4964
High White Matter Fractional Anisotropy and Low Diffusivity in Participants with Post-acute Sequelae SARS-CoV-2 Infection1Diagnostic Radiology and Nuclear Medicine, University of Maryland School of Medicine, Baltimore, MD, United States, 2Department of Neurology, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 3Department of Radiology, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 4Institute of Human Virology, Department of Medicine, Division of Infectious Disease, University of Maryland School of Medicine, Baltimore, MD, United States, 5Department of Medicine, Division of Pulmonary & Critical Care Medicine, University of Maryland School of Medicine, Baltimore, MD, United States, 6Department of Neurology, University of Maryland School of Medicine, Baltimore, MD, United States
Synopsis
Diffusion tensor imaging (DTI), a sensitive method to detect inflammatory or cytotoxic tissue changes, has been used to study brain microstructure in patients with COVID-19. At 2-3 months post-acute sequelae SARS-CoV-2 infection (PASC), prior reports found both higher or lower than normal white matter diffusivity in participants who had variable severity of clinical manifestations. We performed DTI and neuropsychiatric assessments in 20 participants with PASC. Individuals with PASC had lower diffusivity 6 months after the diagnosis, which correlated with greater fatigue. These diffusion findings may be due to glial proliferation and immune-response related cytotoxic edema.
INTRODUCTION
SARS-CoV-2 causes COVID-19, and one third of infected individuals would have a neurological or psychiatric diagnosis within 6 months, with higher prevalence among those with a severe clinical course.1 However, even patients with milder COVID-19 can have persistent neuropsychiatric symptoms, such as fatigue, concentration problems (“brain fog”), headache, anosmia, hypogeusia, anxiety and emotional stress.2,3 The mechanisms behind these symptoms are unclear but may involve thromboembolic and inflammatory processes.3 Neuroinflammation can induces white matter (WM) microstructure changes such as demyelination and glia cell proliferation. Diffusion tensor imaging (DTI) can detect such microstructural changes by measuring the diffusivity of water molecules. WM fiber anisotropy diffusion was either higher 4,5or lower 6,7 in individuals with post-acute sequelae SARS-CoV-2 infection (PASC) at 2-3 months after the infection. Therefore, we aimed to examine white matter microstructure integrity in individuals at least 6 weeks after the diagnosis of COVID-19. We hypothesized that convalescent COVID-19 participants would have ongoing or residual neuroinflammation and hence higher diffusivity and lower fractional anisotropy (FA) in the brain WM compared to uninfected controls.METHODS
Thirty-six participants [20 uninfected controls (8 men) and 16 with PASC (7 men)] completed neuropsychiatric evaluations and brain MRI scan. DTI was acquired on a 3T Siemens scanner, using a spin-echo echo-planar sequence (TR/TE = 18000/ 91ms, in-plane resolution 2.5 × 2.5 mm, thickness = 2.5 mm, four b=0 scans, 30 directions with b=1000s/mm2). DTI data were processed on MRICloud (http://www.MRICloud.org).8,9 FA, mean diffusivity (MD), radial diffusivity (RD), and axial diffusivity (AD) were obtained from 9 major WM fiber tracts and 6 subcortical grey matter regions (Figures 1-2).NIH Toolbox® (NIHTB) using the Cognition and Motor batteries, and Patient-Reported Outcomes Measurement (PROMIS®, Pain Interferenc, Fatigue, and Psychological Well-being modules) were collected and evaluated in relation to the DTI metrics. ANCOVAs were used to compare DTI measures between controls and PASC, covarying for age, sex, and index of social position (ISP). Linear regression was used to explore the associations between regional FA/ MD, duration since COVID diagnosis and the NIHTB and PROMIS measures that show significant group differences.
