4869
Can blood flow and artery patency alterations in medium-to-large arteries predict alteration in cognitive function?1Vascular Imaging Lab and BioMolecular Imaging Center, Department of Radiology, University of Washington, Seattle, WA, United States, 2Institute of Science and Technology for Brain-Inspired Intelligence, Fudan University, Shanghai, China
Synopsis
Association between brain tissue level perfusion and cognitive decline has been previously documented. However, contribution of blood flow and artery patency in medium-to-large arteries and its relation to tissue level perfusion and cognition remain unclear. In this study, 3D-TOF, ASL, and SNAP, an MRA technique sensitive to slow blood flow, were acquired at baseline and 12-months follow-up. A vascular map construction software was used to measure changes in medium-to-large arterial features. Changes in SNAP artery length and branch number during follow-up were significantly associated with changes in cognitive function, while no such association was found with ASL tissue level perfusion.
Introduction:
Cerebral blood flow (CBF) plays an essential role in affecting cognition1. However, little is known about how changes in blood flow over time contribute to cognitive deficits in individuals. Current studies are mainly focused on the blood flow velocity in proximal arteries and perfusion level in the parenchyma, which are the 'frontend' and 'backend' of the cerebral vasculature. Such studies disregard the morphology and patency of medium-to-large arteries and the blood flow through them. Non-contrast enhanced MRA techniques, such as simultaneous non-contrast angiography and intraplaque hemorrhage (SNAP)2 and time of flight (TOF), are capable of measuring medium-to-large artery morphology, patency, and blood flow. Intracranial artery feature extraction (iCafe) is a custom-made semi-automatic vascular map construction software, which can measure intracranial vascular features3. iCafe measures on SNAP and TOF have shown their potential value in evaluating cerebral blood flow in several large population clinical studies4,5. Furthermore, SNAP may provide additional blood flow information due to the distal artery visibility being affected by slow blood flow velocity, as shown in simulations6. iCafe measures were also associated with the Montreal Cognitive Assessment (MoCA) scores7,8. However, it is not known whether iCafe SNAP/TOF measures can detect changes in cerebral blood flow that may accompany changes in cognition. Therefore, we aim to test whether SNAP/TOF iCafe measures can track changes in MoCA scores over 12-months in subjects with carotid atherosclerosis.Methods:
Participants:The local Institutional Review Board approved this prospective study and all participants gave written informed consent. We enrolled 25 subjects from the Intraplaque hemorrhage study. Subjects all had >15% carotid stenosis by ultrasound.
Cognitive test: MoCA scoring was used to evaluate cognition. Based on the recommended classification9, a MoCA score below 26 was considered as cognitively impaired.
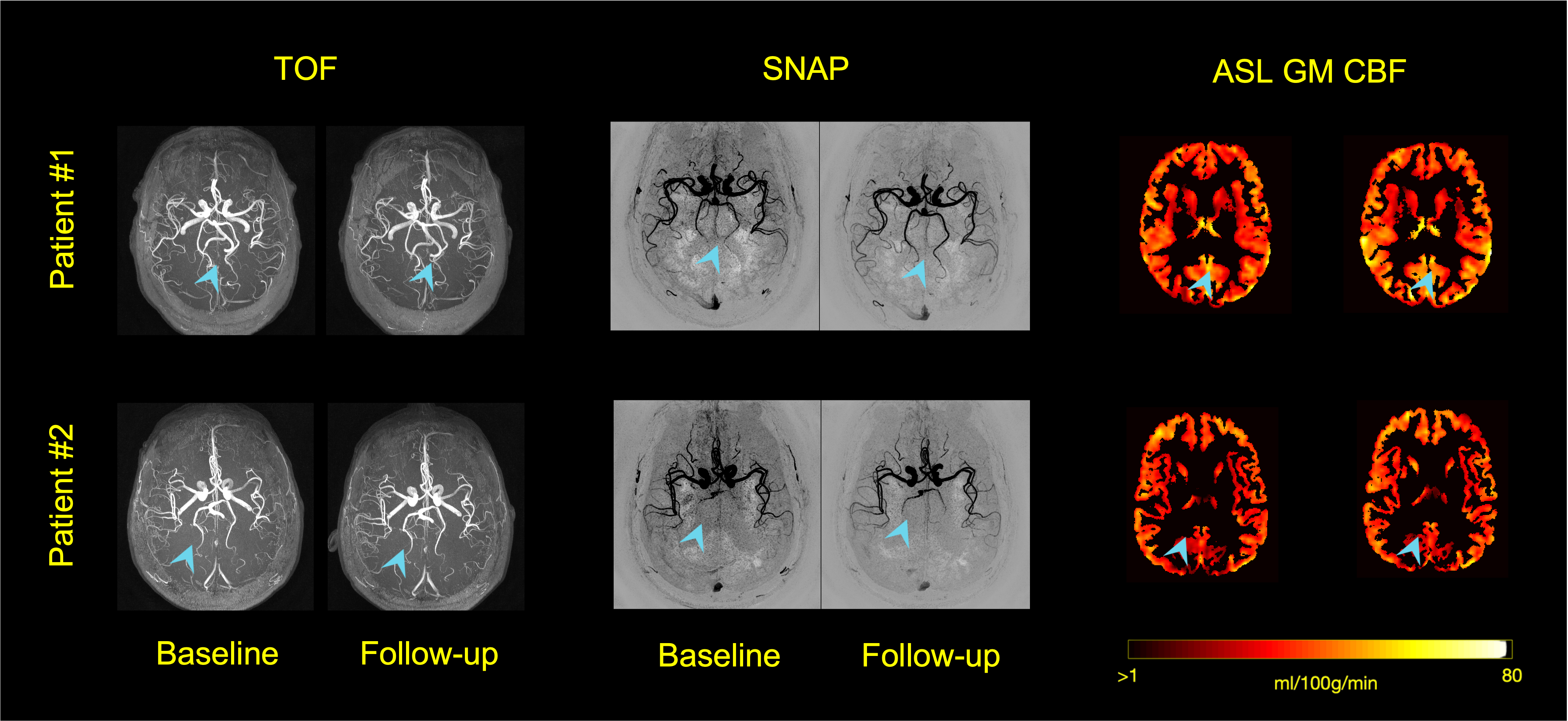
Imaging protocol: All MR studies were conducted on a 3.0-T Philips Ingenia CX scanner (Philips, Best, The Netherlands) with a 32-channel array head coil. We used 3D TOF (voxel size 0.5×0.5×1 mm3, FOV 190×180×105 mm3, TR/TE 20/3.5ms, flip angle (FA) 18 degrees, with spoiled gradient echo readout (SPGR)) and SNAP (voxel size 0.8mm isotropic, FOV 180×180×70 mm3, TR/TE 11/5.6ms, FA 11 degrees, with SPGR) to visualize medium-to-large cerebral arteries. 3D pseudo-continuous ASL (balanced pCASL, RF duration 0.48ms, RF interval 1.21ms, FA 28 degrees, maximum gradient strength 5 mT/m) was performed to obtain parenchymal blood flow.
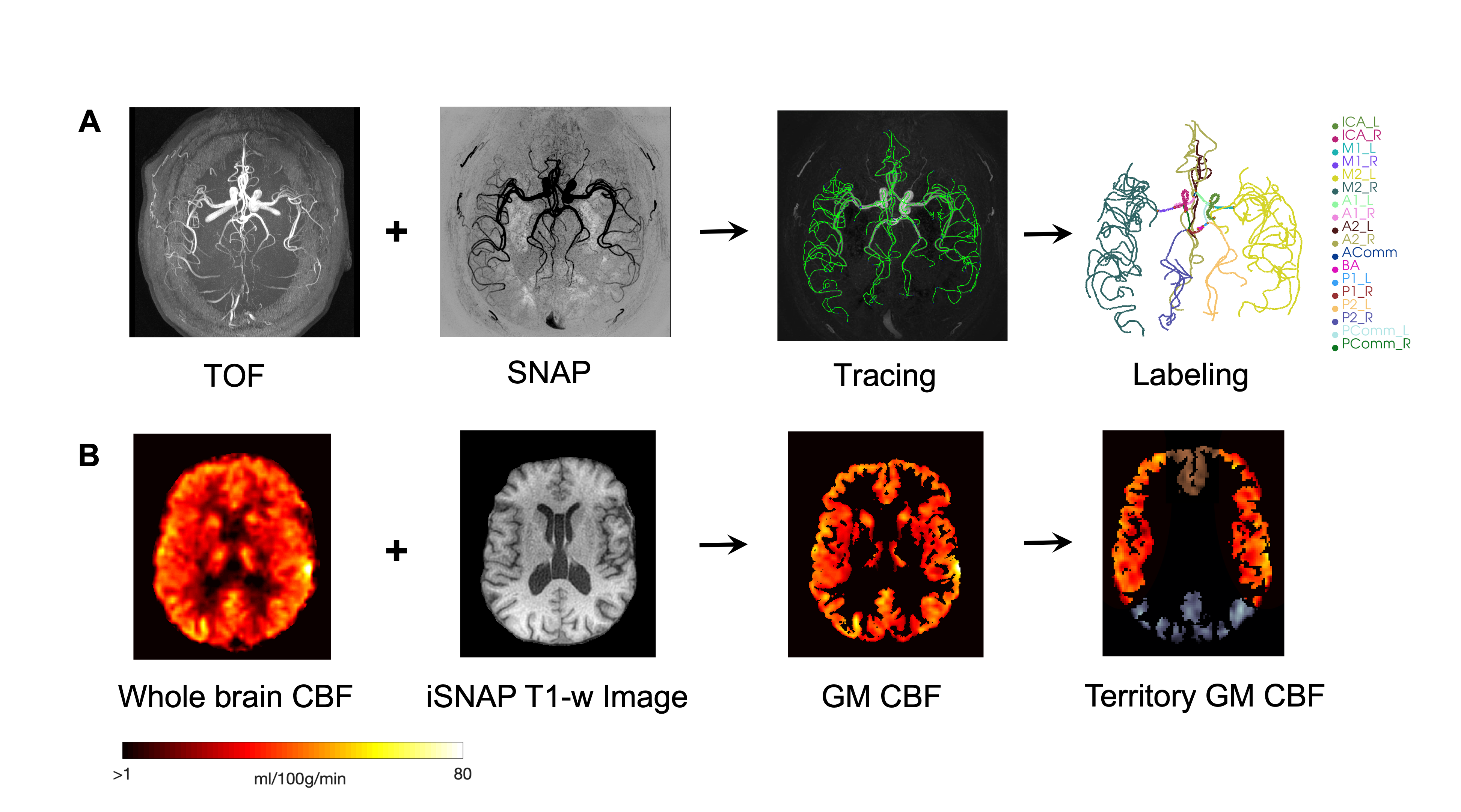
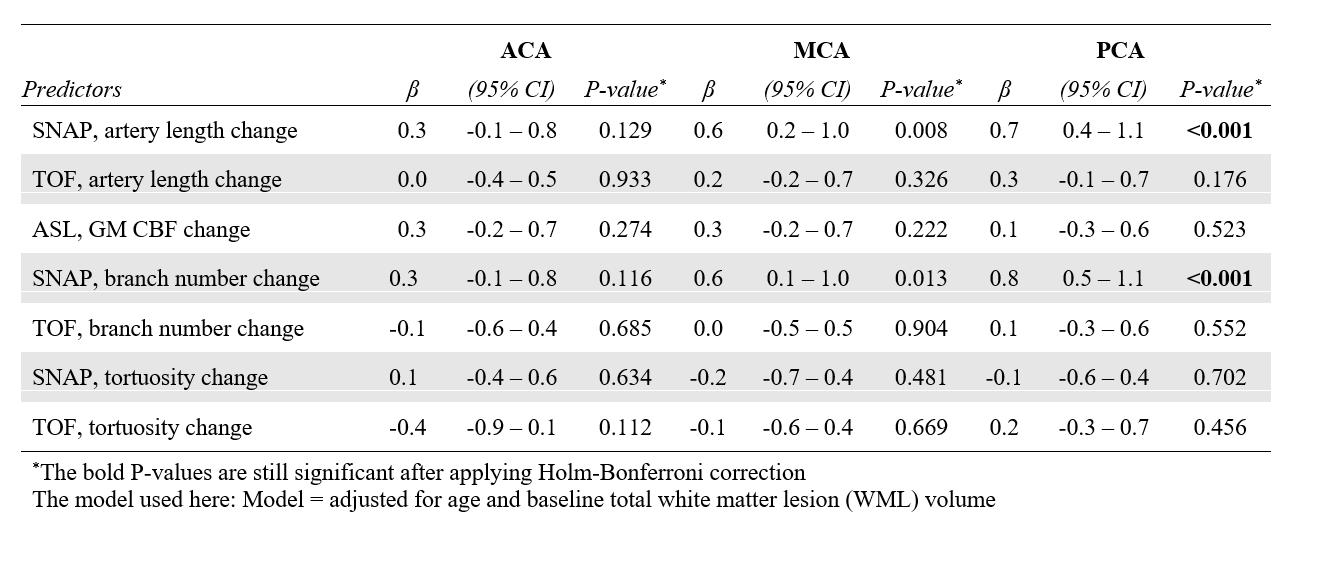
