4956
COVID-19 as an Opportunity for Quality Improvement in MR Neuro Imaging.
Emanuele Camerucci1, Jose Thulasee1, Matthew Bernstein1, Steven Messina1, Peter Kollasch1, and John Huston1
1Mayo Clinic, Rochester, MN, United States
1Mayo Clinic, Rochester, MN, United States
Synopsis
We took advantage of the COVID-19-related decrease in clinical volume to conduct a quality improvement project; we established a panel of 24 experts for reviewing currently used brain MRI sequences and proposing ways to improve image quality and/or decrease acquisition time. The proposed sequences were integrated in existing protocols and compared with the standard ones. We were able to improve 14 of the most used brain MRI sequences with an equal or improved image quality and reduced acquisition time. Hence, we were able to reduce the acquisition time of our Brain protocol and Epilepsy protocol by 29.2% and 40%, respectively.
Introduction
An unexpected beneficial consequence of the COVID-19 pandemic was the opportunity to perform a quality improvement (QI) project taking advantage of the unprecedented availability of both MRI scanner capacity and radiologist time.Methods
Subspecialty expert panel: We established a subspecialty panel of 15 board-certified radiologists, 6 registered technologists, 1 vendor scientist, and 2 board-certified medical physicists. A rapid and highly iterative process was designed and established. The panel held regular weekly meetings from April 2020 to July 2020.Sequence optimization process: The panel selected candidate MRI sequences to improve image quality and/or decrease acquisition times using 3T MAGNETOM Prisma (Siemens Healthcare, Erlangen, Germany). These sequences were subsequently introduced into the existing protocol containing the standard sequence and performed on a set of patients, typically 30. To provide an estimate of the effectiveness of the optimized sequences within clinical practice, we evaluated and compared the overall performance of the existing sequences to the candidate sequences based on signal to noise radio (SNR), artifacts, gray/white matter contrast, image sharpness/resolution and overall image quality of the sequences.
Evaluation: The corresponding cases were then graded with a 5-point Likert scale, with 1 indicating that the standard sequence was strongly preferred, 3 representing no differences between the two sequences, and 5 that the candidate sequence was preferred to the standard sequence. The final grade assigned to every set of images represented the consensus among the expertise of all the readers involved.
Statistical analysis: Statistical analysis was performed using both a one-sided and two-sided Wilcoxon signed rank tests. The null hypothesis of the left-sided test was that the candidate sequence performed equally to or better than the standard sequence; the right-sided test used the reverse of this hypothesis; whereas the two-sided null hypothesis was that the two sequences were equal.
Results
The panel met for a total of 14 virtual sessions. 20 MRI sequences underwent expert review process and ultimately, 14 MRI sequences met the final criteria for adequate quality to replace existing default sequences in clinical practice. Figure 1 reports the results of the statistical test for two sequences used as example to highlight our methodology, axial T2 TSE (accepted) and 2D sagittal T2 FLAIR (rejected). In these examples, we decided to accept the new axial T2 TSE for three main reasons. First, it came with a reduction in gradient-on acquisition time (1:45 vs the previous 2:17, with 32 seconds saved); second, it had no left-sided significances (Figure 1), indicating that the proposed sequence was never inferior to the standard in any of the five parameters assessed; third, it was deemed significantly better in number of motion artifacts and, most importantly, in terms of overall quality. On the other hand, even though the new 2D sagittal T1 FLAIR sequence led to a reduction in gradient-on acquisition time of 32 seconds (as many as in the T2E FS just reported), it was rejected for two reasons. First, it showed mixed right and left-sided significances (Figure 1), indicating that no sequence was clearly better than the other; second, all the measurements were deemed equivalent in three parameters, including overall quality. Hence, we improved the gradient-on acquisition time of the Brain protocol from 24:51 minutes to 17:35 (reduction of 29.3%) and the Epilepsy protocol from 32:21 to 19:24 minutes (reduction of 40%) while maintaining or improving image quality for each of the sequences. The original and the newer Brain protocol with and without gadolinium is described in detail in Figure 2. Epilepsy protocol before and after our QI is described in detail in Figure 3.Discussion
This work demonstrates the potential to produce important benefits to existing MRI sequences and radiology clinical workflows. With a focus on improved image quality and reduced scan times, it provides clinical practices with the flexibility to utilize the time savings to improve patient care in several ways. The new Brain protocol showed a reduction in gradient-on acquisition time of nearly 30% and the Epilepsy protocol gradient-on acquisition time was reduced by 40%. This allows the practice to manage a higher patient volume, devote additional time to educate patients prior to the exam, increase access to imaging by decreasing waiting lists and potentially even address staff burnout by reducing workplace stressors. Additionally, the practice has increased bandwidth to accommodate emergency add-on patients without disrupting an already overstretched work schedule. The time saved with improved sequence acquisition techniques is making a positive difference in today’s challenging healthcare environment.Conclusion
Strategic efforts to optimize neuro MR imaging during COVID-19 pandemic resulted in a practice improvement initiative that enhanced image quality, clinical workflow, and patient care in an existing clinical practice. We were able to improve 14 of the most commonly used brain MRI sequences with an equal or improved image quality and reduced acquisition time. Subsequently, we were able to reduce the acquisition time of our Brain protocol and Epilepsy protocol by 29.2% and 40% respectively.Acknowledgements
No acknowledgement found.References
No reference found.Figures
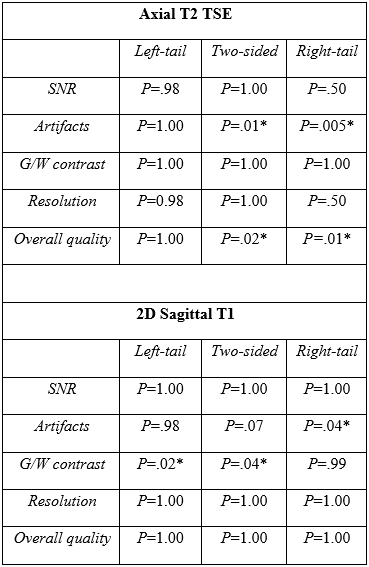
Results
of the statistical test for one accepted sequence (axial T2 TSE) and one
rejected sequence (2D sagittal T1).

Performance of Brain (with and without
gadolinium contrast) Protocol with Existing and Alternative Sequence.
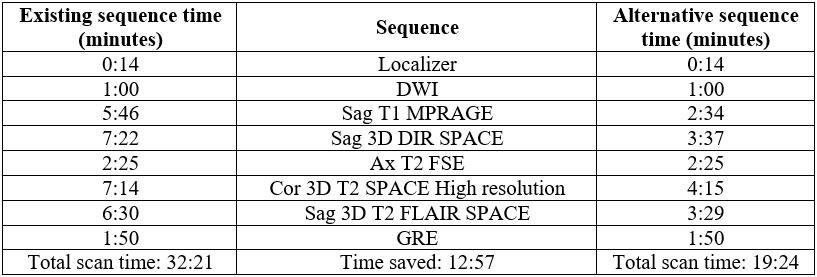
Performance of Epilepsy Protocol with Existing and Alternative Sequence.
DOI: https://doi.org/10.58530/2022/4956