4889
Imaging Ascending Thoracic Aortic Aneurysm Wall Stretch: A Comparison to Biaxial Mechanical Testing1Department of Radiology and Biomedical Imaging, University of California, San Francisco, San Francisco, CA, United States, 2Department of Radiology, University of Washington, Seattle, WA, United States, 3Department of Surgery, University of California, San Francisco, San Francisco, CA, United States, 4Department of Biomedical Engineering, University of Virginia, Charlottesville, VA, United States
Synopsis
Ascending thoracic aortic aneurysm (aTAA) can result in life-threatening rupture or dissection. Displacement encoding with stimulated echoes (DENSE) is a non-invasive phase-contrast MRI technique that can measure aTAA wall deformation during the cardiac cycle. This study investigated DENSE-derived aTAA wall stretch in patients and found that the ratio between aTAA stretch and descending aorta stretch was different in patients who met surgical repair criteria from those who did not. Moreover, mechanical properties of aTAA specimens from patients who underwent surgery correlated significantly with in vivo DENSE measurements. Our findings suggest DENSE as a potential imaging marker for understanding aTAA progression.
1. Introduction
Rupture and dissection are life-threatening sequelae of ascending thoracic aortic aneurysms (aTAAs). Current management guidelines recommend surgical intervention when aTAA size meets the repair threshold (e.g., 5.5cm for patients without valvular disease) [1]. Aneurysm development is associated with degradative extracellular matrix (ECM) remodeling which reduces the aneurysm wall integrity [2-5]. Aneurysm stiffness is associated with mural ECM composition, suggesting that it could be relevant for understanding the disease progression [6,7].Displacement encoding with stimulated echoes (DENSE) is a non-invasive phase-contrast MRI technique that measures tissue displacement during its deformation, from which local stretch or strain can be derived to gauge stiffness [8,9]. Although DENSE has been developed for assessing the relatively thick myocardium, feasibility has been recently demonstrated in application to the arterial wall [10-12]. However, no study to date has investigated DENSE-derived aneurysm wall stretch in different aTAA patient groups. Moreover, in vivo aortic DENSE has not been compared with mechanical testing on aTAA specimens.
The aim of this study is to investigate DENSE-measured aTAA wall stretch in bicuspid aortic valve (BAV) and tricuspid aortic valve (TAV) patients who met repair criteria and underwent surgical repair versus those undergoing surveillance. We also sought to compare the in vivo DENSE-derived aneurysm wall stretch to measurements from ex vivo biaxial mechanical testing on aTAA specimens from the same surgical patients.
2. Methods
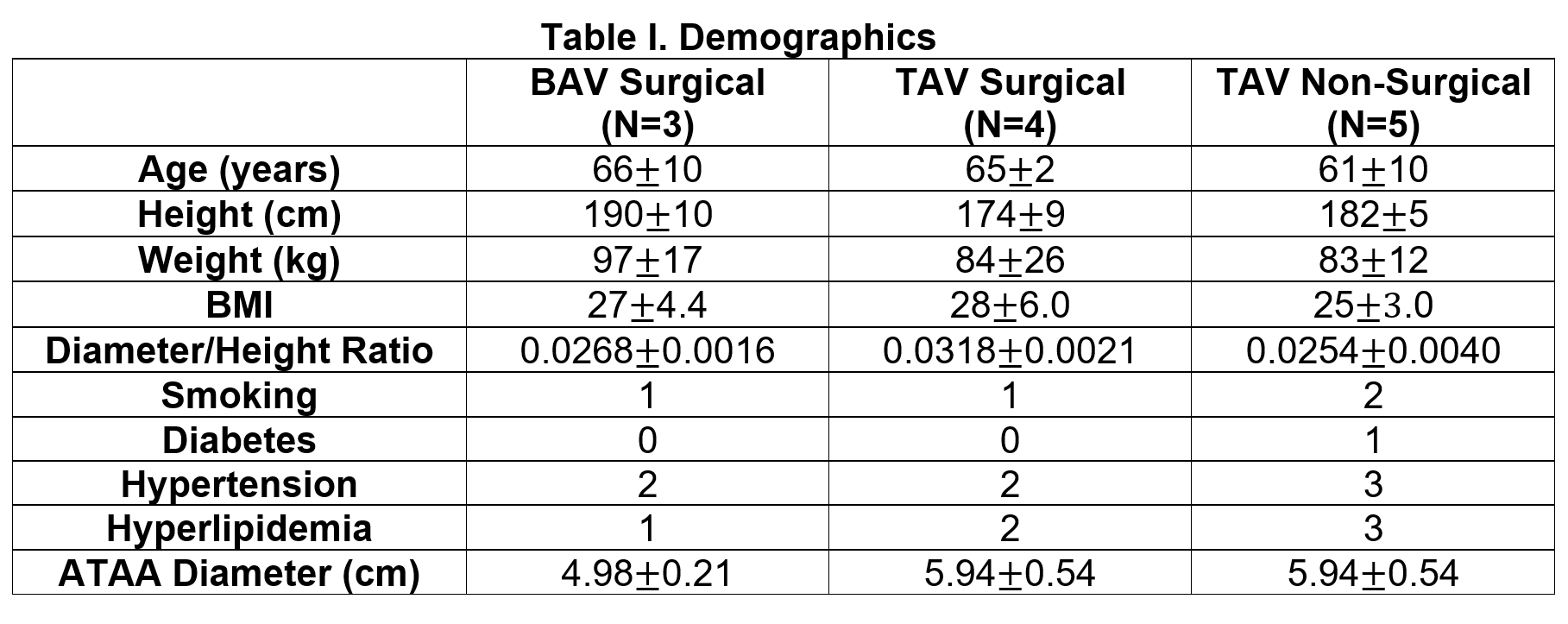
