4778
Myocardial stress field from combined CMR and FEM in ALL survivors
Mehdi Ghafarinatanzi1
1Polytechnique Montréal, Montreal, QC, Canada
1Polytechnique Montréal, Montreal, QC, Canada
Synopsis
The objective of this study is to investigate the myocardial 3D strain stress field of the patient-specific left ventricles in children with acute lymphoblastic leukemia (ALL) after treatment. The virtual field-finite element approach is applied to the 3D mesh generated tetrahedral for each patient-specific geometry over the cardiac cycle. The results illustrate the difference in distribution stress and displacement field for each LV subject.
Introduction
doxorubicin-based chemotherapy is an effective way to treat acute lymphoblastic leukemia (ALL). However, its success is hindered by cardiotoxic effects depending on the doxorubicin dose received during the treatment. Changes in Left ventricle myocardial deformation are an important determinant of systolic and diastolic dysfunction and the main cause of heart failure occurred at doxorubicin cardiotoxicity. The assessment of left ventricular (LV) strain provides useful knowledge and for the early detection of doxorubicin-induced cardiotoxicity. In recent years, 3D imaging technology and finite element modeling (FEM) have been used to quantify mechanical strain/stress within the myocardium. However, the accuracy of measurements of LV deformation data may affect strain parameters, may depend on the techniques calculating their values. Applying FEM and virtual field method (VFM) to 3D Cine-CMR data, this study estimates mechanical strain and stress all over the cardiac cycle (systole and diastole) in childhood ALL survivors who previously received doxorubicin therapy. In VFM application, with the generation of the mesh model of the left ventricle, and the strain virtual fields which are kinematically admissible to full-field LV deformation, we estimate the stiffness of the myocardium from a reverse identification approach [1].
doxorubicin-based chemotherapy is an effective way to treat acute lymphoblastic leukemia (ALL). However, its success is hindered by cardiotoxic effects depending on the doxorubicin dose received during the treatment. Changes in Left ventricle myocardial deformation are an important determinant of systolic and diastolic dysfunction and the main cause of heart failure occurred at doxorubicin cardiotoxicity. The assessment of left ventricular (LV) strain provides useful knowledge and for the early detection of doxorubicin-induced cardiotoxicity. In recent years, 3D imaging technology and finite element modeling (FEM) have been used to quantify mechanical strain/stress within the myocardium. However, the accuracy of measurements of LV deformation data may affect strain parameters, may depend on the techniques calculating their values. Applying FEM and virtual field method (VFM) to 3D Cine-CMR data, this study estimates mechanical strain and stress all over the cardiac cycle (systole and diastole) in childhood ALL survivors who previously received doxorubicin therapy. In VFM application, with the generation of the mesh model of the left ventricle, and the strain virtual fields which are kinematically admissible to full-field LV deformation, we estimate the stiffness of the myocardium from a reverse identification approach [1].
Materials and methods
The data used in this study comes from the PETAL study [2] in which the ALL survivors were divided into 3 groups according to their prognostic risk to the doxorubicin: standard risk (SR, n=3), high risk (HR, n=3) and high-risk group who received dexrazoxane, a cardioprotective agent (HRdex, n=3). The CMR acquisitions were performed at rest on a Siemens Skyra 3T MR system using an 18-channel phased-array body matrix coil and included an ECG-gated cine TruFISP sequence (14 slices in short axis and 5 slices in long axis, slice thickness 8mm, repetition time 34.6ms, effective echo time 1.2ms, flip angle 38°, iPAT factor 3, matrix 208x210 and in-plane pixel size 1.25x1.25 mm). The patient-specific shape of the left ventricle was extracted at each phase of the cardiac cycle using a semi-automatic segmentation (CIM v8.1, University of Auckland), and displacements between phases were computed [2]. Myocardial geometry was meshed into 6144 tetrahedral elements and then deformed under the experienced displacements. The virtual field strain was implemented in mechanical strain-stress relation for the LV myocardium [3]. The finite element mesh was used to estimate myocardial stiffness by discretizing the equations of the principle of the virtual work. Later, actual stresses (von Mises index) were obtained for each element at the end of systole, diastasis, and at the end of diastole, and compared between the three groups (HR, HRdex, SR).
Results
The Von-Mises strain remained almost similar behavior for the three groups during systole, increased slightly from SR to HR during diastole, and decreased in SR at end-diastole (Figure 1). The Von-Mises stress increased in HR at end-systole, increased in SR at diastasis, and decreased in SR at end-diastole (Figure 2). The distribution of nodal displacement at end of systole was similar for the 3 groups with the highest displacement found in the anterior basal area (Figure 3).
Discussion
The literature indicates a significant reduction in the myocardial diastolic function for SR patients compared to HR. The reduction in the myocardial relaxation function in ALL survivor’s stresses that remained similar between ALL survivors suggests that myocardial changes may be local rather than generalized over myocardium. Strain reduction in HR and HRdex groups as compared to SR, corresponds to an increase of the amount of the muscle fibers in the myocardium, in agreement with doxorubicin-induced cardiotoxicity. The results data showed that as the dose of doxorubicin increased, the strain values and left ventricle function reduced, and it caused the progression to HF.
Conclusion
Our technique in the combination with the virtual field method and mesh generation allowed personalized LV restructuration at each cardiac phase and assessed the subtle changes using stress and strain analysis due to childhood cardiotoxicity based on cine-MRI images.