RESULTS
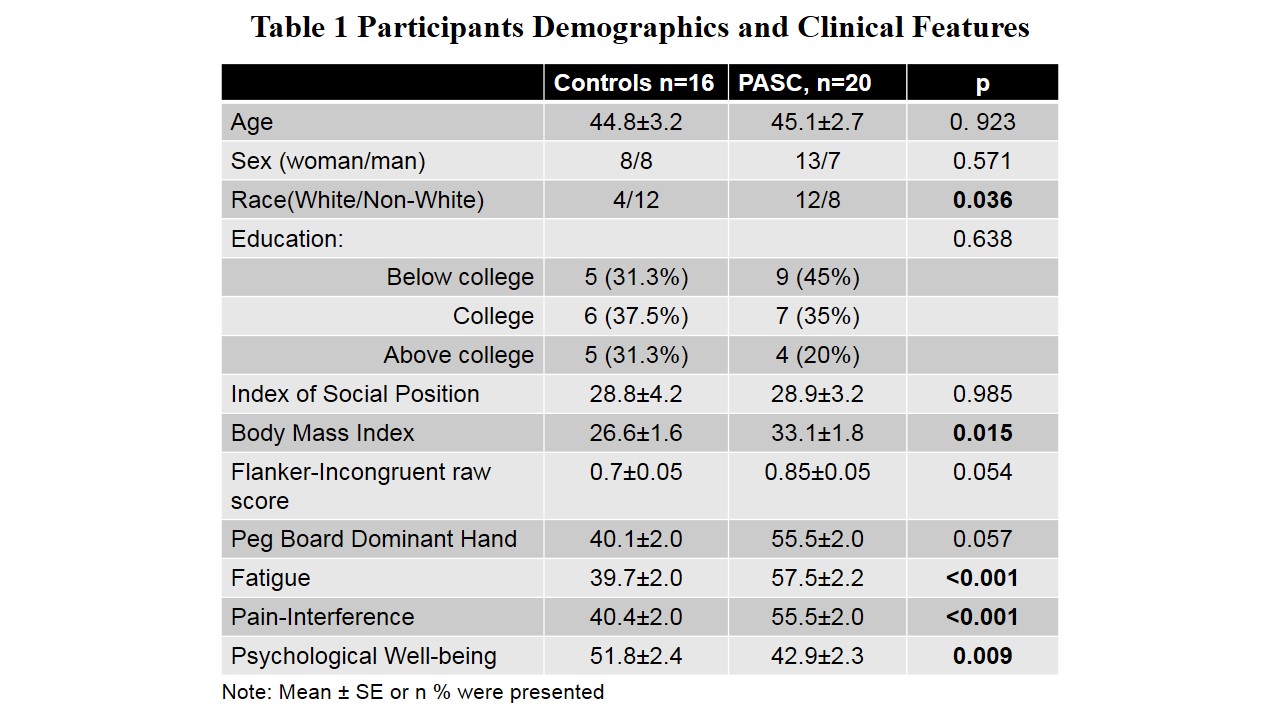
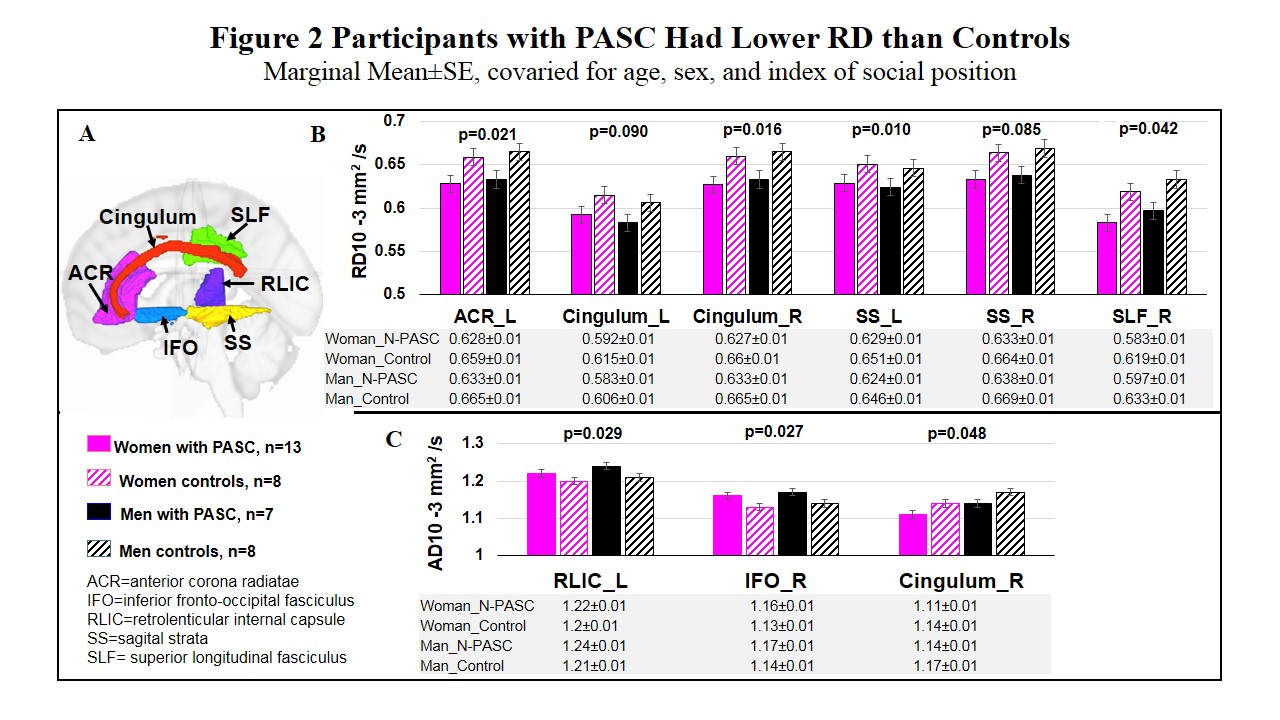
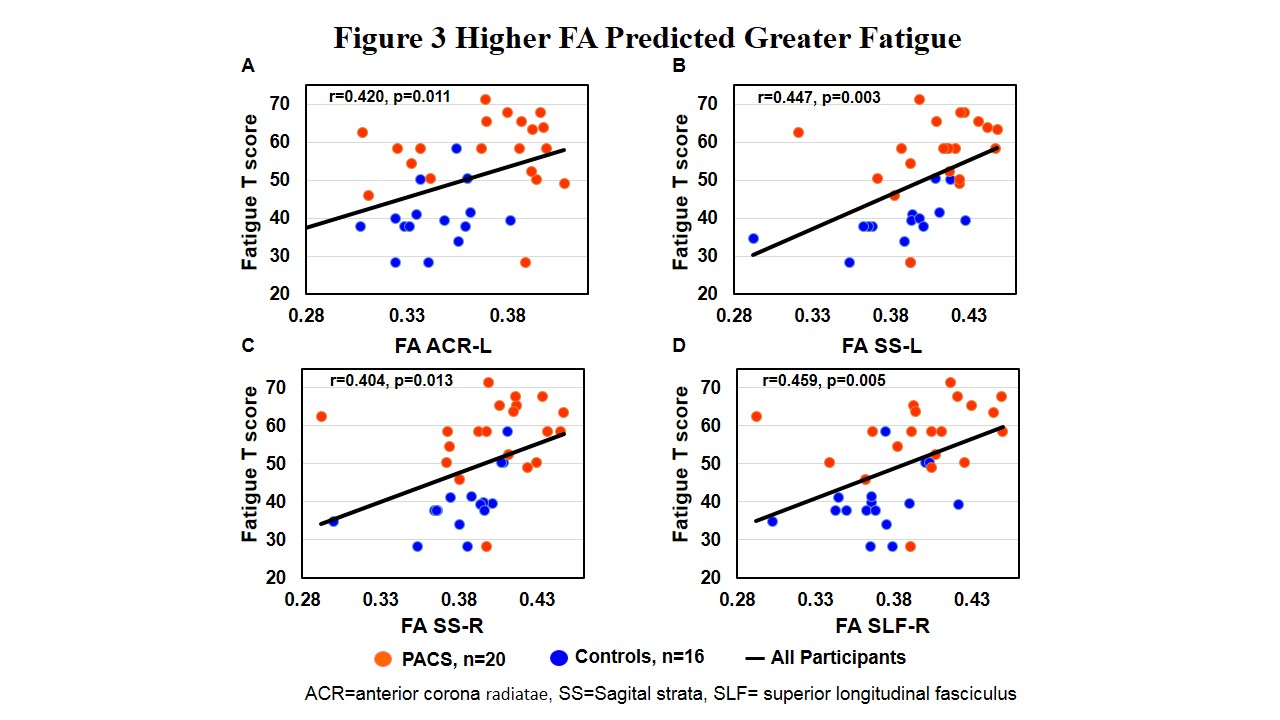
Participants in the two groups had similar age, education level, index of social position, and sex distribution; however, the PASC group was less diverse in race/ethnicity (p=0.036) and had higher body mass index (+24.4%, p=0.015) than controls. The PASC participants were diagnosed with COVID-19 158 days (median, range: 41-399 days) prior to the study. The most common neurological symptoms were fatigue (92%), difficulty with concentration (85%) and memory (85%). Compared with controls, participants with PASC tended to have slower processing speed (Flanker-Incongruent, p=0.054) and slower motor function (Peg Board Dominant hand, p=0.057), as well as higher level of fatigue (p<0.001), more Pain-Interference (p<0.001) and lower score on psychological well-being (p=0.009) (Table 1).On DTI, participants with PASC had higher FA in the bilateral anterior corona radiatae (ACR, left p=0.001; right p=0.033), bilateral sagittal strata (SS; left: p=0.027; right: p=0.045) and right superior longitudinal fasciculus (SLF, p=0.014) (Figure 1A), and lower MD in the right SLF (p=0.029) (Figure 1B) and bilateral cingulum than controls (left p=0.048; right p=0.003). Higher FA and lower MD were driven by the lower RD in the PASC group compared to controls (Figure 2B). In addition, participants with PASC had higher AD in the retrolenticular internal capsule-left (p=0.029) and inferior fronto-occipital fasciculus-right (p=0.048) and lower AD in the cingulum-right (p=0.027) than controls. Among all participants, greater levels of fatigue were associated with higher FA in the ACR-left (p=0.011), SS-left (p=0.003), SS-right (p=0.013), and SLF-right (p=0.005) (Figure 3A-D).