2.1 Study PopulationIn this prospective study, in vivo aortic DENSE was performed on 12 male aTAA patients. Three BAV patients and four TAV patients who met repair criteria underwent surgery while five TAV patients who did not the criteria were continued imaging surveillance (Table I). DENSE imaging was performed prior to the surgery. Among all surgical patients, aTAA specimens were collected from four patients for ex vivo mechanical testing.
2.2 Image Acquisition
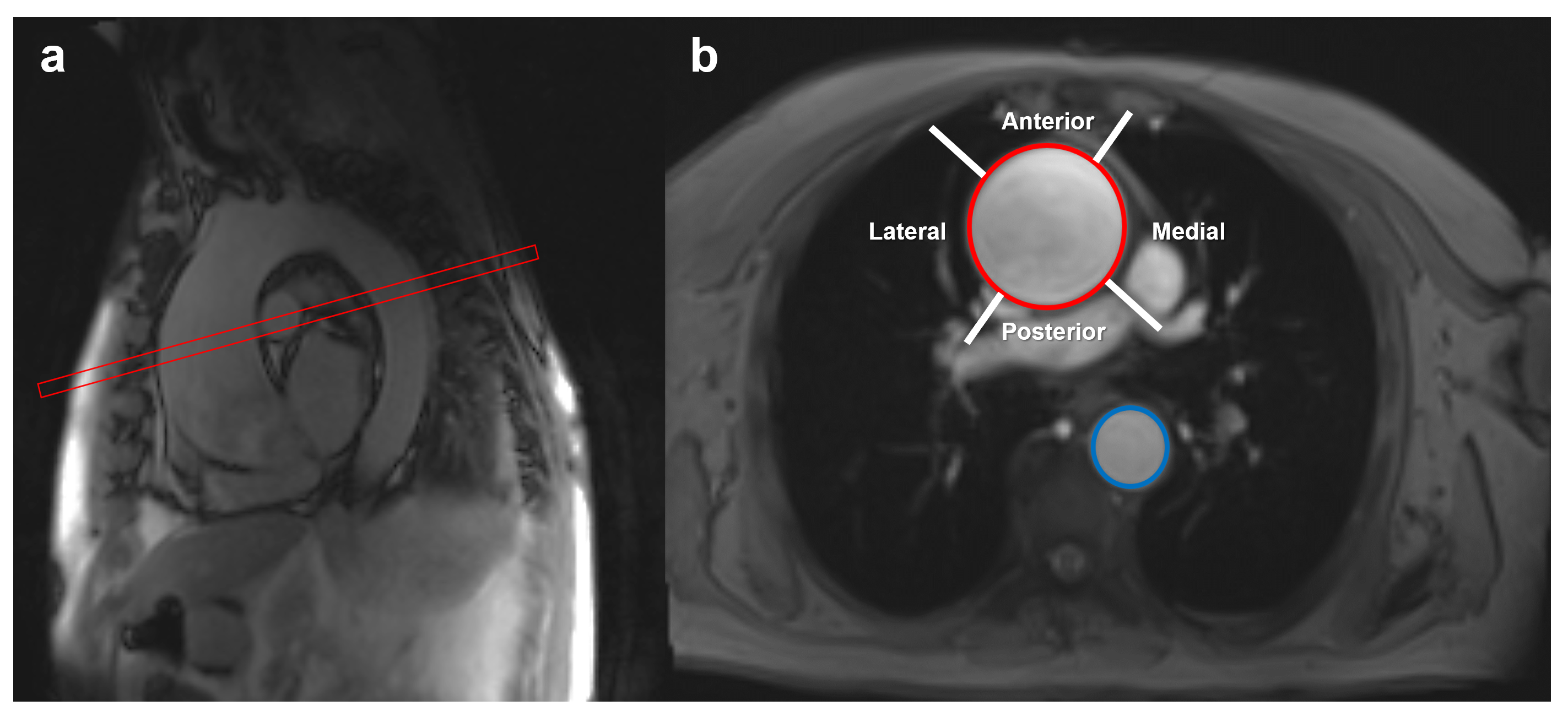
Data were acquired on 1.5T or 3T scanners (Avanto or Skyra, Siemens Healthcare, Erlangen, Germany). A single imaging plane was prescribed orthogonal to the vessel centerline at the level of maximum aTAA diameter in the tubular portion of the ascending aorta (see Figure 1). CINE steady-state free precession (SSFP) imaging was performed first to determine the time point when the ascending aorta distended maximally. Subsequently, a cardiac and respiratory navigator-gated DENSE acquisition [9] was performed through the same slice. Imaging parameters were TE=1.14 ms, TR=18–27 ms, 8-10 spiral interleaves per image, 1 spiral interleave per heartbeat, FOV=320×320 to 410×410 mm2, slice thickness=8 mm and reconstruction matrix size=148×148 to 180×180. Additional DENSE parameters were: in-plane (xy-plane) and through-plane (z-direction) encoding frequencies of 0.08-0.37 cycles/mm, balanced four-point encoding and three-point phase cycling to suppress spurious free induction decays and artifact-generating echoes [13, 14].
