4659
Deep Learning Reconstruction for Abdomen Diagnosis: Improvement of Image Quality and Diagnostic Performance
Po-Ting Chen1,2, Cheng-Ya Yeh2, Yi-Chen Chen2, Chia-Wei Li3, Charng-Chyi Shieh3, Chien-Yuan Lin3, and Kao-Lang Liu1,2
1Department of Medical Imaging, National Taiwan University Hospital and National Taiwan University College of Medicine, Taipei, Taiwan, 2Department of Medical Imaging, National Taiwan University Cancer Center, Taipei, Taiwan, 3GE Healthcare, Taipei, Taiwan
1Department of Medical Imaging, National Taiwan University Hospital and National Taiwan University College of Medicine, Taipei, Taiwan, 2Department of Medical Imaging, National Taiwan University Cancer Center, Taipei, Taiwan, 3GE Healthcare, Taipei, Taiwan
Synopsis
There has been no study that demonstrated the quality improvement in abdomen images by DLrecon. We evaluate the image quality comparison, included SNR, CNR, and clinical scoring, between DL and non-DL abdomen images. DLrecon are found to be less artefacts, higher SNR, CNR, and clinical scores than those on non-DL images. This study proves the improvement of image quality by DLrecon, and DLrecon shows its potential power in clinical diagnosis of abdomen images to overcome classical MRI trade-off resolution, SNR, and scan time.
INTRODUCTION
In clinical settings, MRI with a 5-6 mm slice thickness is commonly used for abdomen imaging. Better spatial resolution can lead to better delineation of the lesion and its relationship with adjacent structures. However, higher spatial resolution would prolong the data acquisition time and lead to serious motion artefact, lower signal-to-noise ratio (SNR), contrast-to-noise ratio (CNR), and uncomfortable scanning [1-5]. Therefore, one method that can maintain or improve SNR while acquiring with better spatial resolution setting would greatly benefit the diagnosis in the rather complicated structure of abdominal region. Recent advances in deep learning (DL) reconstruction (DLrecon) for MRI have produced a myriad of trained neural networks capable of increasing the quality of diagnostic images. Moreover, DLrecon that makes more efficient use of the acquired data to produce sharp, high SNR images, would substantially benefit abdomen images acquisitions, adding more flexibility in protocol adjustments and enabling better leveraging of available acceleration techniques such as parallel and partial Fourier imaging. Yet no study has demonstrated the image quality improvement and clinical feasibility in abdominal region by DLrecon Therefore, this study aims to validate the improvement of MR abdomen image by DLrecon in terms of SNR, CNR, and clinical scoring.METHODS
Sixty-one participants (22 females) were enrolled retrospectively in this study. All the datasets including axial T2-weighted single-shot fast spin-echo (SSFSE) magnetic resonance cholangiopancreatography with/without fat-saturation were performed on a 3T clinical scanner (Signa Architect; GE Healthcare, Milwaukee, USA) equipped with an adaptive AIR™ Coil for signal detection and a whole-body coil for radio-frequency excitation. Those images were reconstructed by conventional pathway (non-DL) and by AIR™ Recon DL (DLrecon) process. The acquisition parameters for T2-weighted SSFSE images are: TR, 1622 ms; TE, 89 ms; flip angle, 90°; FOV, 29 cm; acquisition matrix, 256×256 (Reconstructed to 512×512); 32-36 slice thickness, 3.5 mm; NEX, 1.0; and bandwidth, 125 kHz. In the fat-saturated T2-weighted SSFSE images acquiring, the parameters are: TR, 1056 ms; TE, 82 ms; TI, 170 ms; flip angle, 90°; field of view, 32 cm; acquisition matrix, 324×288; reconstruction matrix, 512×512; slice thickness, 6.0 mm; NEX, 1.0; and bandwidth, 125 kHz. To compare the image quality of conventional MR images with images reconstructed by DLrecon technique, ROIs of pancreas (ball shape with 6-mm radius), liver (ball shape with 12-mm radius), and background noise (ball shape with 12-mm radius) were selected manually by two experienced radiology technologists, and the SNR and contrast-to-noise ratio (CNR) were assessed based on the signal intensity of those ROIs (Figure 1). The quality of images in clinical diagnosis in terms of perceived SNR, perceived sharpness, presence of artefacts, and overall quality is evaluated from one experienced radiologist by a 5-point score:1, very bad; 2, bad; 3, fair; 4, good; 5, very good.RESULTS and DISCUSSION
In Figure 2, Images by DLrecon showed higher SNR and less ringing artefact (as arrow indicated) than those by conventional reconstruction. In the result of SNR/CNR comparing, the images by DLrecon show significant enhanced SNR (39% and 61% of T2-weighted images with/without fat-saturation, respectively) and CNR (37% and 75% of T2-weighted images with/without fat-saturation, respectively) values than images by non-DL reconstruction (Figure 3). The same as the result of clinical-scores comparing, the 5 selected regions (Intrahepatic duct, bile duct, gall bladder, pancreas, spinal cord) in the images by DLrecon showed significantly better scores than that by non-DL reconstruction in the result of clinical scoring (Table 1).CONCLUSION
Compared with images by non-DL reconstruction, DLrecon images are found to be less artefacts, higher SNR and CNR as well as high clinical scores in routine T2-weighted SSFSE MRCP images with/without fat-saturation. Our finding proves the improvement of image quality by DLrecon, and DLrecon shows its potential power in clinical diagnosis of abdomen images. It may be possible to leverage DLrecon to overcome classical MRI trade-off resolution, SNR, and scan time.Acknowledgements
No acknowledgement found.References
- Chen, F., Taviani, V., Malkiel, I., Cheng, J. Y., Tamir, J. I., Shaikh, J., Chang, S. T., Hardy, C. J., Pauly, J. M., & Vasanawala, S. S. (2018). Variable-density single-shot fast spin-echo MRI with deep learning reconstruction by using variational networks. Radiology, 289(2), 366–373.2.
