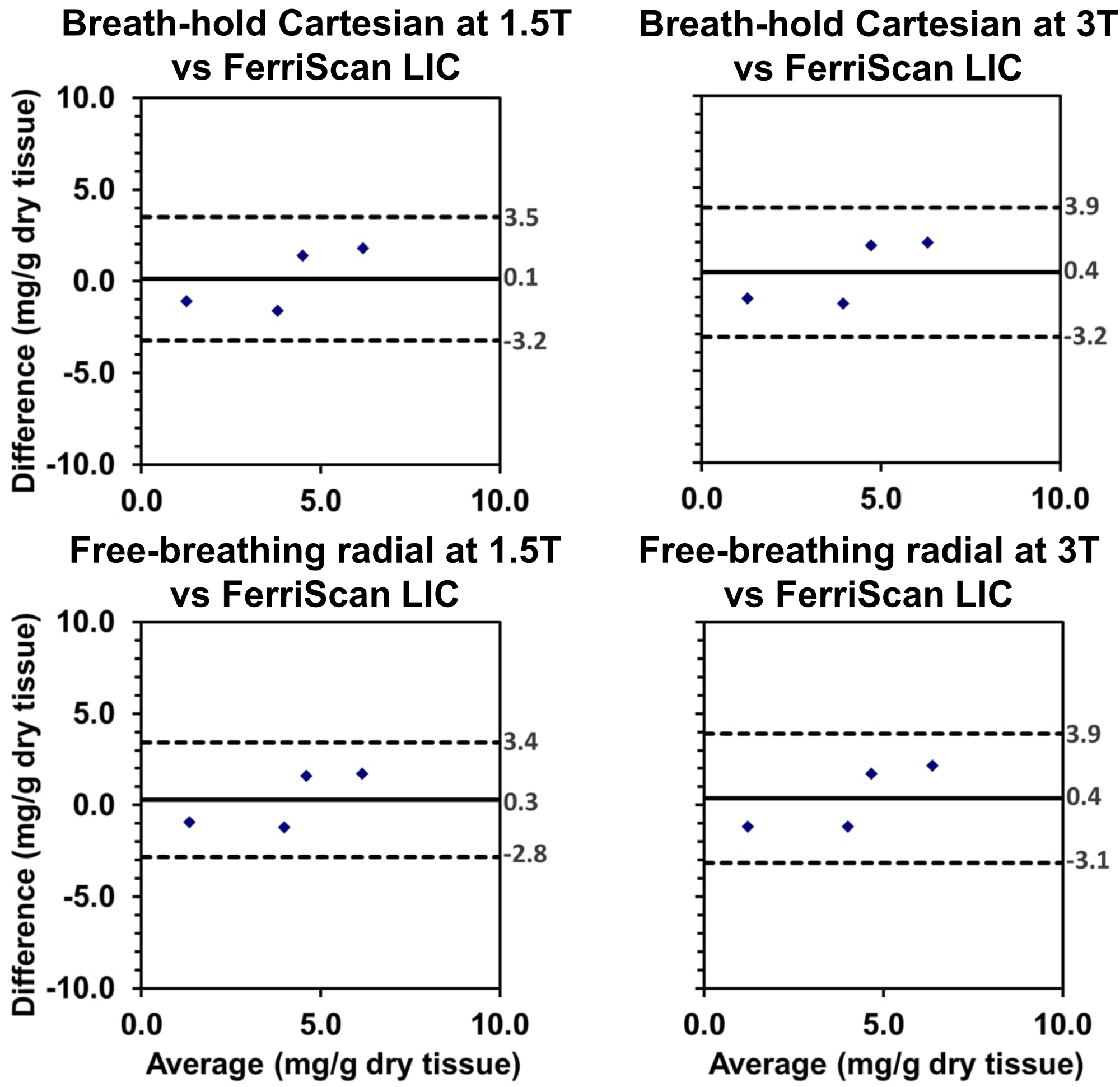
Figure 3
Bland-Altman plots between the LIC values measured by breath-hold 3D
Cartesian and free-breathing 3D stack-of-radial at different
field strengths vs the R2-based LIC values.