2.3 Image Analysis
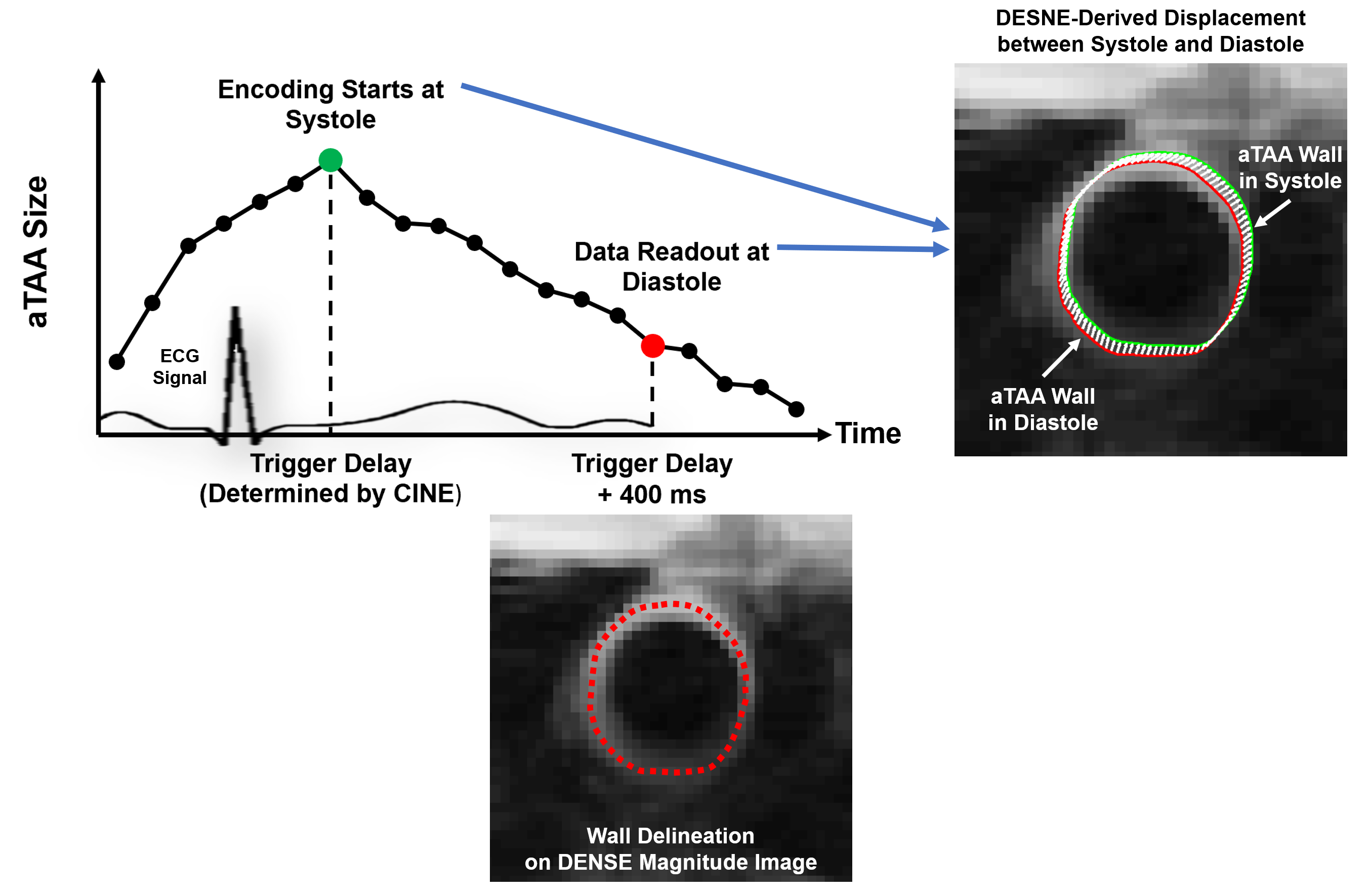
DENSE encoding was performed at the time of maximal aortic distension at systole, and the imaging readout was performed 400 ms later in diastole to quantify the wall stretch that occurred between diastole and systole (Figure 2). A purpose-built post-processor [12] was employed to derive the wall stretch for aTAA (λaTAA) and for the remote normal descending aorta (λDA) within the same slice. Additionally, we calculated the ratio of stretch in the aTAA relative to that in the descending aorta as: γ=λaTAA/λDA. The stretch ratio normalizes aTAA with the remote normal aorta for each individual and thus potentially reduces the effect of confounding factors such as age among different patients.
2.4 Biaxial Mechanical Testing
Ex vivo mechanical testing was performed on aTAA specimens harvested from four surgical patients. Specimens were subject to stretch testing using a custom-built planar biaxial stretching system [15, 16]. The specimen deformation at failure with respect to its original length was recorded as failure stretch. For each of the four patients, regional wall stretch was investigated by dividing the aTAA into four quadrants: anterior, posterior, medial and lateral (Figure 1b). DENSE-derived aTAA stretch and the mechanical testing-measured failure stretch were compared for each quadrant.
