4730
Assessment of renal injury in patients with IgA nephropathy using mono-exponential DWI vs IVIM derived from advanced zoomed-FOV DWI1Department of Radiology, Zhongshan Hospital, Fudan University, Shanghai, China, 2Department of Nephrology, Zhongshan Hospital, Fudan University, Shanghai, China, 3MR Application Development, Siemens Shenzhen Magnetic Resonance Ltd, Shenzhen, China, 4MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
The use of intravoxel incoherent motion (IVIM) and diffusion-weighted imaging (DWI) has increased for renal function and fibrosis assessments. However, debates have continued about which method is best. In this study, we used IVIM to assess the pathologic injury associated with IgA nephropathy and compared the results with the mono-exponential model of DWI. Both diffusion models were derived from advanced zoomed field of view (FOV) DWI acquisitions. IVIM had better diagnostic performance than the mono-exponential model in assessing the renal pathologic injury in patients with IgA nephropathy.
Introduction
Epidemiologic studies have revealed that chronic kidney disease (CKD) has become a major public health problem worldwide[1, 2]. IgA nephropathy is a common pathologic type of CKD that can result in progressive loss of renal function and the eventual occurrence of poorly controlled end-stage renal disease (ESRD) [3-5]. Delaying the progression of IgA nephropathy is currently the main treatment strategy; therefore, a precise evaluation of the renal pathologic injury during the follow-up visits is important. Currently, renal biopsy is the only means of assessing the severity of renal pathologic injury in patients with IgA nephropathy and is significant for guiding therapy and evaluating prognosis [6]. Nonetheless, biopsies are rarely used in clinical medicine because of the complication risks [7], such as perirenal hematoma, infection, and hematuria [8]; it is also difficult to repeat for longitudinal monitoring. Thus, it is imperative that an accurate and non-invasive imaging technique be developed for effective follow-up of this disease. Thus, our study aimed to investigate the value of intravoxel incoherent motion (IVIM) using advanced zoomed-field of view (FOV) diffusion-weighted imaging [9] to assess the renal pathologic injury of IgA nephropathy and compare it to the mono-exponential diffusion-weighted imaging (DWI) model.Methods
This prospective study included 50 subjects (40 patients with biopsy-proven IgA nephropathy and 10 healthy volunteers). A 3T MRI system (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) was used for all MRI examinations. A prototype zoomed-FOV DWI (zoomed DWI) was used to acquire multiple-b data. To further improve the image quality of zoomed DWI, a slight rotation of the field-of-excitation [10], motion registration [11], and complex averaging [12] were performed. Other parameters were as follows: TR/TE=4000/54ms; slice thickness=5 mm; FOV=160x400mm2; scan matrix = 84x200, bandwidth=2084 Hz; b= 0, 25, 50, 80, 100, 150, 300, 500, 800, and 1000 s/mm2 with a 4-scan trace diffusion mode, free-breathing, and acquisition time=5 min 40 s. The prototypical MR Body Diffusion Toolbox (Siemens Healthcare, Erlangen, Germany) was used to calculate the IVIM parametric maps and ADC maps using all acquired b-value images. The apparent diffusion coefficient (ADC), true diffusivity (D), pseudo-diffusion coefficient (D*), and perfusion fraction (f) values of the right renal parenchyma were measured from the fitted maps. Renal biopsies were performed within 3 days after the MR examination. All renal biopsy specimens were evaluated by a pathologist to calculate the renal pathologic injury scores, including the glomerular injury score, tubulointerstitial injury score, and vascular injury score. All patients with IgA nephropathy were divided into two groups based on the pathology scores, a mild renal injury group and a moderate-severe (m-s) renal injury group. Furthermore, 10 healthy volunteers were recruited as the control group. The differences in the DWI-derived parameters among the three groups were compared using a one-way analysis of variance (ANOVA). The diagnostic performance of the DWI-derived parameters in assessing renal pathologic injury was evaluated using receiver operating characteristic (ROC) curves. A Pearson correlation analysis was applied to assess the relationship between the renal pathologic injury scores and the DWI-derived parameters. All data were analyzed using SPSS (Version 22, IBM, Armonk, NY, USA) and MedCalc for Windows (version 14.8.1, Ostend, Belgium) software. Differences with p values < 0.05 were regarded statistically significant.Results
