4933
A randomized controlled trial of statins to reduce inflammation in cerebral aneurysms using vessel wall MRI1Radiology, University of Washington, Seattle, WA, United States, 2Neurosurgery, Tiantan Hospital, Beijing, China, 3Neurology, Tiantan Hospital, Beijing, China, 4Neurosurgery, University of Washington, Seattle, WA, United States, 5Neurosurgery, University of Iowa, Iowa, IA, United States
Synopsis
Aneurysm wall enhancement as shown on contrast-enhanced vessel wall MRI (VW-MRI) is a surrogate biomarker of intracranial aneurysm (IA) wall inflammation, and it is associated with IA symptoms, growth, and rupture. However, it hasn't been used in clinical trails for UIA treatment. We performed the first prospective randomized controlled trial on the effect of statins for changes in aneurysm wall enhancement as shown in VW-MRI. We found that statins decreased aneurysm wall enhancement of UIAs in a short term of 6 months. Our results suggest VWI-MRI has great potential in future image-guided clinical trails to investigate novel treatment of IAs.
Background
Intracranial aneurysm (IA) is a common disease with a prevalence of 3-5% in the general population. There are almost 500,000 deaths worldwide each year caused by rupture of intracranial with half the victims younger than age 50. Inflammation and atherosclerotic changes play a critical role in the formation and rupture of IAs. Statins may reduce aneurysmal inflammation, but several clinical studies did not reach a consistent conclusion.[1-3] A possible explanation for these divergent findings is the use of aneurysm diameter growth as an outcome may not be sensitive enough to detect short-term aneurysm changes. Aneurysm wall enhancement as shown on contrast-enhanced vessel wall magnetic resonance imaging (VW-MRI) is a surrogate and sensitive biomarker of aneurysm wall inflammation, and it is associated with UIA symptoms, growth, and rupture.[4-9] Our study aimed to evaluate if statins could decrease UIA wall enhancement, suggesting modulation of inflammation and potential prevention of rupture, and also to monitor the effect of statins on aneurysm morphology and inflammation-related circulating biomarkers.Methods
In this double-blind, randomized, placebo-controlled trial (registered with ClinicalTrials.gov, NCT04149483), 60 patients with UIAs were enrolled between Nov 07, 2019, and Jun 30, 2021. They were randomized 1:1 to either atorvastatin 20mg daily or placebo. Subjects were imaged at baseline and at 6-month follow up with VW-MRI. MR imaging was performed using a 3.0T MR system (Prisma, Siemens Healthineers; Erlangen, Germany) with a 32-channel head coil. 3D T1-weighted tubro-spin-echo with variable flip angle (SPACE) was acquired in sagittal plane with whole head coverage and 0.7 mm isotropic resolution before and immediately after intravenous gadolinium contrast injection: TR/TE: 800/22ms, echo train length 52, scan time 5:30s. The primary endpoint was change in aneurysm wall enhancement measured by the quantitative wall enhancement index (WEI [6])WEI=(SIWallPre/SIWhitematterPre –SIWallPost/SIWhitematterPost) / ( SIWallPre/SIWhitematterPre)
and three dimensional wall enhancement volume rate (WEVR):
WEVR = Aneurysm Enhancement Volume/Whole Aneurysm Volume ×100%.
The secondary outcomes were changes in aneurysm size and/or morphology and inflammation-related circulating biomarkers. Additional method details can be found at ClinicalTrials.gov.