3. Results
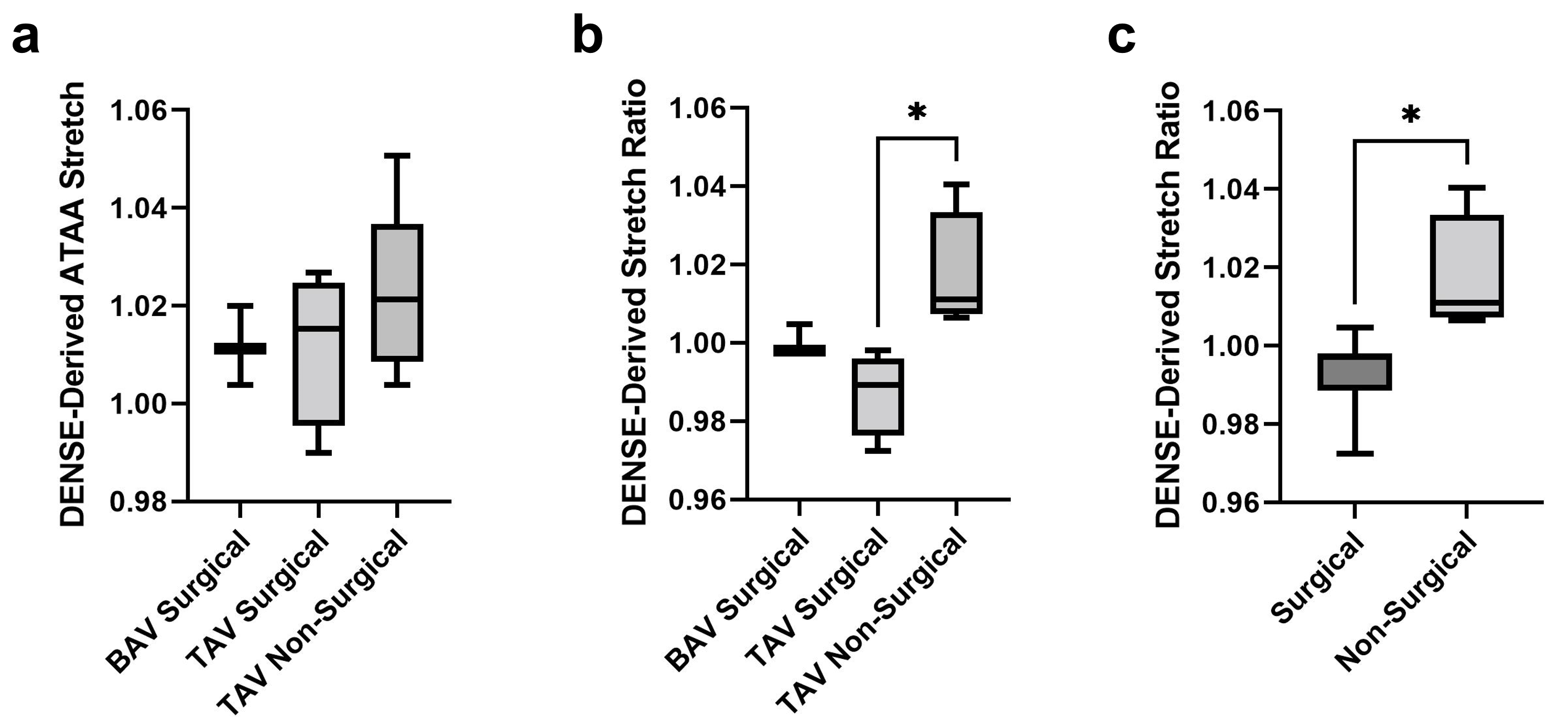
For BAV surgical patients, TAV surgical patients and TAV non-surgical patients, the mean DENSE-derived ATAA wall stretch between diastole and systole was 1.17±0.81%, 1.18±1.58% and 2.23±1.76%, respectively (Figure 3a).The mean DENSE-derived ratio of aTAA stretch to descending aorta stretch was 0.999±0.004, 0.987±0.013 and 1.017±0.017 for these three groups, respectively (Figure 3b). Moreover, DENSE-derived stretch ratio was significantly lower among TAV surgical patients than the non-surgical groups (p=0.02).