Figure 1 shows a representative example of diffusion parameter maps in the kidney, including ADC, D, D*, and f maps. Figure 2 display the DWI-derived parameters of the three groups. A significant difference was found for the DWI-derived parameters among the three groups (all P< 0.01). DWI-derived parameters of the control and mild renal injury groups were significantly higher than those in the m-s renal injury group (all P < 0.01). The analytic results of the ROC curve analysis for the DWI-derived parameters in evaluating renal pathologic injury are summarized in Table 1. The ROC analysis indicated that the f value had the highest diagnostic value for distinguishing the mild and m-s renal injury groups (AUC values of 0.891) and the control and m-s renal injury groups (AUC values of 0.908). The renal pathologic injury scores had the highest correlation coefficients with renal parenchymal f values (r=-0.84, P<0.01), followed by the D*, ADC, and D values, with r values of -0.77, -0.54, and -0.53, respectively (all P<0.01).Discussion and conclusion
In this study, the renal parenchymal f value had the strongest correlation with renal pathologic injury scores in patients with IgA nephropathy. This parameter showed the largest AUCs in being able to distinguish the mild and m-s renal injury groups. It also could distinguish the m-s renal injury and control groups. Therefore, our study results revealed that using advanced zoomed DWI, IVIM had better diagnostic performance compared with the mono-exponential model in evaluating the renal pathologic injury in patients with IgA nephropathy.Acknowledgements
None
References
1. Gupta T, Paul N, Kolte D, et al. Association of chronic renal insufficiency with in-hospital outcomes after percutaneous coronary intervention. J Am Heart Assoc 2015;4(6):e2069.
2. Onuigbo MA, Agbasi N. Chronic kidney disease prediction is an inexact science: The concept of "progressors" and "nonprogressors". World J Nephrol 2014;3(3):31-49.
3.D'Amico G. Influence of clinical and histological features on actuarial renal survival in adult patients with idiopathic IgA nephropathy, membranous nephropathy, and membranoproliferative glomerulonephritis: survey of the recent literature. Am J Kidney Dis 1992;20(4):315-23.
4.Johnston PA, Brown JS, Braumholtz DA, et al. Clinico-pathological correlations and long-term follow-up of 253 United Kingdom patients with IgA nephropathy. A report from the MRC Glomerulonephritis Registry. Q J Med 1992;84(304):619-27.
5. Li PK, Ho KK, Szeto CC, et al. Prognostic indicators of IgA nephropathy in the Chinese--clinical and pathological perspectives. Nephrol Dial Transplant 2002;17(1):64-9.
6. Cagnoli L. Instructions and implementations for percutaneous renal biopsy. Guidelines for the therapy of glomerular nephropaties. G Ital Nefrol 2003;20 Suppl 24:S3-47.
7. Jiang SH, Karpe KM, Talaulikar GS. Safety and predictors of complications of renal biopsy in the outpatient setting. Clin Nephrol 2011;76(6):464-9.
8. Parrish AE. Complications of percutaneous renal biopsy: a review of 37 years' experience. Clin Nephrol 1992;38(3):135-41.
9. Hu L, Wei L, Wang S, Fu C, Benker T, Zhao J. Better lesion conspicuity translates into improved prostate cancer detection: comparison of non-parallel-transmission-zoomed-DWI with conventional-DWI. Abdom Radiol (NY) 2021. doi:10.1007/s00261-021- 03268-5
10. Finsterbusch J. Improving the performance of diffusion-weighted inner field-of-view echo-planar imaging based on 2D-selective radiofrequency excitations by tilting the excitation plane. J Magn Reson Imaging 2012;35(4):984-92.
11. Jolly, M.-P., Guetter, C., Guehring, J., Cardiac segmentation in MR cine data using inverse consistent deformable registration, Proceedings/IEEE International Symposium on Biomedical Imaging: from nano to macro. IEEE International Symposium on Biomedical Imaging. January 2010. DOI: 10.1109/ISBI.2010.5490305
12. Kordbacheh H, Seethamraju RT, Weiland E, Kiefer B, Nickel MD, Chulroek T, et al. Image quality and diagnostic accuracy of complex-averaged high b value images in diffusion-weighted MRI of prostate cancer. Abdom Radiol (NY) 2019;44(6):2244-53.
