4779
Improved myocardial T1 mapping accuracy with Deep Learning reconstruction of low flip angle MOLLI series1GE Healthcare, Barcelona, Spain, 2GE Healthcare, Madrid, Spain, 3GE Healthcare, London, United Kingdom, 4Imperial College Healthcare NHS Trust, London, United Kingdom, 5Servicio de diagnóstico por la imagen, Hospital Universitario Quirónsalud, Madrid, Spain, 6Servicio de cardiología, Hospital Universitario Quirónsalud, Madrid, Spain
Synopsis
In this study, we explore the possibility of leveraging Deep Learning regularized reconstruction to enable lower flip angle MOLLI acquisition for myocardial T1 mapping. It has been shown in the past that lowering flip angle helps reduce various artifact sources, at the cost of lower signal to noise ratio. Regularized reconstruction can effectively manage image noise as well as increase feature sharpness. This hypothesis has been tested on a group of clinical patients referred for a cardiac MR exam.
INTRODUCTION
The relaxation properties of myocardial tissue have been shown to be a reliable indicator of heart diseases related to extracellular changes (such as oedema and fibrosis), fat, iron and amyloid content1,2. Tissue characterization by means of T1 mapping enables the use of quantitative criteria in clinical diagnosis.The typical implementation of T1 mapping involves the acquisition of a series of inversion or saturation recovery measurements, followed by pixel-wise fitting of an exponential relaxation model. In the case of inversion recovery measurements, Modified Look-Locker (MOLLI) sequences are generally used to speed up the acquisition. One drawback of this sequence is the disturbance introduced in the inversion recovery by the readout pulses. Using lower flip angles can mitigate this effect and makes the measurement more robust to heart rate and off-resonance variations, but at the cost of reduced signal-to-noise (SNR).
Novel reconstruction methods based on Deep Learning (DL) are trained on large image databases to make more efficient use of the acquired data, producing sharper images with higher SNR3. The goal of the present study was to evaluate whether DL reconstruction can be leveraged to enable lower flip angle MOLLI acquisition in clinical T1 mapping.
METHODS
A group of 10 subjects (6 male, 4 female; age 59±12 [37,76]; weight 79±20kg [51,130]) referred to Hospital Universitario Quironsalud (Madrid, Spain) for a clinically indicated CMR exam were included in this study. All subjects were scanned on a 1.5T MR450w system (GE Healthcare, Waukesha, WI). The protocol included the site’s standard T1 mapping MOLLI series (short axis stack and 4-chamber view): FIESTA FGRE sequence, 5(3)3, FOV=380mm, ST=8mm, TR=3.0ms, TE=1.4ms, matrix 160x128, FA=35, BW=83.3kHz, NEX=1, ASSET=2, resolution=1.48x1.48mm2, Body 30 Small coil. Several replicas of this series were acquired, with flip angles 35, 30, 25, and 20deg.The acquired data were anonymized and exported for offline reconstruction. Two algorithms implemented using GE’s Orchestra library were applied: A 2D Cartesian reconstruction equivalent to the one in the scanner; and AIR Recon DL, a reconstruction based on a convolutional neural network trained to provide sharpened and de-noised images3.
The reconstructed datasets were post-processed and reviewed by a cardiologist with 4 years of CMR experience, using cvi42 (Circle Cardiovascular Imaging Inc., Calgary, CA). Custom analysis scripts were implemented in Matlab (The Mathworks Inc., Natick, MA) to provide quantitative image quality metrics (ROI & pixel-wise T1 statistics, fitting R2 histogram analysis).
To confirm the clinical findings, a series of equivalent measurements were performed using the T1 Mapping and ECV Standardization (T1MES) phantom4.
RESULTS
All cases were successfully reconstructed with both methods. Figure 1 illustrates the typical image quality obtained with both methods, for each of the MOLLI flip angle settings.No clinical finding was reported regarding T1 mapping measurements. Normal T1 values and ECV measurements were obtained for all patients involved in this study. The rest of the clinical protocol didn’t show any hyperintensities in the MDE sequences and two cases showed a certain degree of LV hypertrophy as well as mild aortic regurgitation. The Deep Learning method was found to provide better qualitative results compared to the current clinical standard, improving confidence in diagnosis with respect to the standard series.
The coefficient of determination (R2) of the exponential fitting was used as a surrogate of T1 accuracy. The R2 distribution in the cardiac area showed a consistent increase of high R2 pixels with DL reconstruction. Table 1 shows the impact of DL reconstruction on the peak of the R2 histogram (i.e., the number of cardiac pixels with a good T1 fit). This improvement increased for lower flip angle acquisitions, indicating effective noise compensation, as illustrated in figure 2.
The impact of DL reconstruction was minor on the T1 values obtained on large myocardial regions of interest (ROI), as seen in figure 3. Two-tailed paired t-tests show P values of 0.93 for FA35, 0.67 for FA30 and 0.64 for FA25. Pixel-wise maps, on the other hand, clearly showed increased T1 deviation with lower flip angles, effectively compensated with the DL (see table 2).