Pooling both BAV and TAV surgical patients, we also observed a significantly lower stretch ratio in the pooled surgical group when compared to the non-surgical patients (p=0.01) as shown in Figure 3c, suggesting less compliant aneurysms in the patients who proceeded to surgical intervention.
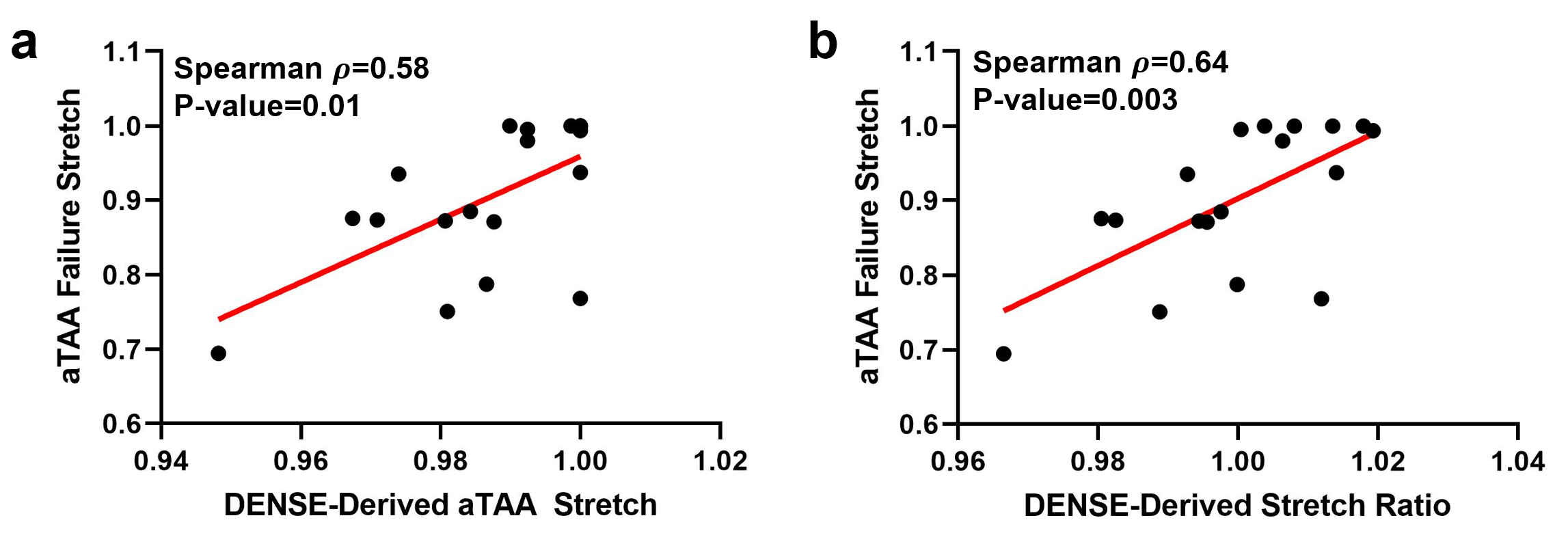
The failure stretch of aneurysm wall measured via mechanical testing correlated to both (1) DENSE-derived aTAA stretch (Spearman rho=0.58, p=0.01, Figure 4a) and (2) stretch ratio (Spearman rho=0.64, p=0.003, Figure 4b), demonstrating the potential of DENSE for risk stratification.