Figures
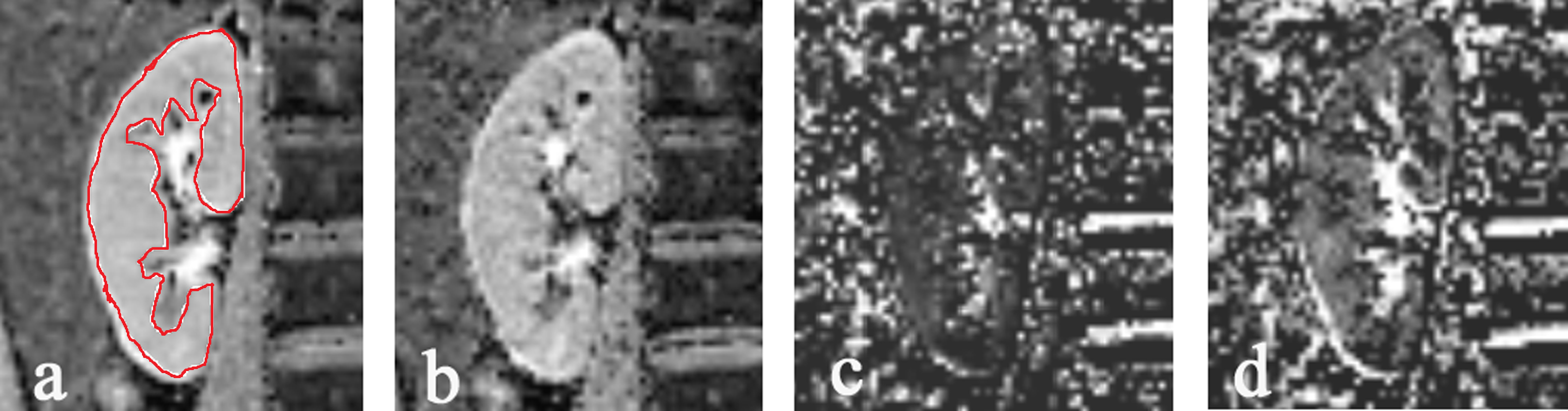
Fig 1. Representative images of diffusion-weighted imaging (DWI)-derived parameters, including (a) the apparent diffusion coefficient (ADC), (b) true diffusivity (D), (c) pseudo-diffusion coefficient (D*), and (d) perfusion fraction (f) maps. The region of interest (ROI) is marked in the renal parenchyma (cortex and medulla) in (a).
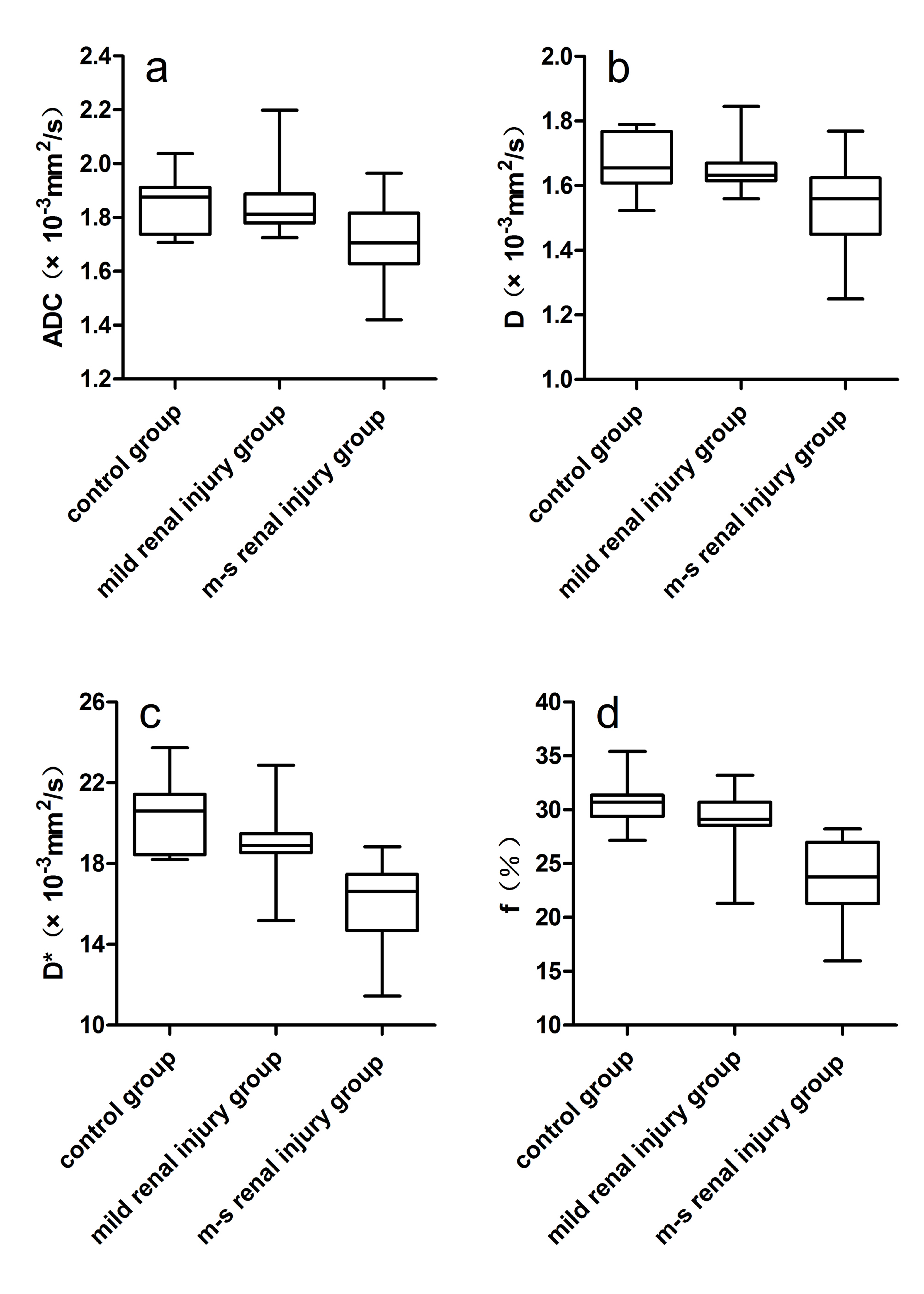
