4914
Manifold-based Respiratory Phase Estimation Enables Motion and Distortion Correction of Free-Breathing Cardiac Diffusion Tensor MRI1Cardiology, Massachusetts General Hospital, Charlestown, MA, United States, 2Harvard Medical School, Boston, MA, United States, 3Athinoula A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Charlestown, MA, United States, 4Massachusetts Insitute of Technology, Cambridge, MA, United States
Synopsis
For in-vivo cardiac diffusion-tensor MRI (DT-MRI), respiratory motion and B0 field inhomogeneities produce misalignment and geometric distortion in diffusion weighted images acquired with conventional single shot echo planar imaging. We propose using Laplacian Eigenmaps (LE), a dimensionality reduction method, to retrospectively estimate the respiratory phase of DWI and facilitate both distortion correction (DisCo) and motion compensation (MoCo). LE-based DisCo and MoCo reduces geometric distortion by 13.2% while producing computationally efficient image alignment. Furthermore, preliminary results indicate the LE-based DisCo and MoCo can be applied with only acquiring a single set of b-value averages.
Introduction
Free-breathing cardiac DT-MRI is a promising imaging technique to evaluate the microstructure of the heart1,2. Recently, 2nd order motion compensated (M2) diffusion gradient encoding and two-dimensional spatial selective radiofrequency (2DRF) zoomed EPI enabled single-shot and single-heartbeat acquisition with improved SNR and spatial resolution3,4. However, B0 field inhomogeneities in the torso introduce geometric distortion to the images acquired with EPI readout. Moreover, breathing impedes using standard distortion correction (DisCo) techniques such as TOPUP5 due to respiratory dependent B0 field inhomogeneities and within and through-plane displacement of the tissue. To provide DT-MRI model estimates that are aligned with complementary contrasts such as T1 or T2, it is necessary to first perform DisCo and motion compensation (MoCo) to the raw diffusion weighted images (DWI). Here, we propose an approach that uses the respiratory phase of the DWI to enable DisCo and that reduces the computational demands of MoCo, while reducing its sensitivity to contrast differences in DWI.Methods
Free-breathing ECG-triggered whole left-ventricular (LV) cardiac DTI using an M2 2D-RF zoomed spin echo EPI sequence was performed on eleven healthy volunteers (mean age 43 years, 5 female) under the appropriate approval of the Institutional Review Board of the Massachusetts General Hospital. The acquisition was performed on a 3T clinical MRI system (MAGNETOM Prisma, Siemens Healthineers, Erlangen, Germany), equipped with an 80mT/m gradient system and a standard 32-channel antero-posterior surface coil (2.5x2.5x8mm3, matrix size 150x44, pixel bandwidth 2380 Hz/pixel, 1/3 reduced FOV, FOV=375mm, Partial Fourier=6/8, TE=79ms, TR= number of slices x RR) at b=50 s/mm2 and 30 gradient directions x2 averages at b=500 s/mm2. The images were acquired with phase encoding along the anterior-posterior (AP) direction, adjusted to minimize aliasing artifacts, and then reversed 180° (PA) for a second acquisition with the same parameters. The scanning protocol also included a T2-HASTE under breath-hold to serve as a distortion-free reference (TE 36ms, TR=ECG trigger, (BW) 1860Hz/pixel, matrix size 128x96 and voxel size 1.125x1.125 mm2). Finally, a second group of four volunteers (mean age 39.5, 3 female) was recruited and imaged with the same DWI sequence, now including a pencil navigator echo to track respiratory phase for validation.Distortion and Motion compensation (DisCo and MoCo) were performed after estimating the respiratory phase of each DWI6. All the images were projected into a 2D space using Laplacian Eigenmaps, where they formed an elongated cluster per b-value. Respiratory phase was then estimated by extracting the relative position along the elongated direction of the clusters. Afterwards, the b=50 s/mm2 images with opposite phase encoding were sorted according to respiration and used to estimate the B0 field distortion with TOPUP5. These fields were subsequently used to correct the distortion in all DWI also sorted by respiration. To perform MoCo, the images were binned into 5 groups according to their respiratory phase and the average centroid of each bin was registered to the centroid at the end-expiratory phase, hence ensuring similar position across slices. Each image was aligned following the transformation learned with the registration transforms learned with the corresponding centroid. The results were compared against conventional breath-held HASTE by computing the distances between the LV contours manually segmented using the DTI data and the HASTE images. Cardiac DTI parameters including fractional anisotropy (FA), mean diffusivity (MD) and helix angle transmurality (HAT) were compared with and without DisCo.