Results
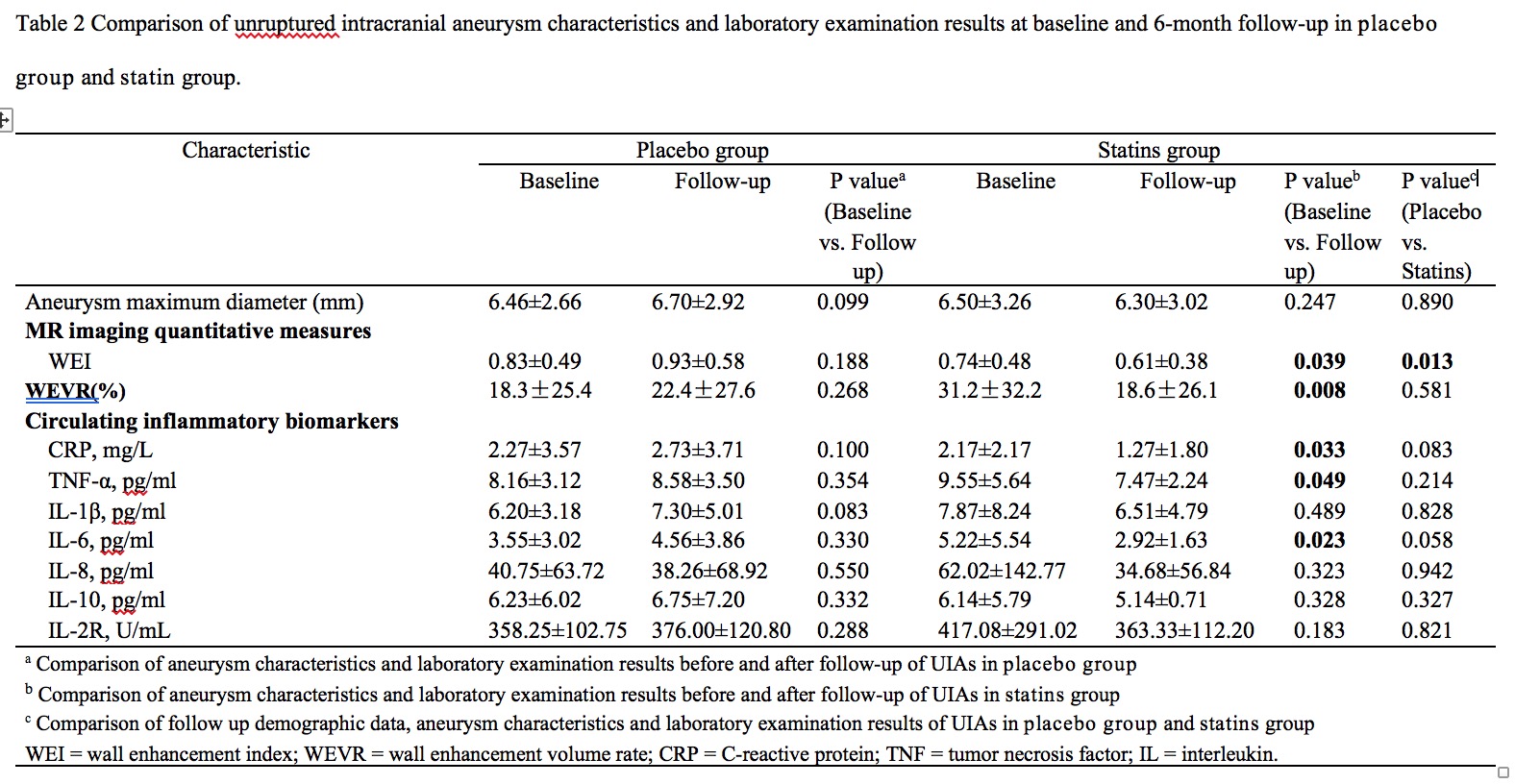
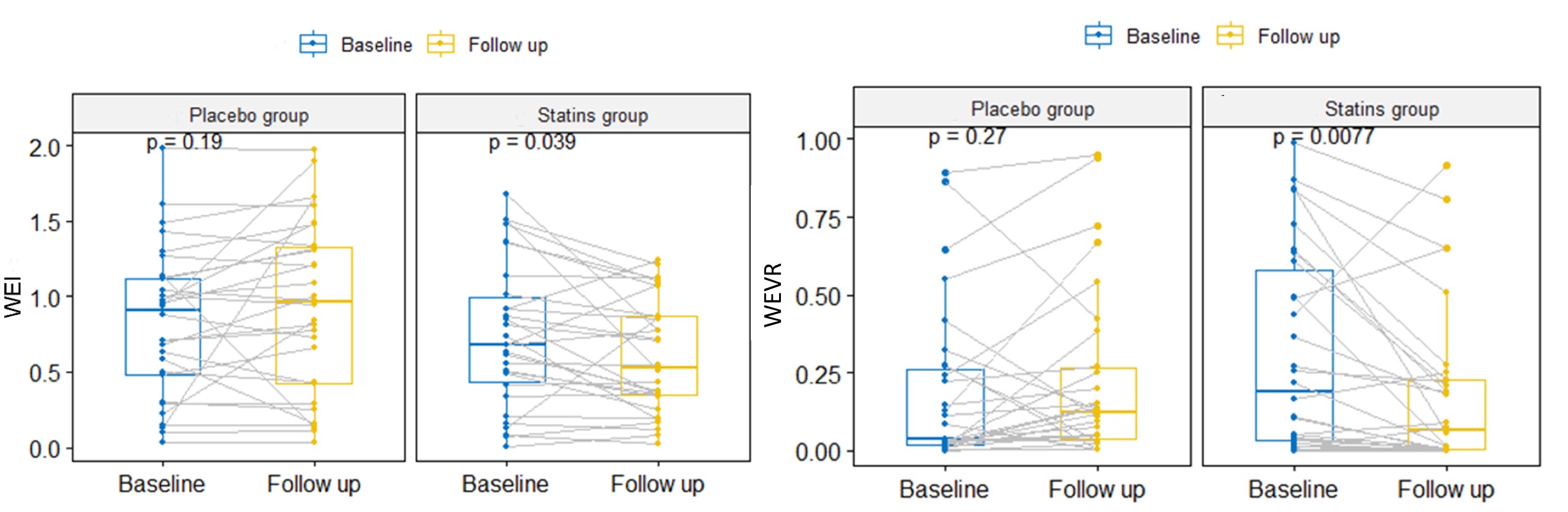
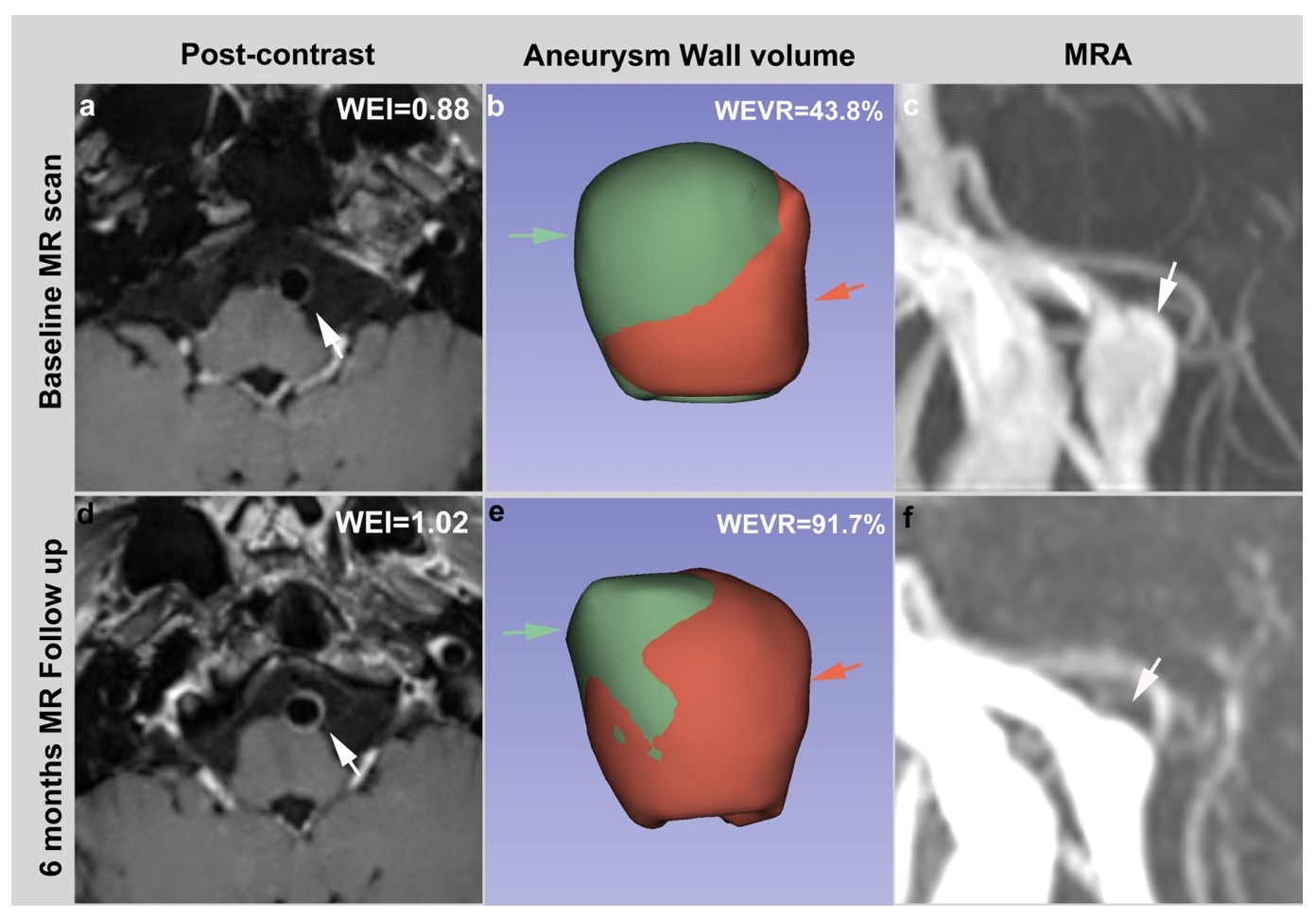
Results: The patients’ demographic information is shown in Table 1. In the atorvastatin group, the WEI and WEVR decreased significantly at 6-month follow-up compared to baseline (P=0.039 and P=0.008, respectively, Table 2 and Figure 1), but not in the placebo group (P=0.188 and P=0.268 respectively). Furthermore, circulating plasma levels of C-reactive protein, tumor necrosis factor-α and interleukin-6 in the atorvastatin group deceased significantly at 6 months compared to baseline (p= 0.033, 0.049 and 0.023, respectively). Aneurysm size did not change significantly in either group. Patient cases are shown in Figure 2 and 3.Discussion/Conclusion
In this randomized, double-blinded, placebo-controlled trial, we found that statins decreased aneurysm wall enhancement of UIAs, which serve as a surrogate markers for aneurysm wall inflammation. The quantitative WEI and WEVR as well as several circulating inflammatory biomarkers (C-reactive protein, TNF-α, and IL-6) decreased significantly after 6-month atorvastatin treatment. However, aneurysm size did not change in either group. To the best of our knowledge, this is the first prospective randomized controlled trial on the effect of statins for changes in aneurysm wall enhancement as shown in VWI-MRI. Our study showed significant changes in arterial wall enhancement characteristics (WEI and WEVR) that coincided with circulating inflammatory