4872
Highly Accelerated Free-Breathing Real-Time 2D Flow Imaging using Compressed Sensing and Shared Velocity Encoding1Cardiovascular MR R&D, Siemens Medical Solutions USA, Inc, Charleston, SC, United States, 2Cardiovascular MR R&D, Siemens Medical Solutions USA, Inc, Chicago, IL, United States, 3Department of Surgery, Medical University of South Carolina, Charleston, SC, United States, 4Department of Radiology and Radiological Science, Medical University of South Carolina, Charleston, SC, United States, 5MR Cardiovascular Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
We aim to demonstrate the feasibility of a highly accelerated, free-breathing RT PC technique empowered by compressed sensing (CS) and shared velocity encoding (SVE) which allows a scan time less than 5s and fast inline image reconstruction.
Introduction
2D phase contrast (PC) MRI is an established imaging technique for quantification and visualization of blood flow dynamics in the heart and large vessels [1-3]. The conventional approach often relies on retrospective electrocardiogram (ECG)-synchronized and segmented CINE acquisition of multiple heartbeats with or without respiratory control [4]. This gives only the averaged flow information and could not resolve beat-by-beat flow variations associated with irregular cardiac motion. 2D real-time (RT) PC flow MRI is a promising alternative to address the limitations of conventional PC MRI utilizing single-shot k-space data acquisition which does not rely on regular ECG and respiratory control. In this study, we present a highly accelerated, free-breathing RT PC flow imaging technique empowered by both compressed sensing (CS) and shared velocity encoding (SVE) which allows a scan time less than 5s and fast inline image reconstruction. We demonstrated its feasibility by flow measurements both in-vivo and in-vitro.Sequence Implementation
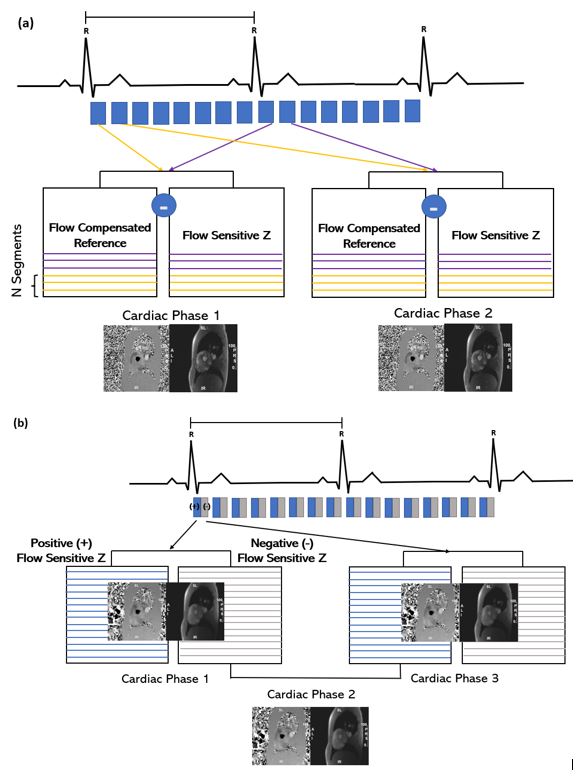
The prototype CS accelerated RT PC-MRI sequence was implemented using a single-shot fast RF-spoiled gradient echo (GRE) with SVE reconstruction to achieve a higher temporal resolution. The CS technique is characterized by sparse and incoherent sampling with variable density and a non-linear iterative reconstruction with k-t regularization [6-8]. A fully sampled central k-space data is formed by time averaging to estimate the coil sensitivity map that is further used for reconstructing subsampled data with SENSE [9]. Unlike the conventional PC-MRI, in which asymmetric velocity encoding is used to eliminate background phase error, the SVE method utilizes symmetric velocity encoding. The difference between the two approaches is illustrated in Figure1, in asymmetric velocity encoding, the velocity information was extracted using the flow encoded and flow compensated data within the same cardiac phase, whereas in symmetric