Sikandar Shaikh1,2,3
1Department of Radiodiagnosis, Shadan Institute of Medical Sciences.. Hyderabad. India, Hyderabad, India, 2Department of Radiodiagnosis, Kasturba Medical College, Manipal, India, 3Department of Biomedical Engineering, Indian Institute of Technology, Hyderabad, India
Synopsis
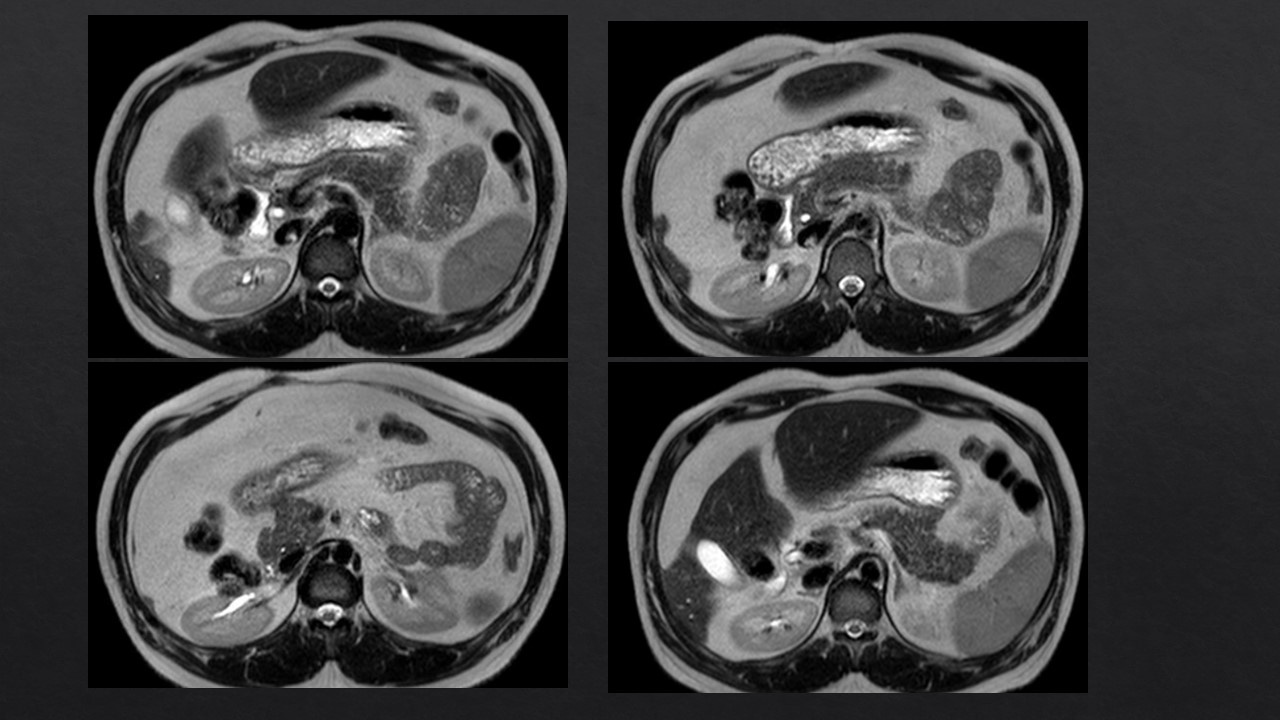
MRI is the important modality for the evaluation of
the Pancreas. It has significant role in the evaluation of various pancreatic pathologies
comprising of the congenital, infective, inflammation, neoplastic, traumatic,
and miscellaneous pathologies. This is also important screening tool for differentiating
the indeterminate pancreatic focal lesions like focal pancreatitis versus
neoplastic. MRI using magnetic resonance cholangiopancreatography (MRCP) also evaluates
associated hepatobiliary pancreatic
pathologies. Due to technical advances
in MRI, newer sequences as well as protocols like diffusion-weighted and
T1-weighted dynamic contrast-enhanced MRI are used despite of various challenges of
retroperitoneal location of the Pancreas.
Acknowledgements
Dr. Bhuchandi References
1. Ma J, Son JB, Zhou Y, et al. Fast spin-echo
tripleecho Dixon (fTED) technique for efficient T2- weighted water and fat
imaging. Magn Reson Med 2007;58:103–9.
2.Bayramoglu S, Kilickesmez O, Cimilli T, et al. T2-
weighted MRI of the upper abdomen: comparison of four fat-suppressed
T2-weighted sequences including PROPELLER (BLADE) technique. Acad Radiol
2010;17(3):368–74. [Epub 2009 Dec 30].
3.Nanko S, Oshima H, Watanabe T, et al. Usefulness of
the application of the BLADE technique to reduce motion artifacts on
navigation-triggered prospective acquisition correction (PACE) T2-weighted MRI
(T2WI) of the liver. J Magn Reson Imaging 2009; 30:321–6.
4.Hirokawa Y, Isoda H, Maetani YS, et al. Evaluation
of motion correction effect and image quality withthe periodically rotated
overlapping parallel lines with enhanced reconstruction (PROPELLER) (BLADE) and
parallel imaging acquisition technique in the upper abdomen. J Magn Reson
Imaging 2008;28:957–62.
5.Purysko AS, Gandhi NS, Walsh RM, Obuchowski NA,
Veniero JC. Does secretin stimulation add to magnetic resonance
cholangiopancreatography in characterising pancreatic cystic lesions as
side-branch intraductal papillary mucinous neoplasm? Eur Radiol
2014;24(12):3134-3141.
6.Canto MI, Harinck F, Hruban RH, et al. International
cancer of the pancreas screening (CAPS) consortium summit on the management of
patients with increased risk for familial pancreatic cancer. Gut
2013;62(3):339-347.
7.Jang KM, Kim SH, Kim YK, Song KD, Lee SJ, Choi D.
Missed pancreatic ductal adenocarcinoma: Assessment of early imaging findings
on prediagnostic magnetic resonance imaging. Eur J Radiol 2015;84(8):1473-1479.
8.Corrias G, Raeside MC, Agostini A, et al. Pilot
study of rapid MR pancreas screening for patients with BRCA mutation. Eur
Radiol 2019;29 (8):3976-3985.
9.Corral JE, Mareth KF, Riegert-Johnson DL, Das A,
Wallace MB. Diagnostic yield from screening asymptomatic individuals at high
risk for pancreatic cancer: A meta-analysis of cohort studies. Clin
Gastroenterol Hepatol 2019;17(1):41-53.
10.Henrikson NB, Aiello Bowles EJ, Blasi PR, et al.
Screening for pancreatic cancer: Updated evidence report and systematic review
for the US preventive services task force. JAMA 2019;322(5):445-454.
11.Schawkat K, Eshmuminov D, Lenggenhager D, Endhardt
K, Vrugt B, Boss A, et al. Preoperative Evaluation of Pancreatic Fibrosis and
Lipomatosis: Correlation of Magnetic Resonance Findings With Histology Using
Magnetization Transfer Imaging and Multigradient Echo Magnetic Resonance
Imaging. Investigative radiology. 2018; 53(12):720–7.