Fig 2. Box-and-whisker plots of the renal parenchymal the apparent diffusion coefficient (ADC) (a),true diffusivity (D) (b), pseudo-diffusion coefficient (D*) (c) and perfusion fraction (f) (d) values from the mild renal injury, moderate-severe renal injury, and control groups.
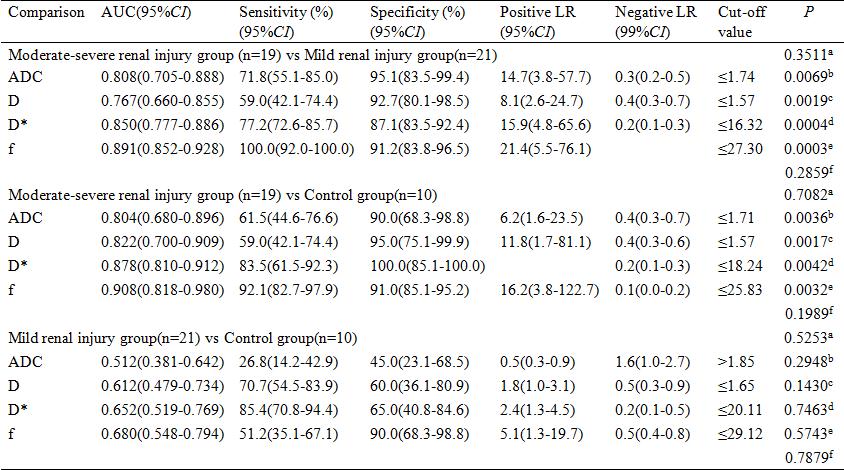
Table 1. Receiver operating characteristic (ROC) curve results for ADC and IVIM-derived parameters in differentiating among the three groups.