velocity encoding, the velocity information was acquired from the equal and opposite flow encodings. While both result in reduced temporal resolution and increased scan time, the SVE reconstruction enables a two-fold better temporal resolution by sharing sets of k-space data between two adjacent frames in symmetric velocity encoding. The additional intermediate frames (2,4,6) share velocity data with the adjacent original frames (1,3,5) which therefore creating a new set of data that represents the velocity measurement centered at the time between the original frames [10].Flow Experiment Set Up
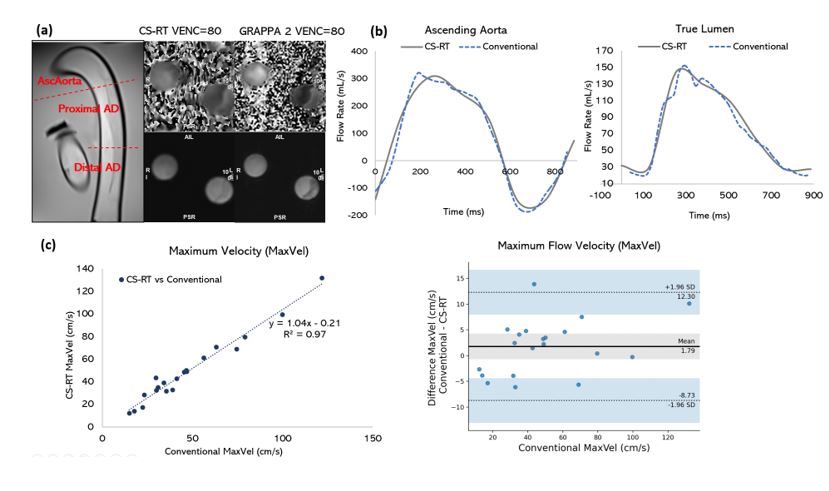
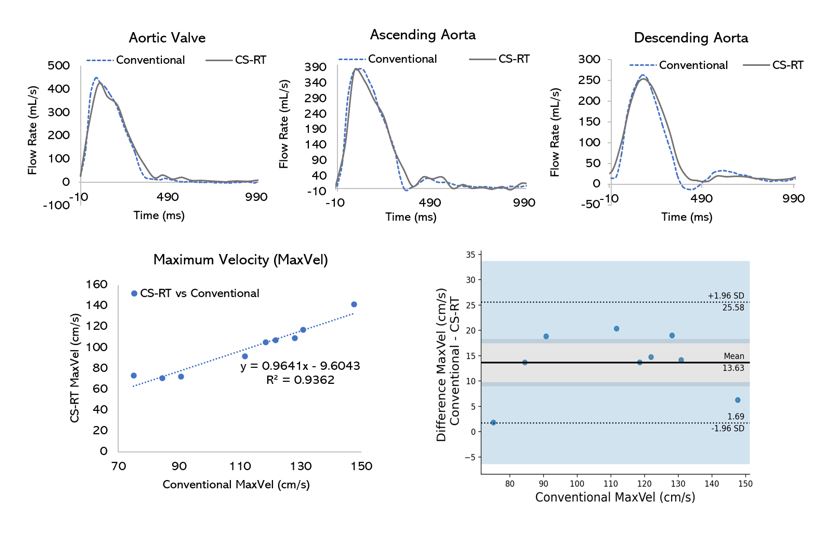
Eight phantom studies were performed using a pulsatile flow phantom (80 bpm) with silicone models of Type B aortic dissection (AD) on a 3T clinical scanner (MAGNETOM Vida, Siemens Healthcare, Erlangen, Germany). The MRI protocol included conventional segmented (GRAPPA R=2, spatial resolution 2x2x6mm3, temporal resolution 35.2ms) and prototype CS-RT (CS R=8, spatial resolution 2.5x2.5x6mm3, temporal resolution 52ms) PC techniques. Through-plane flow measurements were done at three locations (ascending, proximal and distal descending aorta). Flow parameters including the maximum velocities (MaxVel) and flow rates (MaxFlow), and the total forward blood flow (Vol/min) were calculated with a commercial software (cvi42, Circle Cardiovascular Imaging Inc., Calgary, Canada). The same PC protocols were tested in 4 healthy volunteers (Age: 25-35, 3 Male) at ascending aorta and aortic valve. The 2-tailed, paired t-tests and Bland-Altman analyses were used to evaluate for differences between flow parameters. Correlation between the two methods was assessed using linear regression with further evaluation using the intraclass correlation coefficient (ICC).Results
CS-RT enabled similar flow quantification to conventional 2D flow MR for a complete cardiac cycle both in-vitro and in-vivo with >80% reduction in scan time (2±1s vs 19±3s). Comparisons of the flow measurements at all locations in AD phantoms demonstrated an excellent correlation and agreement (MaxVel r: 0.97; ICC: 0.99, p<.001; MaxFlow r: 0.96; ICC: 0.99, p<.001; Vol/min r: 0.91; ICC: 0.97, p<.001). No significant difference was found between the two techniques (mean differences: MaxVel -1.79cm/s, p=0.15; MaxFlow 2.37ml/s, p=0.65; Vol/min -0.23, p=0.21). In healthy volunteers, a similarly good correlation and agreement (MaxVel r:0.93; ICC: 0.91, p<.001; MaxFlow r: 0.88; ICC: 0.93, p<.001; Vol/min r: 0.86; ICC: 0.92, p<.001) were found. However, CS-RT underestimated the maximum velocities within an acceptable margin(mean differences: MaxVel -13.60cm/s (12.14%), p<0.001; MaxFlow -45.47ml/s (12.46%), p=0.01; and Vol/min 0.33l/min (7%), p=0.21).Conclusion