Image analysis: The overall workflow for TOF and SNAP, as well as ASL processing, are shown in Figure 1. Centerlines are traced with a deep learning-based open curve active contour algorithm10 and then each segment is labeled with its artery name using iCafe. For ASL processing, recommended implementation of the hemodynamics model was used11, and only grey matter (GM) CBF was measured. In addition to whole-brain measurements, TOF, SNAP, and ASL measurements were examined in the anterior cerebral artery (ACA), middle cerebral artery (MCA), and posterior cerebral artery (PCA) territories. All segmentation and registration processes are based on the SPM platform12.
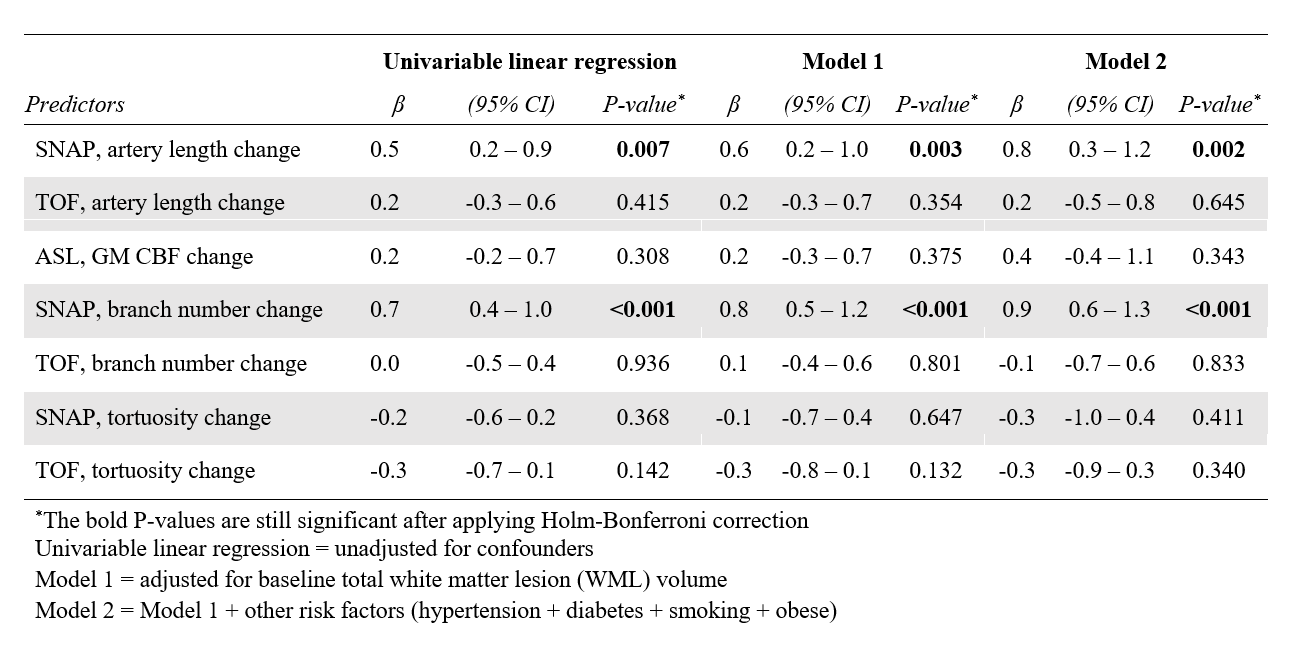
Statistical analysis: Statistical analyses were performed using the statistical computing language R (version 3.6.1; R Foundation for Statistical Computing, Vienna, Austria). Univariable regression between cerebral vascular feature change (artery length, branch number, tortuosity) and MoCA score change was first performed. Then, partial linear regression models were applied considering other confounding factors. Finally, the subjects were stratified into cognitively intact and cognitively impaired groups, and the same univariable and partial linear regression analyses were performed for both groups. Bonferroni correction was applied for multiple testing.