4.Conclusion
DENSE-derived aortic stretch ratio was lower for surgical aTAA patients compared to non-surgical patients. In vivo DENSE measurements correlated to mechanical testing-measured the failure property of the aneurysm wall. Future work is warranted to evaluate whether DENSE has utility as a novel imaging marker of aTAA progression.Acknowledgements
No acknowledgement found.References
1. Davies RR, Goldstein LJ, Coady MA, et al. Yearly rupture or dissection rates for thoracic aortic aneurysms: simple prediction based on size. Ann Thorac Surg. 2002;73(1):17-28. doi:10.1016/S0003-4975(01)03236-2
2. Hope MD, Meadows AK, Hope TA, et al. Clinical evaluation of aortic coarctation with 4D flow MR imaging. J Magn Reson Imaging. 2010;31(3):711-718. doi:10.1002/jmri.22083
3. Lindeman JHN, Ashcroft BA, Beenakker J-WM, et al. Distinct defects in collagen microarchitecture underlie vessel-wall failure in advanced abdominal aneurysms and aneurysms in Marfan syndrome. Proc Natl Acad Sci. 2010;107(2):862-865. doi:10.1073/pnas.0910312107
4. Vorp DA, Geest JP Vande. Biomechanical Determinants of Abdominal Aortic Aneurysm Rupture. Arterioscler Thromb Vasc Biol. 2005;25(8):1558-1566. doi:10.1161/01.ATV.0000174129.77391.55
5. Wisneski AD, Wang Z, Xuan Y, Ge L, Tseng EE. Biomechanics of Ascending Thoracic Aortic Aneurysm: Computational Modeling and Pursuit of Wall Stress Based Rupture Risk. J Am Coll Surg. 2019;229(4):S43-S44. doi:10.1016/j.jamcollsurg.2019.08.108
6. Iliopoulos DC, Kritharis EP, Giagini AT, Papadodima SA, Sokolis DP. Ascending thoracic aortic aneurysms are associated with compositional remodeling and vessel stiffening but not weakening in age-matched subjects. J Thorac Cardiovasc Surg. 2009;137(1):101-109. doi:10.1016/j.jtcvs.2008.07.023
7. Dong H, Russell DS, Litsky AS, et al. In Vivo Aortic Magnetic Resonance Elastography in Abdominal Aortic Aneurysm. Invest Radiol. 2020;Publish Ah(7):Publish Ahead of Print. doi:10.1097/RLI.0000000000000660
8. Aletras AH, Ding S, Balaban RS, Wen H. DENSE: Displacement Encoding with Stimulated Echoes in Cardiac Functional MRI. J Magn Reson. 1999;137(1):247-252. doi:10.1006/JMRE.1998.1676
9. Zhong X, Spottiswoode BS, Meyer CH, Kramer CM, Epstein FH. Imaging three-dimensional myocardial mechanics using navigator-gated volumetric spiral cine DENSE MRI. Magn Reson Med. 2010;64(4):1089-1097. doi:10.1002/MRM.22503
10. Iffrig E, Wilson JS, Zhong X, Oshinski JN. Demonstration of circumferential heterogeneity in displacement and strain in the abdominal aortic wall by spiral cine DENSE MRI. J Magn Reson Imaging. 2019;49(3):731-743. doi:10.1002/JMRI.26304
11. Wilson JS, Taylor WR, Oshinski J. Assessment of the regional distribution of normalized circumferential strain in the thoracic and abdominal aorta using DENSE cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2019;21(1):59. doi:10.1186/s12968-019-0565-0
12. Haraldsson H, Hope M, Acevedo-Bolton G, et al. Feasibility of asymmetric stretch assessment in the ascending aortic wall with DENSE cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2014 161. 2014;16(1):1-8. doi:10.1186/1532-429X-16-6
13. Kim D, Gilson WD, Kramer CM, Epstein FH. Myocardial Tissue Tracking with Two-dimensional Cine Displacement-encoded MR Imaging: Development and Initial Evaluation. Radiology. 2004;230(3):862-871. doi:10.1148/radiol.2303021213
14. Zhong X, Spottiswoode BS, Cowart EA, Gilson WD, Epstein FH. Selective suppression of artifact-generating echoes in cine DENSE using through-plane dephasing. Magn Reson Med. 2006;56(5):1126-1131. doi:10.1002/MRM.21058
15. Azadani AN, Chitsaz S, Matthews PB, et al. Biomechanical comparison of human pulmonary and aortic roots. Eur J Cardio-Thoracic Surg. 2012;41(5):1111-1116. doi:10.1093/EJCTS/EZR163
16. Azadani AN, Chitsaz S, Matthews PB, et al. Comparison of Mechanical Properties of Human Ascending Aorta and Aortic Sinuses. Ann Thorac Surg. 2012;93(1):87-94. doi:10.1016/J.ATHORACSUR.2011.08.002
Figures