The highly accelerated CS-RT PC technique provides >80% scan time efficiency improvement and is feasible for evaluation of cardiovascular flow patterns without requiring breath-holding. Although CS-RT 2D flow slightly underestimates the maximum flow velocities, it allows for a quick flow assessment when arrhythmia or poor respiratory control is present.Acknowledgements
No acknowledgement found.References
1. Wymer, D. T., Patel, K. P., Burke, W. F., & Bhatia, V. K. (2020). Phase-contrast MRI: Physics, Techniques, and clinical applications. RadioGraphics, 40(1), 122-140. doi:10.1148/rg.2020190039
2. Stalder, A. F., Russe, M. F., Frydrychowicz, A., Bock, J., Hennig, J., & Markl, M. (2008). Quantitative 2d and 3D phase contrast MRI: Optimized analysis of blood flow and vessel wall parameters. Magnetic Resonance in Medicine, 60(5), 1218–1231. https://doi.org/10.1002/mrm.21778
3. Gatehouse, P. D., Keegan, J., Crowe, L. A., Masood, S., Mohiaddin, R. H., Kreitner, K.-F., & Firmin, D. N. (2005). Applications of phase-contrast flow and velocity imaging in Cardiovascular MRI. European Radiology, 15(10), 2172–2184. https://doi.org/10.1007/s00330-005-2829-3
4. Sun, A., Zhao, B., Li, Y. et al. Real-time phase-contrast flow cardiovascular magnetic resonance with low-rank modeling and parallel imaging. J Cardiovasc Magn Reson 19, 19 (2017). https://doi.org/10.1186/s12968-017-0330-1
5. Forman C. et al.; High-Resolution 3D Whole-Heart Coronary MRA: A Study on theCombination of Data Acquisition in Multiple Breath-Holds and 1D Residual Respiratory Motion Compensation; Magn Reson Mater Phy; doi: 10.1007/s10334-013-0428-x (2014).
6. Greiser A., Zenge M., Schmidt M., Gulsun A., Stalder A.F.; Application of Highly Accelerated Cartesian Phase Contrast Imaging Using Compressed Sensing and Iterative Reconstruction to Real-Time and Vector Encoded Flow Imaging; #3854 Proc. ISMRM 22 (2014).
7. Greiser A., Zenge M., Schmidt M., Speier P., Mueller E.; Highly Accelerated Phase Contrast Imaging using Compressed Sensing and Iterative Reconstruction for High Resolution Short Breathhold Flow Acquisitions; #3851 Proc. ISMRM 22 (2014).
8. Greiser A, Forman C, W etzl J, Tillmanns C, Stalder AF, Schmidt M, Zenge M, Mueller E; Clinical Evaluation and Optimization of Highly Accelerated 2D and 4D Phase Contrast Flow Imaging Applications using Sparse Sampling and Iterative Reconstruction; #6076 ISMRM 23 (2015).
9. Liang, D., Liu, B., Wang, J. J., & Ying, L. (2009). Accelerating sense using compressed sensing. Magnetic Resonance in Medicine, 62(6), 1574–1584. https://doi.org/10.1002/mrm.22161
10. Lin, H. Y., Bender, J. A., Ding, Y., Chung, Y. C., Hinton, A. M., Pennell, M. L., Whitehead, K. K., Raman, S. V., & Simonetti, O. P. (2012). Shared velocity encoding: a method to improve the temporal resolution of phase-contrast velocity measurements. Magnetic resonance in medicine, 68(3), 703–710.
Figures