Results
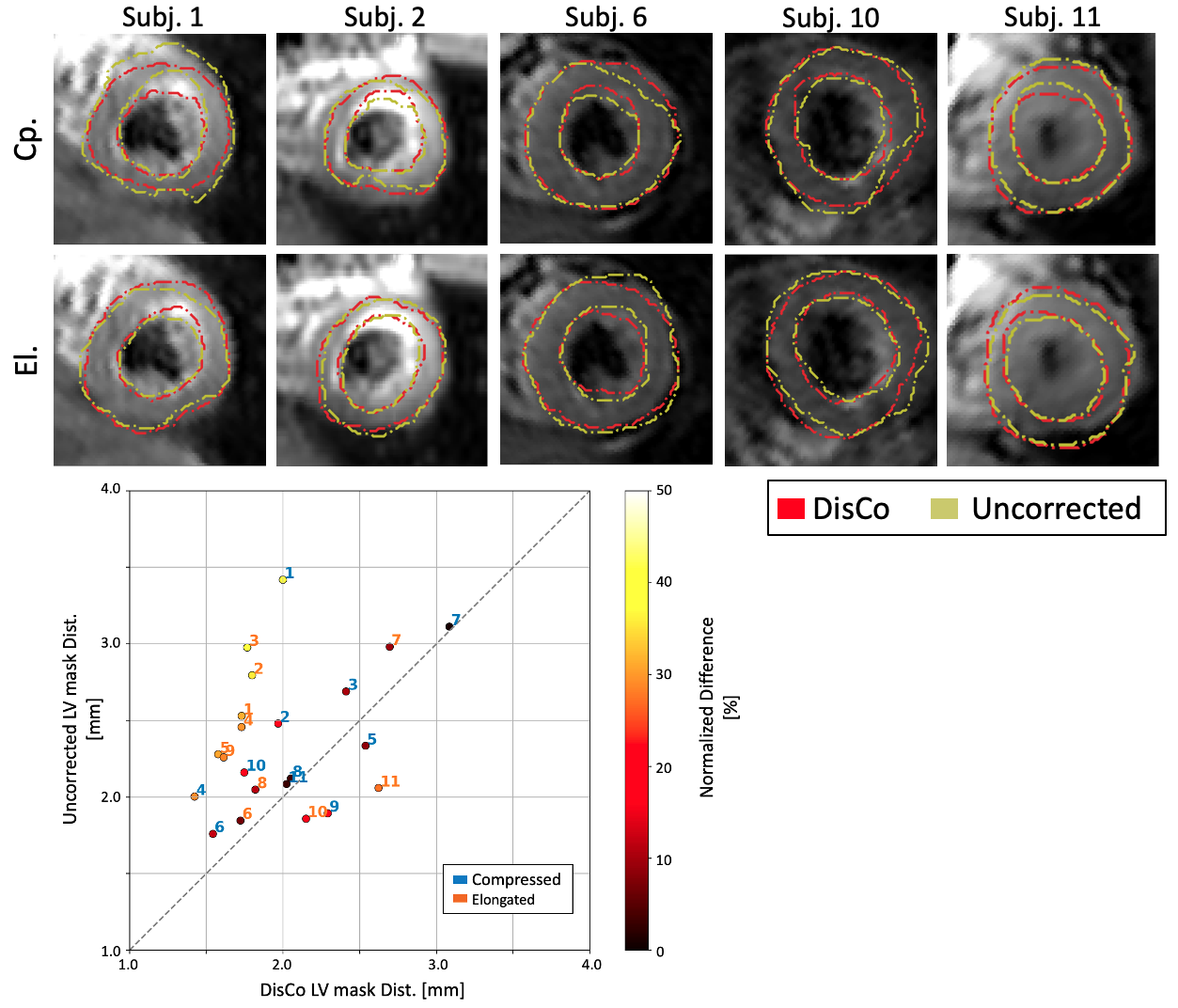
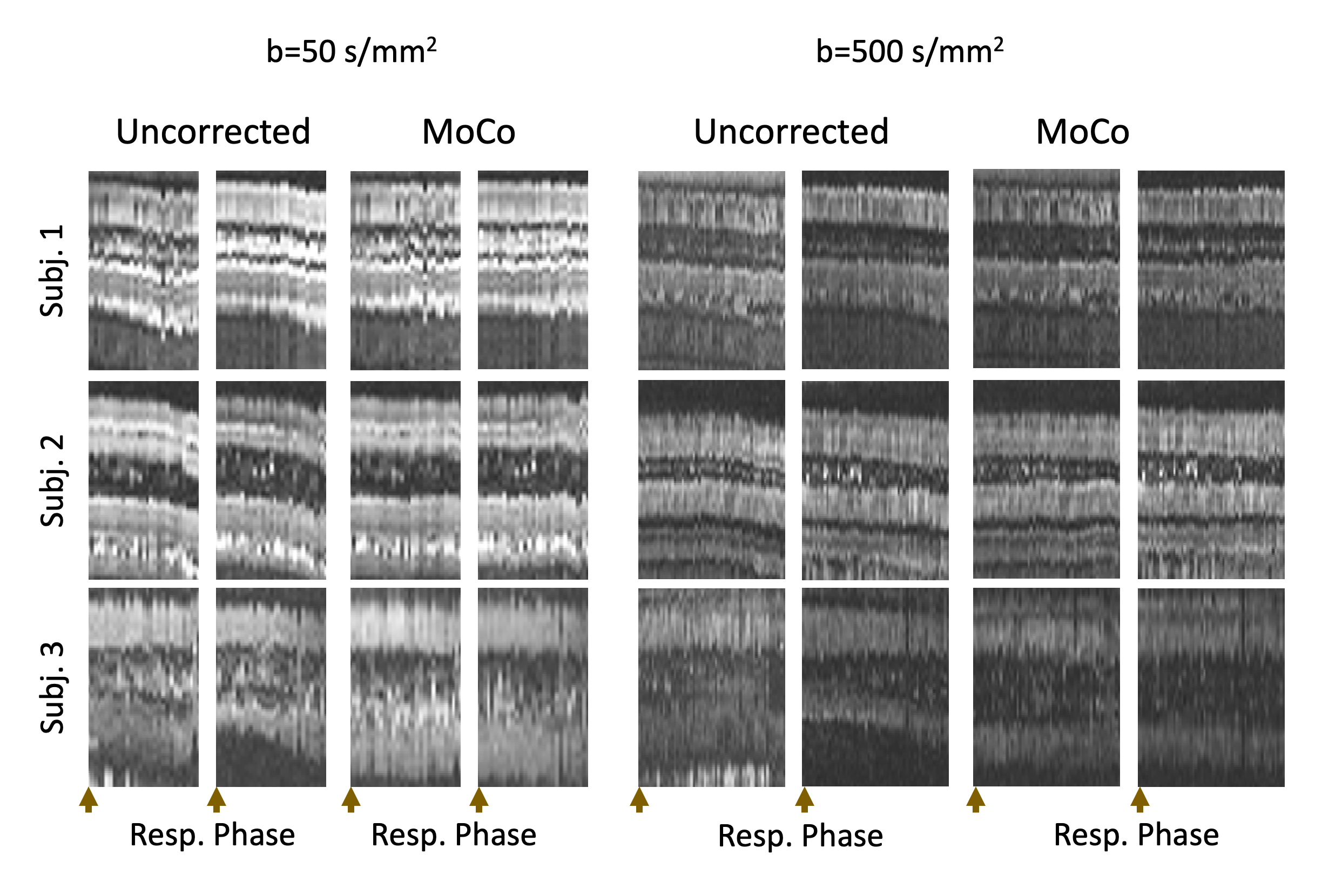
Figure 1 shows the 2D projection obtained with LE, the estimated respiratory phases and the DWI sorted according to respiration. As expected, the LE projection resulted in two clusters (b50 and b500) with the elongated axis matching the respiratory phase estimated with the navigator echoes. Consequently, the respiratory phases estimated with the proposed method and the navigator echoes presented good agreement over time (correlation of 0.72+/-0.14) and resulted in similar transitions between end-expiration and end-inspiration after sorting all DWI. The LV contours of the DisCo images presented improved alignment with the HASTE reference over the uncorrected images (Figure 2). Numerically, this reduced the average distance between the LV contours generated with DWI and HASTE data by 13.2+/-19.2% p<0.05 (2.0+/-0.4 for DisCo and 2.4+/-0.5 mm for uncorrected). Figure 3 shows a line of voxels plotted over respiratory phase before and after MoCo for representative subjects. The respiratory binned approach resulted in DWI aligned throughout the entire respiratory cycle even though the registration