The measurements of the T1MES phantom showed (in comparison with the reference measurements) the expected improvement of T1 accuracy with decreasing flip angles, with absolute differences of 7.2%±4.1% for 35deg, 6.6%±3.6% for 30deg, 6.2%±3.1% for 25deg and 5.4%±3.2% for 20deg.
DISCUSSION
Lowering the flip angle settings of MOLLI acquisitions reduces the impact of several sources of inaccuracy in T1 mapping. With the use of Deep Learning reconstruction methods, this can be achieved without significantly increasing image noise.The qualitative review of the acquired clinical cases clearly confirmed DL to be the preferred reconstruction method for T1 mapping purposes. No instances of loss of diagnostically relevant information were reported.
The use of lower flip angles showed the expected increase both in estimated T1 consistency and in image noise. The former showed optimal results for FA30 acquisitions. The latter could be effectively managed by DL reconstruction, with FA25 acquisitions showing noise levels comparable to standard FA35 images.
CONCLUSION
The results obtained in this study support the hypothesis that DL reconstruction can be leveraged to enable lower FA acquisition of MOLLI series, achieving more accurate and consistent pixel-wise T1 estimates and increased robustness to artifacts.Acknowledgements
No acknowledgement found.References
1. Jellis, C. L. & Kwon, D. H. Myocardial T1 mapping: modalities and clinical applications. Cardiovasc Diagn Ther 4, 126–137 (2014).
2. Radenkovic, D., Weingärtner, S., Ricketts, L., Moon, J. C. & Captur, G. T1 mapping in cardiac MRI. Heart Fail Rev 22, 415–430 (2017).
3. Lebel, RM. "Performance characterization of a novel deep learning-based MR image reconstruction pipeline.", arXiv:2008.06559 (2020).
4. Captur, G., Gatehouse, P., Keenan, K.E. et al. A medical device-grade T1 and ECV phantom for global T1 mapping quality assurance—the T1 Mapping and ECV Standardization in cardiovascular magnetic resonance (T1MES) program. J Cardiovasc Magn Reson 18, 58 (2016).
Figures
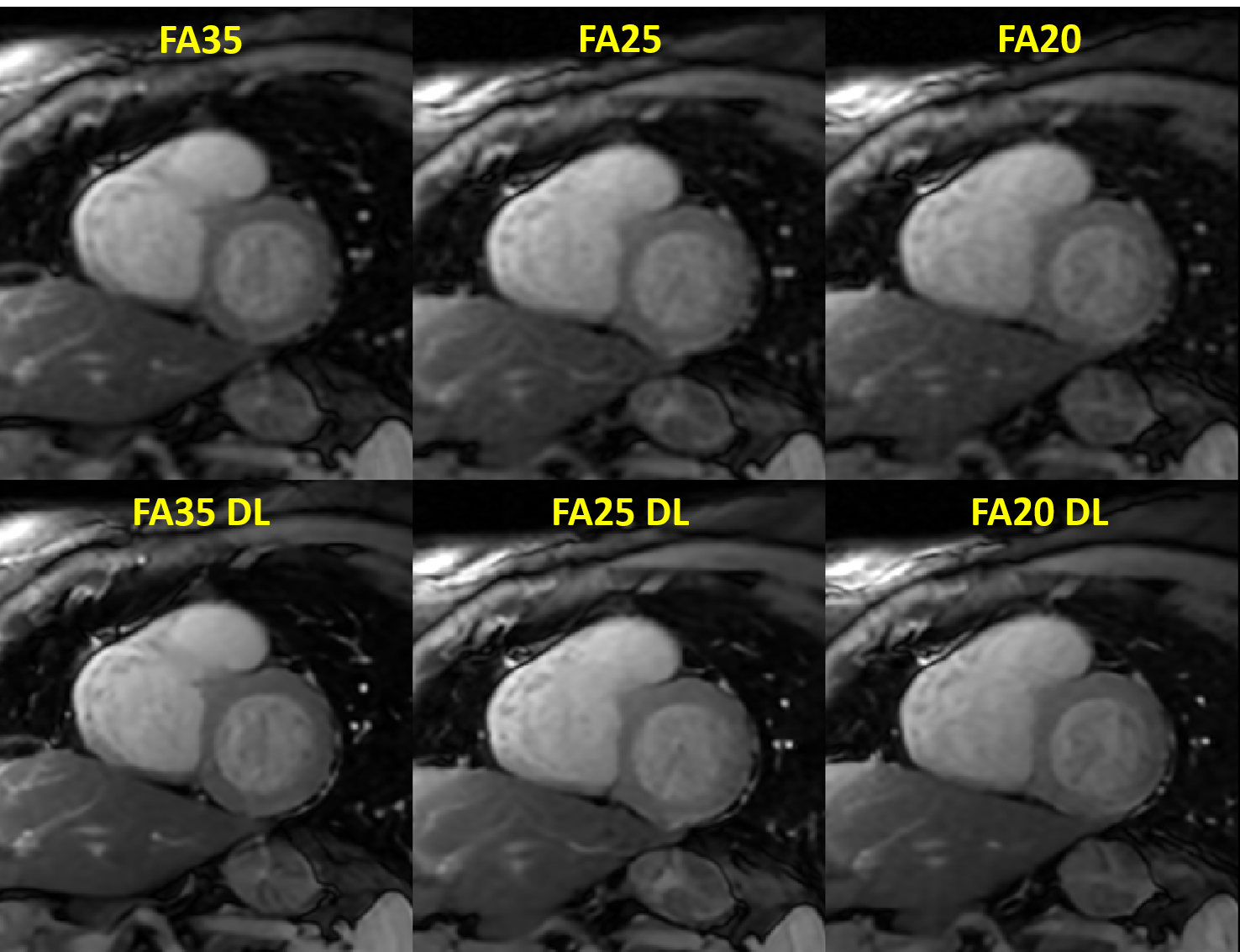
Figure 1.- Short axis cardiac views illustrating the image quality obtained using MOLLI series with different flip angle settings. The top row shows the results of the standard reconstruction, and the bottom row the corresponding Deep Learning reconstruction.