biomarker reductions over a 6-month period in association with statin therapy, while aneurysm morphologic characteristics, including aneurysm size and shape did not change. The use of quantitative and three-dimensional enhancement characters was also a unique advantage of our study. A few cross-sectional studies have found conflicting results for whether statins were protective against IA formation or rupture.[1, 3, 10] Possible reasons are: 1) they were not randomlized or 2) the statin dose was low (10mg/day) or 3) they were retrospective in design. In addition, all previous studies used growth or rupture as the only endpoints, resulting in low event rate because UIA had very low growth and rupture rates. By using VWI-MRI, we are able to observe the inflammatory changes of the aneurysmal wall within a short period of 6 months. VWI-MRI has great potential in future image-guided clinical trails to investigate novel treatment of IAs. In conclusion, Atorvastatin significantly decreased UIA wall enhancement in this randomized controlled trial relative to the placebo control group.Acknowledgements
Dr Zhu receives grant support from the National Institutes of Health (R00HL136883).References
[1]. Bekelis K, Smith J, Zhou W, et al. Statins and subarachnoid hemorrhage in Medicare patients with unruptured cerebral aneurysms. Int J Stroke. 2015 10 Suppl A100: 38-45.
[2]. Yoshida K, Uwano I, Sasaki M, et al. Small Unruptured Aneurysm Verification-prevention Effect against Growth of Cerebral Aneurysm Study Using Statin. Neurol Med Chir (Tokyo). 2021 61: 442-451.[3]. Marbacher S, Schläppi J-A, Fung C, Hüsler J, Beck J, Raabe A. Do statins reduce the risk of aneurysm development: a case-control study. Journal of Neurosurgery. 2012 116: 638-642.
[4]. Quan K, Song J, Yang Z, et al. Validation of Wall Enhancement as a New Imaging Biomarker of Unruptured Cerebral Aneurysm. Stroke. 2019 50: 1570-1573.
[5]. Zhong W, Su W, Li T, et al. Aneurysm Wall Enhancement in Unruptured Intracranial Aneurysms: A Histopathological Evaluation. Journal of the American Heart Association. 2021 10: e018633.
[6]. Fu Q, Wang Y, Zhang Y, et al. Qualitative and Quantitative Wall Enhancement on Magnetic Resonance Imaging Is Associated With Symptoms of Unruptured Intracranial Aneurysms. Stroke. 2021 52: 213-222.
[7]. Gariel F, Ben Hassen W, Boulouis G, et al. Increased Wall Enhancement During Follow-Up as a Predictor of Subsequent Aneurysmal Growth. Stroke. 2020 51: 1868-1872.
[8]. Wang X, Zhu C, Leng Y, Degnan AJ, Lu J. Intracranial Aneurysm Wall Enhancement Associated with Aneurysm Rupture: A Systematic Review and Meta-analysis. Academic radiology. 2019 26: 664-673.[9]. Edjlali M, Guedon A, Ben Hassen W, et al. Circumferential Thick Enhancement at Vessel Wall MRI Has High Specificity for Intracranial Aneurysm Instability. Radiology. 2018 289: 181-187.
[10]. Yoshimura Y, Murakami Y, Saitoh M, et al. Statin use and risk of cerebral aneurysm rupture: a hospital-based case–control study in Japan. Journal of Stroke and Cerebrovascular Diseases. 2014 23: 343-348.
Figures