5067
Reductin of cervical motion and ADC inaccuracy by use of neck fixation device for DWIBS Imaging1National Hospital Organization Ibarakihigashi Hospital, Toukai, Japan, 2Graduate School of Ibaraki Prefectural University of Health Sciences, Ami, Japan, 3National Hospital Organization Mito Medical Center, Ibaraki-machi, Japan
Synopsis
The effectiveness of a neck fixation device to improve the image quality of DWIBS was investigated. Healthy volunteers were examined while chewing with and without a neck fixation device using 3-T MRI system. The amount of mandibular bone movement and the ADC values of some body parts were decreased by the fixation device. These are thought to improve the image quality and the ADC measurement accuracy. The technique using a neck fixation device helps improve image quality of DWIBS in the head and neck region.
Background and purpose
In recent years, the use of diffusion-weighted whole body imaging with background suppression (DWIBS) has increased worldwide, and it is useful for cancer screening. However, in DWIBS imaging, some artifacts often appear at the head and neck region due to magnetic field inhomogeneity caused by the complicated body shape and chewing motion. Moreover, these artifacts also affect the accuracy of apparent diffusion coefficient (ADC) values. The ADC reflects histological and physiological characteristics and plays an important role in the diagnosis of disease. The Quantitative Imaging Biomarkers Alliance (QIBA) of the Radiological Society of North America (RSNA) has established criteria for changes in the ADC with a 95% confidence interval. Therefore, technologists need to perform DWIBS with minimal artifacts to enable more accurate ADC measurements even in the head and neck. In this study, the effectiveness of a neck fixation device to improve the image quality of DWIBS was investigated.Methods
Ten healthy volunteers who agreed to this study conducted with the approval of our Institutional Review Board were recruited. Magnetic resonance imaging (MRI) was performed with a 3-T MRI system (MAGNETOM skyra, Siemens, Erlangen, Germany). Images were acquired while the participants were chewing with and without a neck fixation device. The neck fixation device used in this study was a combination of a commercially available neck collar (Stiffneck Select, Laerdal Medical, Tokyo, Japan) and a bag filled with polyacetal beads (Fig. 1). (1) The maximum displacement of the mandibular bone was measured on the cine image of true fast imaging with steady-state precession (trueFISP). The imaging parameters of trueFISP were as follows: repetition time (TR) 3.8 ms; echo time (TE) 1.88 ms; flip angle (FA) 60 degrees; field of view (FOV) 327 mm; matrix size 256×256; slice thickness 10 mm; number of