was estimated only with the centroids, hence considerably reducing the computational demands. Finally, DisCo DTI parameter maps, shown in Figure 4, yielded no significant differences beyond the changes in geometry due to DisCo (MD: 1.55+/-0.13 x10-3mm2/s and 1.53+/-0.13 x10-3mm2/s, p=0.09; FA: 0.375+/-0.041 and 0.379+/-0.045, p=0.11; HAT: 1.00+/-0.10 °/% and 0.99+/-0.12 °/%, p=0.44). These results were generated with a full DTI acquisition with opposite phase encoding; however, preliminary results generated by only acquiring an extra set of b50 images for DisCo can provide similar results (Figure 5).Conclusion
Retrospective respiratory phase estimation with LE-based DisCo and MoCo in free-breathing cardiac DTI resulted in significantly reduced geometric distortion and improved alignment within and across slices. The LV contour distortion was reduced an average of 13.2%, although the cardiac DTI parameters did not result in significant differences between when DisCo was applied.Acknowledgements
This work was partially funded by the National Institutes of Health awards R01HL151704, R01HL159010, R01HL135242 and R01HL131635.References
1. Nguyen CT, Fan Z, Xie Y, et al.: In vivo diffusion-tensor MRI of the human heart on a 3 tesla clinical scanner: An optimized second order (M2) motion compensated diffusion-preparation approach. Magn Reson Med 2016; 76:1354–1363.
2. Nielles-Vallespin S, Khalique Z, Ferreira PF, et al.: Assessment of Myocardial Microstructural Dynamics by In Vivo Diffusion Tensor Cardiac Magnetic Resonance. J Am Coll Cardiol 2017; 69:661–676.
3. Riffel P, Michaely HJ, Morelli JN, et al.: Zoomed EPI-DWI of the Pancreas Using Two-Dimensional Spatially-Selective Radiofrequency Excitation Pulses. PLoS One 2014; 9:e89468.
4. Nguyen CT, Christodoulou AG, Coll‐Font J, et al.: Free‐breathing diffusion tensor MRI of the whole left ventricle using second‐order motion compensation and multitasking respiratory motion correction. Magn Reson Med 2021; 85:2634–2648.
5. Jaume Coll-Font, Chen S, Eder RA, et al.: Manifold-based respiratory phase estimation enables motion and distortion correction of free-breathing cardiac diffusion tensor MRI. Magn Reson Med 2021(July):1–14.
6. Andersson JLR, Skare S, Ashburner J: How to correct susceptibility distortions in spin-echo echo-planar images: Application to diffusion tensor imaging. Neuroimage 2003; 20:870–888.
Figures