DISCUSSION
On postmortem studies, SARS-CoV-2 and its viral proteins were found in brain tissues, together with robust microglia and astrocyte activation and T cell infiltration, indicating immune activation and neuroinflammation in the brain.10,11 Opposite to our initial hypotheses, the white matter diffusivity was lower in participants with PASC than in controls. The restricted white matter diffusivity in our study might be explained by the repair processes in response to the initial neuroinflammation-induced brain injury, along with glia proliferation and activation, and immune cells infiltration.12 Consistent with our findings, prior studies of participants with post-COVID neurological symptoms (e.g., mood changes, fatigue, headache, vision changes, myalgia, memory loss, etc.) had lower diffusivities (AD and RD)4 and higher FA than controls 4,5 at 2-3 months post-COVID. However, participants without neurological symptoms during the acute phase had lower FA and higher diffusivities than controls at 2-3 months post-COVID.6,7 Higher FA predicted greater fatigue in our study, which has not been reported previously. However, others have reported that higher FA correlated with poorer cognitive flexibility5, more anxiety and depressive symptoms7 and higher level of plasma inflammatory maker IL-6 in post-COVID participants.6 Taken together, our study suggests that post-COVID neuropsychiatric symptoms may be related to persistent immune activation, which can be detected as persistent microstructural abnormalities. Future studies that correlate these findings with immune markers are needed.CONCLUSION
Participants with PASC might have persistent immune activation that leads to restricted diffusion in various white matter tracts in the brain. Longitudinal studies are needed to understand how WM diffusivity changes during recovery in those with PASC.Acknowledgements
This work was supported by NIH grants R21NS121615. We also thank our research participants for their participation.
References
REFERENCES:
1. Taquet M, Geddes JR, Husain M, Luciano S, Harrison PJ. 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: a retrospective cohort study using electronic health records. Lancet Psychiatry. 2021;8(5):416-427.
2. Graham EL, Clark JR, Orban ZS, et al. Persistent neurologic symptoms and cognitive dysfunction in non-hospitalized Covid-19 "long haulers". Ann Clin Transl Neurol. 2021;8(5):1073-1085.
3. Whitmore HAB, Kim LA. Understanding the Role of Blood Vessels in the Neurologic Manifestations of Coronavirus Disease 2019 (COVID-19). Am J Pathol. 2021;191(11):1946-1954.
4. Lu Y, Li X, Geng D, et al. Cerebral Micro-Structural Changes in COVID-19 Patients – An MRI-based 3-month Follow-up Study. EClinicalMedicine. 2020;25:100484.
5. Silva LS, Joao RB, Nogueira MH, et al. Functional and microstructural brain abnormalities, fatigue, and cognitive dysfunction after mild COVID-19. medRxiv. 2021.
6. Qin Y, Wu J, Chen T, et al. Long-term microstructure and cerebral blood flow changes in patients recovered from COVID-19 without neurological manifestations. J Clin Invest. 2021;131(8).
7. Yang L, Zhou M, Li L, et al. Characteristics of mental health implications and plasma metabolomics in patients recently recovered from COVID-19. Translational Psychiatry. 2021;11(1):307.
8. Li Y, Shea SM, Lorenz CH, Jiang H, Chou MC, Mori S. Image corruption detection in diffusion tensor imaging for post-processing and real-time monitoring. PLoS One. 2013;8(10):e49764.
9. Mori S, Wu D, Ceritoglu C, et al. MRICloud: Delivering High-Throughput MRI Neuroinformatics as Cloud-Based Software as a Service. Computing in Science & Engineering. 2016;18(5):21-35.
10. Matschke J, Lütgehetmann M, Hagel C, et al. Neuropathology of patients with COVID-19 in Germany: a post-mortem case series. Lancet Neurol. 2020;19(11):919-929.
11. Pröbstel AK, Schirmer L. SARS-CoV-2-specific neuropathology: fact or fiction? Trends Neurosci. 2021.
12. Boretius S, Escher A, Dallenga T, et al. Assessment of lesion pathology in a new animal model of MS by multiparametric MRI and DTI. Neuroimage. 2012;59(3):2678-2688.
Figures