High-Dimensional Cardiovascular MR: Simplifying Clinical Scans
Matthias Stuber1
1University Hospital Lausanne, Lausanne, Switzerland
1University Hospital Lausanne, Lausanne, Switzerland
Synopsis
This presentation discusses alternative approaches to cardiac MRI that are time-efficient, operator-independent and easy-to-use. These shift the paradigm from a prospective scan parameter adjustment and scan plane planning to an entirely retrospective query of the data.
High-Dimensional Cardiovascular MR: Simplifying Clinical ScansMatthias Stuber, PhD Magnetic resonance imaging (MRI) is an extremely powerful modality to probe the health of the heart, its tissues, its vessels, its blood-flow, and even its metabolism. This makes MRI not only unique for gaining new biological and biomechanical research insights related to the cardiovascular system, but it also provides an exquisite non-invasive tool for diagnosis and to help guide decision making and therapy in patients with cardiovascular disease. And cardiovascular disease still remains the leading cause of mortality in industrialized nations while the associated morbidity leads to considerable downstream costs. Over the past decades, we have witnessed that MR can increasingly provide comprehensive information about the heart, while the extraction of quantitative information has become paramount to help advance individualized precision medicine. Cardiovascular MR techniques have become more and more sophisticated - to a very large degree also owing to the staggering combined innovation- and engineering power of the ISMRM membership. In fact, imaging of the heart using MR has been and will always be an exquisite engineering challenge simply because there is the added complication of cardiac and respiratory motion, the concomitant need for high spatial resolution and speed, and the rather complex 3D anatomy of the heart that must be accounted for. ECG triggering, segmented k-space acquisition, breath holding, bSSFP imaging, navigators, and narrow data acquisition windows have become mainstays for motion suppression while coil arrays and parallel imaging have critically enabled rapid whole heart acquisitions. Contrast agents in turn have led to perfusion imaging, the visualization of scar tissue, and to the quantification of the extracellular volume fraction. For ECG triggered sequences with interspersed wait periods to account for data collection during the most quiescent time point in the cardiac cycle, time efficiency suffers on the one hand, but it helps maximize steady-state magnetization in favor of SNR and invites pre-pulse concepts on the other. As for time efficiency, the duty cycle (signal sampling time relative to total scan time) of a triggered cardiac sequence is often 2% or below. As for pre-pulses, this offers a multitude of options to enhance tissue contrasts and particularly enables perfusion imaging, scar imaging, tissue mapping etc. Together with a meticulous approach to a double oblique scan plane prescription to account for the individual heart’s anatomy, and sometimes tedious ECG lead placement to optimize the quality of synchronization between the heartbeat and the imaging sequence, taken together this spans an enormous parameter space. However, this adds complexity, affects ease-of-use, and unfortunately promotes operator dependency. And these factors are among the chief hindrances to a broader dissemination of cardiovascular MRI.
To remove these hurdles, several groups have developed new cardiac MRI paradigms where ECG lead placement, complex scan planning, repeated breath-holding, and time in-efficient acquisitions have been replaced by a free-running image acquisition, where more anatomical and functional information from the heart is collected per unit time than was previously possible, where one single mouse click suffices to initiate a scan, and where a fully flexible and retrospective 3D interrogation of the heart’s anatomy, function, and flow is enabled. What makes this also unique is that data are now collected during free breathing with continuous uninterrupted RF excitations and signal readouts irrespective of the heart’s contractile state or its respiratory position. This improves the duty cycle 15-fold and with the advent of compressed sensing, it enables cardiac- and respiratory motion-resolved 3D imaging of the heart (=5D imaging), where adding a 6th contrast dimension is currently an active field of research. Probing and querying such datasets for relevant information provides ample opportunity for research, discovery, and for finding clinical answers. First results obtained in patients are discussed. At our institution and at our partner sites, this approach has even helped remove the need for anesthesia in a certain age bracket of pediatric congenital heart disease patients.
To remove these hurdles, several groups have developed new cardiac MRI paradigms where ECG lead placement, complex scan planning, repeated breath-holding, and time in-efficient acquisitions have been replaced by a free-running image acquisition, where more anatomical and functional information from the heart is collected per unit time than was previously possible, where one single mouse click suffices to initiate a scan, and where a fully flexible and retrospective 3D interrogation of the heart’s anatomy, function, and flow is enabled. What makes this also unique is that data are now collected during free breathing with continuous uninterrupted RF excitations and signal readouts irrespective of the heart’s contractile state or its respiratory position. This improves the duty cycle 15-fold and with the advent of compressed sensing, it enables cardiac- and respiratory motion-resolved 3D imaging of the heart (=5D imaging), where adding a 6th contrast dimension is currently an active field of research. Probing and querying such datasets for relevant information provides ample opportunity for research, discovery, and for finding clinical answers. First results obtained in patients are discussed. At our institution and at our partner sites, this approach has even helped remove the need for anesthesia in a certain age bracket of pediatric congenital heart disease patients.
Acknowledgements
No acknowledgement found.References
No reference found.Figures
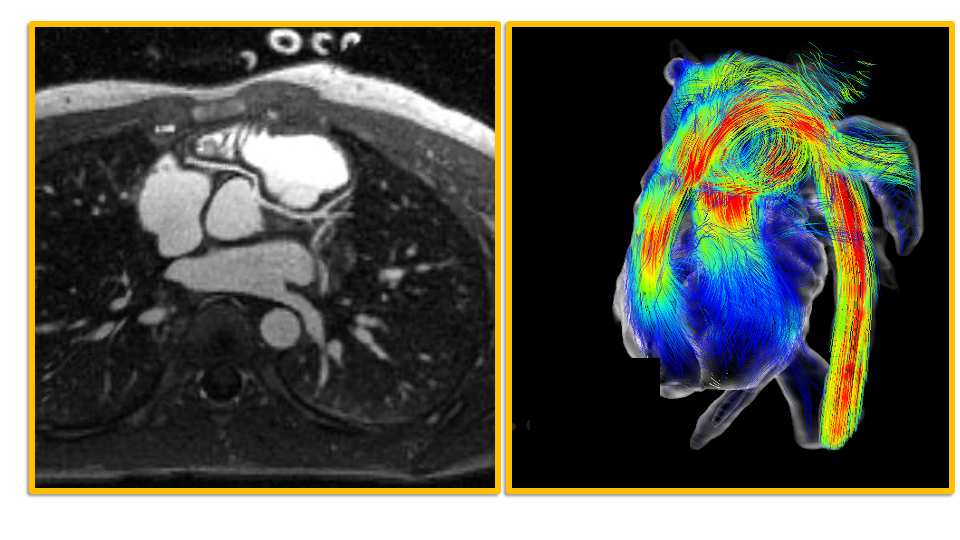
Coronary MRA of a patient with an anomalous right coronary artery on the left and flow data obtained from another patient on the right. Both images were acquired with the fully self-gated free-running framework (FRF: Di Sopra L. et al.: Magn Reson Med. 2019 Dec;82(6):2118-2132 and Ma L. et al.: Radiol Cardiothorac Imaging. 2020 Nov 12;2(6)) that promotes time-efficient 5D imaging using one single mouse click. Images courtesy M. Fogel, K. Whitehead, M. Falcao.