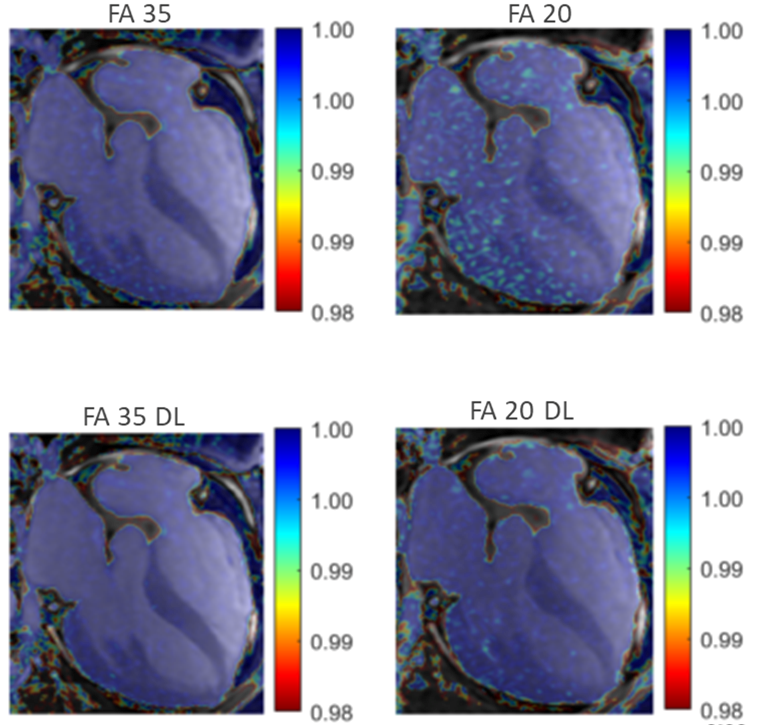
Figure 2.- Maps of the coefficient of determination (R2) of the exponential T1 fitting, superimposed on the corresponding MOLLI frames. With standard reconstruction (top row), lower FA causes a noticeable degradation of the fitting performance. This is mitigated using DL reconstruction (bottom row).
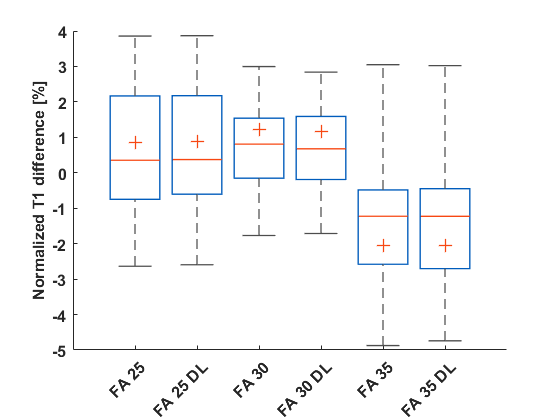
Figure 3.- Box plot showing the variability of the T1 value over the different subjects, measured on a myocardial ROI with different flip angle settings, for each reconstruction method. The measured differences were normalized by the mean value.
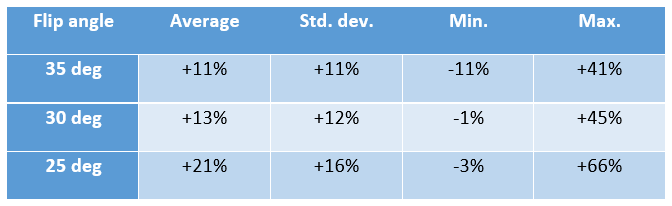
Table 1.- Impact of DL reconstruction on the R2 histogram peak, compared to standard reconstruction. Positive values denote an increase of cardiac pixels with good conformance to the exponential inversion recovery model, suggesting improved T1 accuracy.
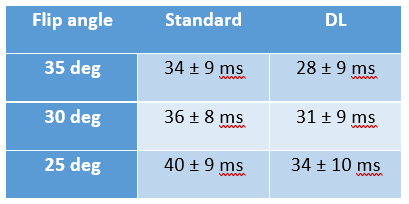
Table 2.- Standard deviation of the pixel-wise T1 estimates in a myocardial ROI, for each flip angle and reconstruction setting, averaged over all subjects.