The data used in this study comes from the PETAL study [2] in which the ALL survivors were divided into 3 groups according to their prognostic risk to the doxorubicin: standard risk (SR, n=3), high risk (HR, n=3) and high-risk group who received dexrazoxane, a cardioprotective agent (HRdex, n=3). The CMR acquisitions were performed at rest on a Siemens Skyra 3T MR system using an 18-channel phased-array body matrix coil and included an ECG-gated cine TruFISP sequence (14 slices in short axis and 5 slices in long axis, slice thickness 8mm, repetition time 34.6ms, effective echo time 1.2ms, flip angle 38°, iPAT factor 3, matrix 208x210 and in-plane pixel size 1.25x1.25 mm). The patient-specific shape of the left ventricle was extracted at each phase of the cardiac cycle using a semi-automatic segmentation (CIM v8.1, University of Auckland), and displacements between phases were computed [2]. Myocardial geometry was meshed into 6144 tetrahedral elements and then deformed under the experienced displacements. The virtual field strain was implemented in mechanical strain-stress relation for the LV myocardium [3]. The finite element mesh was used to estimate myocardial stiffness by discretizing the equations of the principle of the virtual work. Later, actual stresses (von Mises index) were obtained for each element at the end of systole, diastasis, and at the end of diastole, and compared between the three groups (HR, HRdex, SR).
Results
The Von-Mises strain remained almost similar behavior for the three groups during systole, increased slightly from SR to HR during diastole, and decreased in SR at end-diastole (Figure 1). The Von-Mises stress increased in HR at end-systole, increased in SR at diastasis, and decreased in SR at end-diastole (Figure 2). The distribution of nodal displacement at end of systole was similar for the 3 groups with the highest displacement found in the anterior basal area (Figure 3).
Discussion
The literature indicates a significant reduction in the myocardial diastolic function for SR patients compared to HR. The reduction in the myocardial relaxation function in ALL survivor’s stresses that remained similar between ALL survivors suggests that myocardial changes may be local rather than generalized over myocardium. Strain reduction in HR and HRdex groups as compared to SR, corresponds to an increase of the amount of the muscle fibers in the myocardium, in agreement with doxorubicin-induced cardiotoxicity. The results data showed that as the dose of doxorubicin increased, the strain values and left ventricle function reduced, and it caused the progression to HF.
Conclusion
Our technique in the combination with the virtual field method and mesh generation allowed personalized LV restructuration at each cardiac phase and assessed the subtle changes using stress and strain analysis due to childhood cardiotoxicity based on cine-MRI images.
Acknowledgements
NSERC and Polytechnique Montreal for the financial support, researchers from the PETALE study for the opportunity to do these complementary analyses on the cancer survivors.References
1. Périé D., Ghafari M., Curnier D. (2020). Identification of hyperelastic properties of the myocardium from CMR patient-specific 3D geometry and the Virtual Field Method. International Research Society on Magnetic Resonance in Medicine, Virtual Conference & Exhibition.2. Périé D., Gamba M., Trempe M., Wang J., Nash M., Young A., Curnier D. (2018) Subtle changes in Hyper-elastic properties of the myocardium with cardiotoxicity remodeling from CMR. International Research Society on Magnetic Resonance in Medicine, Paris (France).
3. Miller, Renee, et al. Estimation of transversely isotropic material properties from magnetic resonance elastography using the optimized virtual fields method. International journal for numerical methods in biomedical engineering 34.6 (2018): e2979.
Figures
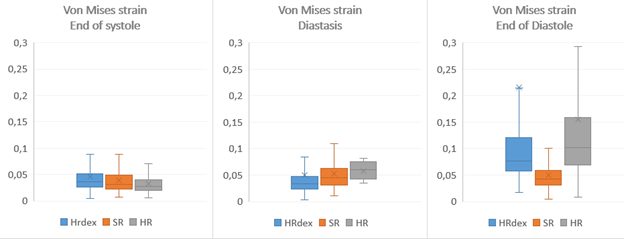
Figure1: Von-Mises Strain at end of
systole (left), diastasis (center), and end of diastole (right)
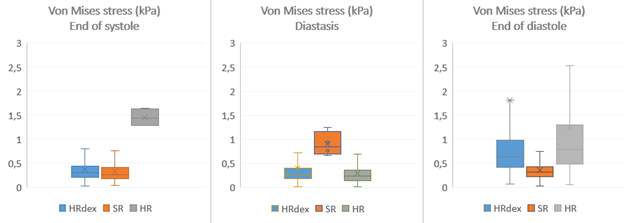
Figure2: Von-Mises Stress at end of systole (left), diastasis (center), and end of
diastole (right)
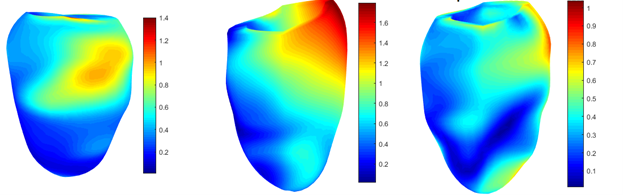
Figure3: Nodal displacement (mm) at end of systole, HRdex (left), SR(center), and HR (right)
DOI: https://doi.org/10.58530/2022/4778