averages = 1; and temporal resolution 1.44 s. (2) The ADC values of the submandibular glands, lymph nodes, second cervical vertebra, and upper thoracic vertebra were measured on the DWIBS source images. The imaging parameters of DWIBS were as follows: pulse sequence spin echo type echo planar imaging; TR 8060 ms; TE 49 ms; FOV 450 mm; matrix size 128×128; slice thickness 5 mm; number of averages 3; and b-value 1000 s/mm2.Results
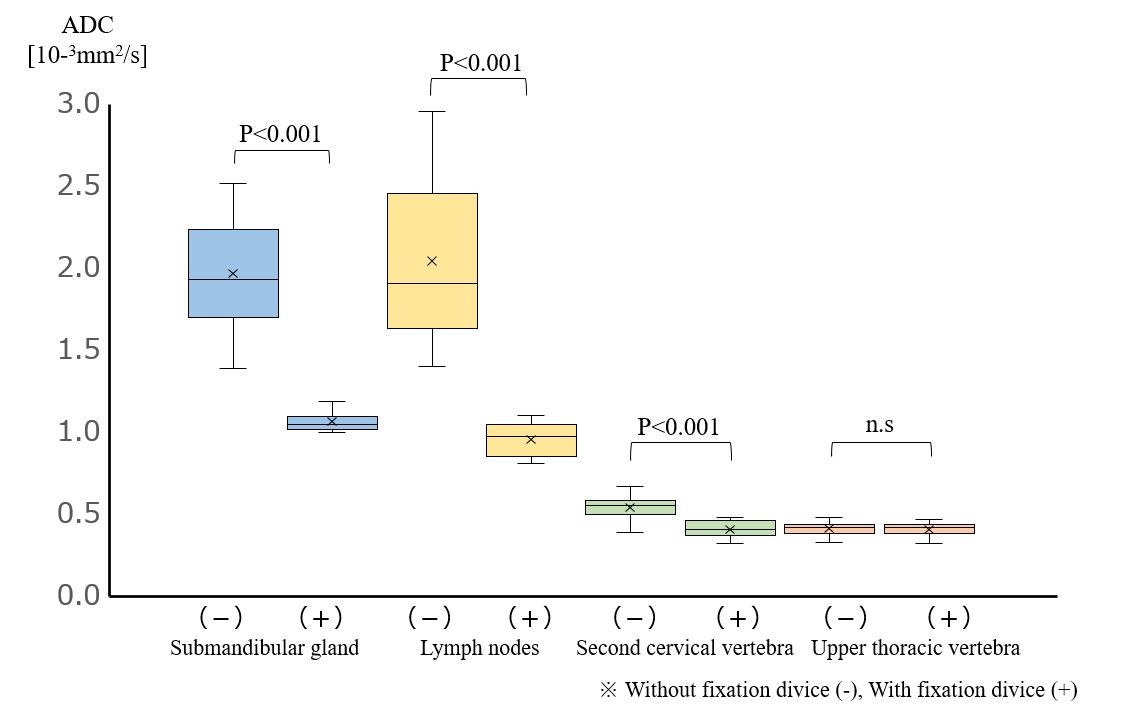
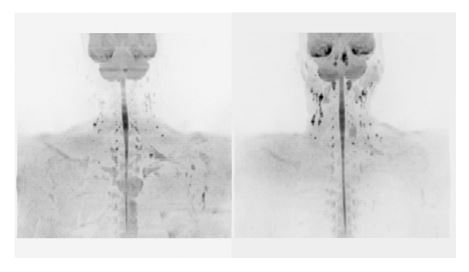
Without the fixation device, the distance the mandibular bone moved was 14.4 ± 3.9 mm in the vertical direction, 14.9 ± 3.9 mm in the anterior-posterior direction, and 3.0 ± 0.8 mm in the left-right direction. With the fixation device, the distances were 1.3 ± 0.5 mm, 1.2 ± 0.6 mm, and 0.4 ± 0.1 mm, respectively. Without the fixation device, the ADC [10-3mm2/s] values were 1.97 ± 0.06 in the submandibular gland, 2.05 ± 0.50 in the lymph nodes, 0.54 ± 0.08 in the second cervical vertebra, and 0.41 ± 0.04 in the upper thoracic vertebra. With the fixation device, they were 1.07 ± 0.06, 0.96 ± 0.10, 0.41 ± 0.05, and 0.41 ± 0.05, respectively. There were significant differences (p<0.001) between the values with and without the fixation device, but no significant difference was found in the thoracic vertebra (Fig. 2). Representative DWIBS images are shown in Figure 3. Visualization of the cervical lymph nodes improved significantly with the fixation device.Conclusions
The distance that the mandible moved with chewing was large in the vertical and anterior-posterior directions and could be greatly reduced by the fixation device. The ADC values were significantly decreased with the fixation device, except for the thoracic vertebra. These changes are thought to have improved image quality and ADC measurement accuracy. This technique using a neck fixation device helps improve the image quality of DWIBS in the head and neck region.Acknowledgements
The authors would like to thank Dr. Usui and his staff at the Department of Radiology of Ibarakihigashi Hospital. The authors would also like to thank the staff of the radiology department of Mito Medical Center.References
1. QIBA profile: Diffusion-weighted magnetic resonance imaging (DWI). http://qibawiki.rsna.org/images/6/63/QIBA_DWIProfile_Consensus_Dec2019_Final.pdf
2. Takahara T, Imai Y, Yamashita T, et al. Diffusion weighted whole body imaging with background body signal suppression (DWIBS): technical improvement using free breathing, STIR and high resolution 3D display. Radiat Med. 2004; 22:275–282.
3. Moriya S, Miki Y, Yokobayashi T, et al. Improved CHESS imaging with the use of rice pads : Investigation in the neck, shoulder, and elbow. J Magn Reson Imaging. 2010; 31(6)1504-1507.
Figures