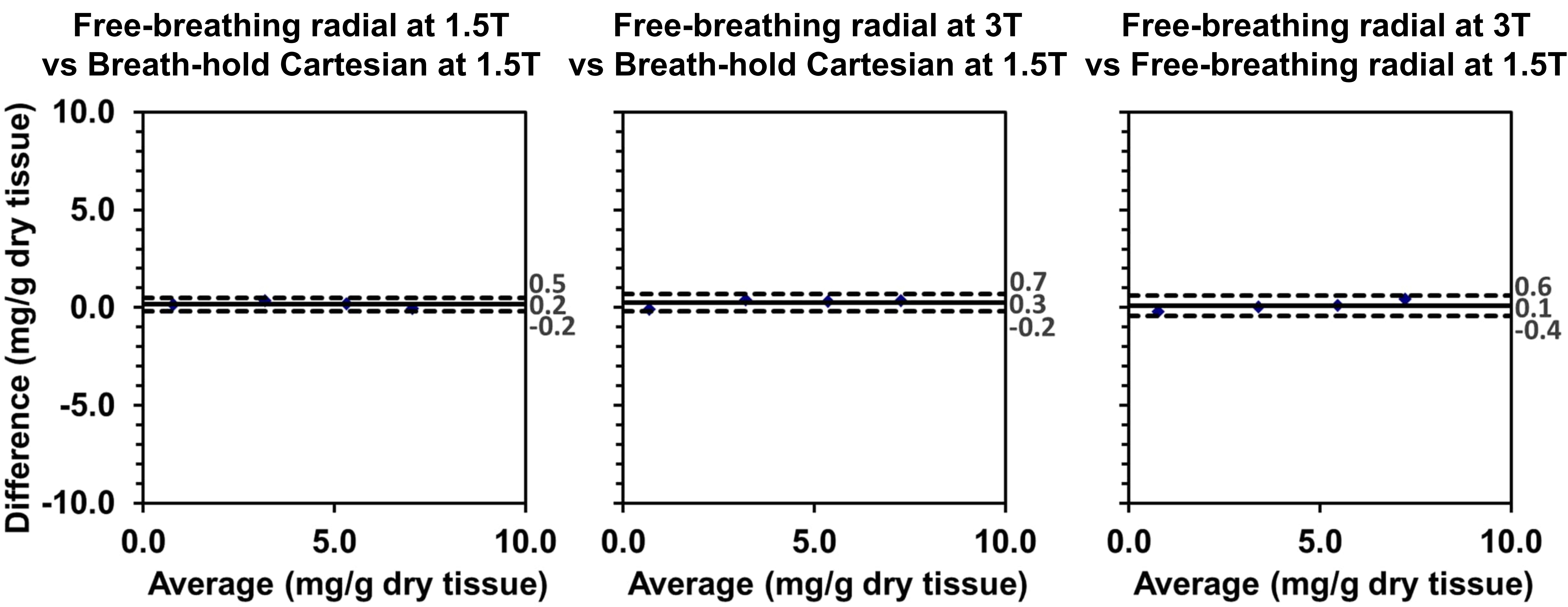
Figure 4
Bland-Altman plots between the LIC values measured by free-breathing 3D stack-of-radial at different field strengths and the LIC values measured by breath-hold 3D Cartesian
at 1.5T, as well as the LIC values by free-breathing
3D stack-of-radial at 3T and 1.5T.
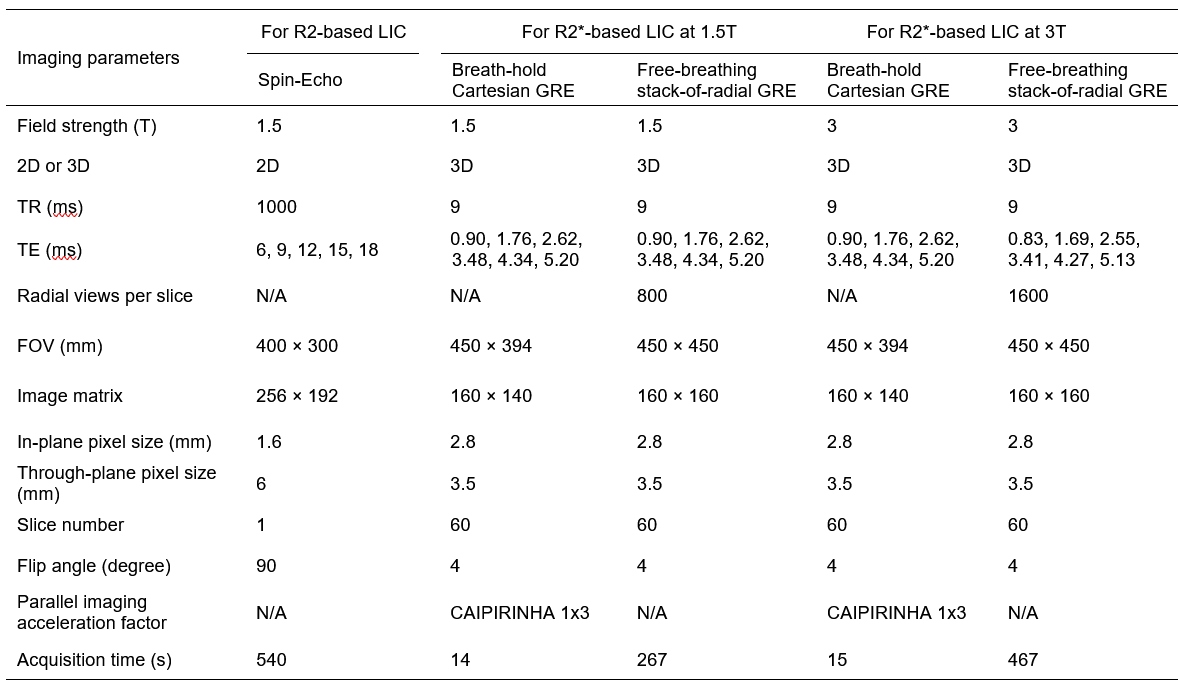
Table
1 Imaging parameters of the protocols
used in this study. N/A:
Not applicable. CAIPIRINHA: Two-dimensional parallel imaging as described in11.
DOI: https://doi.org/10.58530/2023/0058