Results:
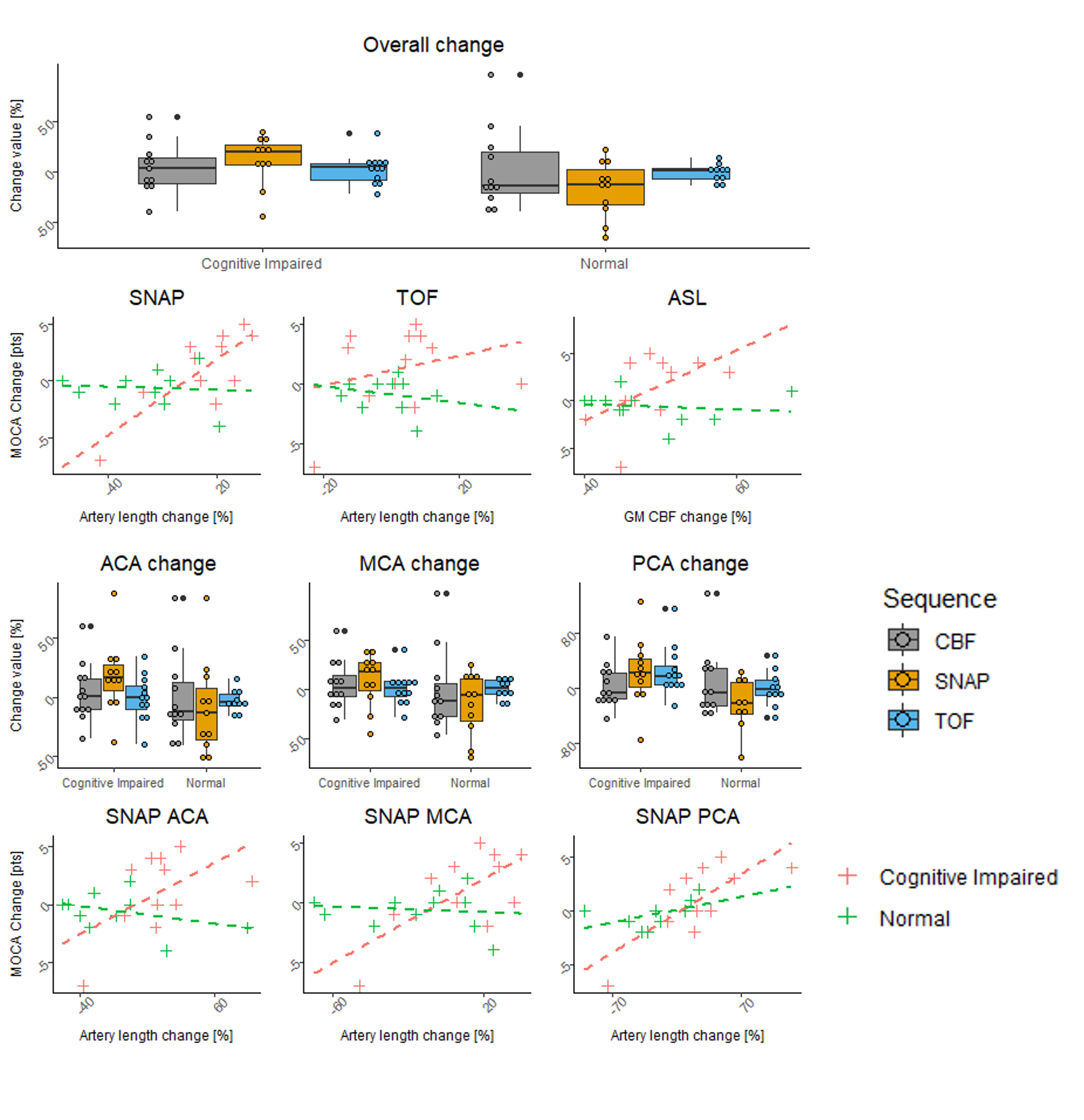
SNAP-measured artery length and branch number changes were significantly associated with MoCA score change, as shown in Table 1. When adding other confounders to the partial regression model, the SNAP-measured artery length, as well as the total branch number, still showed significant associations in all 3 models. The SNAP-measured artery length and branch number in the PCA territory were associated with MoCA score change, while artery length and branch number change in the ACA and MCA territories were not associated with MoCA score change, as shown in Table 2. When comparing cognitively intact and impaired groups, global and PCA territory SNAP length changes were significantly associated with MoCA score change in the cognitively impaired group only. Changes in TOF MRA measures and ASL CBF did not show any associations with MOCA change.Conclusion:
In this prospective study, we demonstrated that changes in cognition can be assessed based on changes in cerebral blood flow and artery patency in medium-to-large arteries using SNAP MRA. SNAP measurements of total artery length and total artery branch number were found to be associated with the MoCA score change after adjusting for other clinical confounders, especially in the PCA territory. However, features measured on TOF and GM CBF from ASL did not show significant associations. This suggests that SNAP is more sensitive than TOF and ASL to capture blood flow or artery patency changes in medium-to-large arteries in patients with carotid atherosclerosis. In addition, changes in SNAP iCafe measures were able to distinguish between the cognitively impaired group and the normal cognition group. Our results suggest that changes in cerebral medium-to-large blood flow may be associated with changes in cognition in subjects with carotid atherosclerosis and these changes can be tracked using SNAP MRA.Acknowledgements
This work was supported in part by NIH grant R01HL103609.References
1. Iadecola, Costantino, et al. "Vascular cognitive impairment and dementia: JACC scientific expert panel." Journal of the American College of Cardiology 73.25 (2019): 3326-3344.
2. Wang, Jinnan, et al. "Simultaneous noncontrast angiography and intraplaque hemorrhage (SNAP) imaging for carotid atherosclerotic disease evaluation." Magnetic resonance in medicine 69.2 (2013): 337-345.
3. Chen, Li, et al. "Development of a quantitative intracranial vascular features extraction tool on 3D MRA using semiautomated open‐curve active contour vessel tracing." Magnetic resonance in medicine 79.6 (2018): 3229-3238.
4. Liu, Wenjin, et al. "Uncontrolled hypertension associates with subclinical cerebrovascular health globally: a multimodal imaging study." European Radiology 31.4 (2021): 2233-2241.
5. Xiong, Yuhui, et al. "Intracranial simultaneous noncontrast angiography and intraplaque hemorrhage (SNAP) MRA: Analyzation, optimization, and extension for dynamic MRA." Magnetic resonance in medicine 82.5 (2019): 1646-1659.
6. Zhang, Qiang, et al. "Angiographic contrast mechanism comparison between Simultaneous Non-contrast Angiography and intraPlaque hemorrhage (SNAP) sequence and Time of Flight (TOF) sequence for intracranial artery." Magnetic resonance imaging 66 (2020): 199-207.
7. Chen, Zhensen, et al. "Shorter Length of Visible Intracranial Arteries on Non-contrast Enhanced MRA is Associated with Cognitive Impairment". Society of magnetic resonance angiography 43 (2021).
8. Nasreddine, Ziad S., et al. "The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment." Journal of the American Geriatrics Society 53.4 (2005): 695-699.
9. Damian, Anne M., et al. "The Montreal Cognitive Assessment and the mini-mental state examination as screening instruments for cognitive impairment: item analyses and threshold scores." Dementia and geriatric cognitive disorders 31.2 (2011): 126-131.
10. Chen, Li, et al. "Deep Open Snake Tracker for Vessel Tracing." International Conference on Medical Image Computing and Computer-Assisted Intervention. Springer, Cham, 2021.
11. Alsop, David C., et al. "Recommended implementation of arterial spin‐labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia." Magnetic resonance in medicine 73.1 (2015): 102-116.
12. https://www.fil.ion.ucl.ac.uk/spm
Figures