- Higaki, T., Nakamura, Y., Tatsugami, F., Nakaura, T., & Awai, K. (2019). Improvement of image quality at CT and MRI using deep learning. Japanese Journal of Radiology, 37(1), 73–80.3.
- Kim, M., Kim, H.S., Kim, H.J., Park, J.E., Park, S.Y., Kim, Y.H., Kim, S.J., Lee, J., Lebel, M.R. (2021), Thin-Slice Pituitary MRI with Deep Learning-based Reconstruction: Diagnostic Performance in a Postoperative Setting. Radiology. Jan;298(1):114-122.4.
- Litjens, G., Kooi, T., Bejnordi, B.E., Setio, A.A.A., Ciompi, F., Ghafoorian, M., van der Laak, J.A.W.M., van Ginneken, B., Sánchez, C.I. (2017), A survey on deep learning in medical image analysis, Med. Image Anal. 42, 60–88.
- van der Velde, N., Hassing, H.C., Bakker, B.J., Wielopolski, P.A., Lebel, R.M., Janich, M.A., Kardys, I., Budde, R.P.J., Hirsch, A. (2021), Improvement of late gadolinium enhancement image quality using a deep learning-based reconstruction algorithm and its influence on myocardial scar quantification. Eur Radiol. Jun;31(6):3846-3855.
Figures
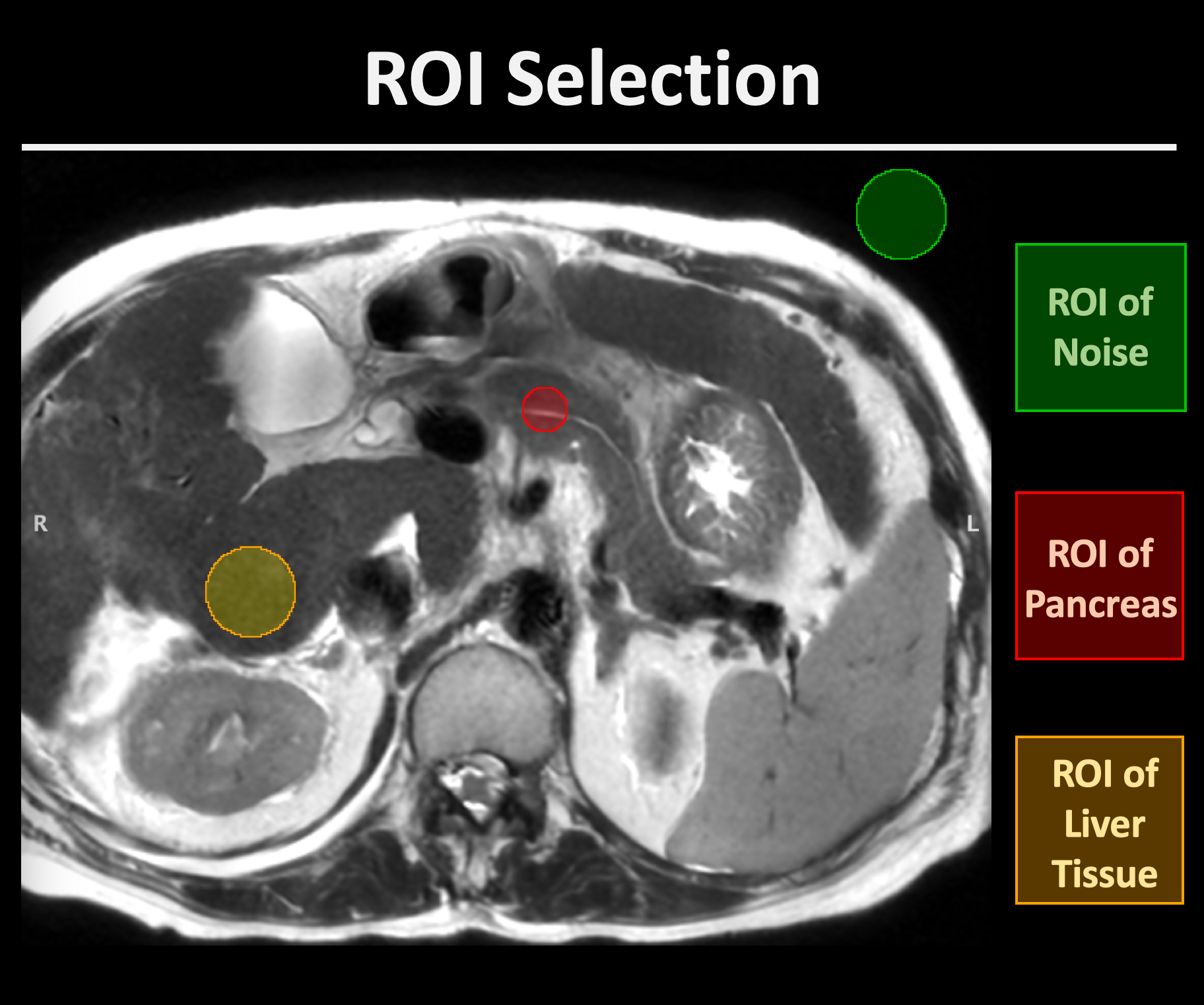
Figure 1. The ROIs selection for SNR and CNR calculation
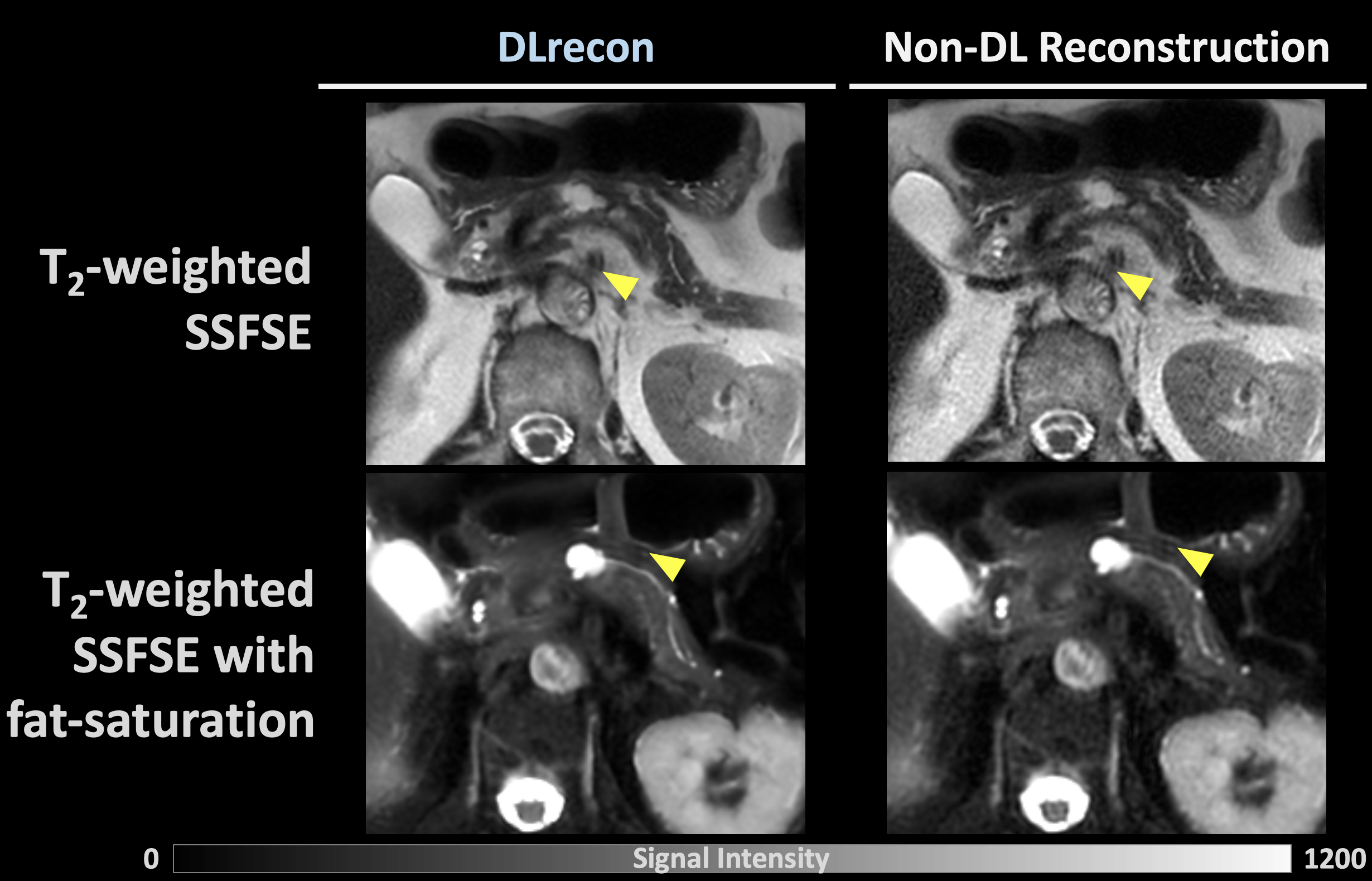
Figure 2. The representative images by DLrecon and non-DL reconstruction. The yellow arrows indicate the ringing artefact in the image by non-DL reconstruction but are almost absent in the images by DLrecon.
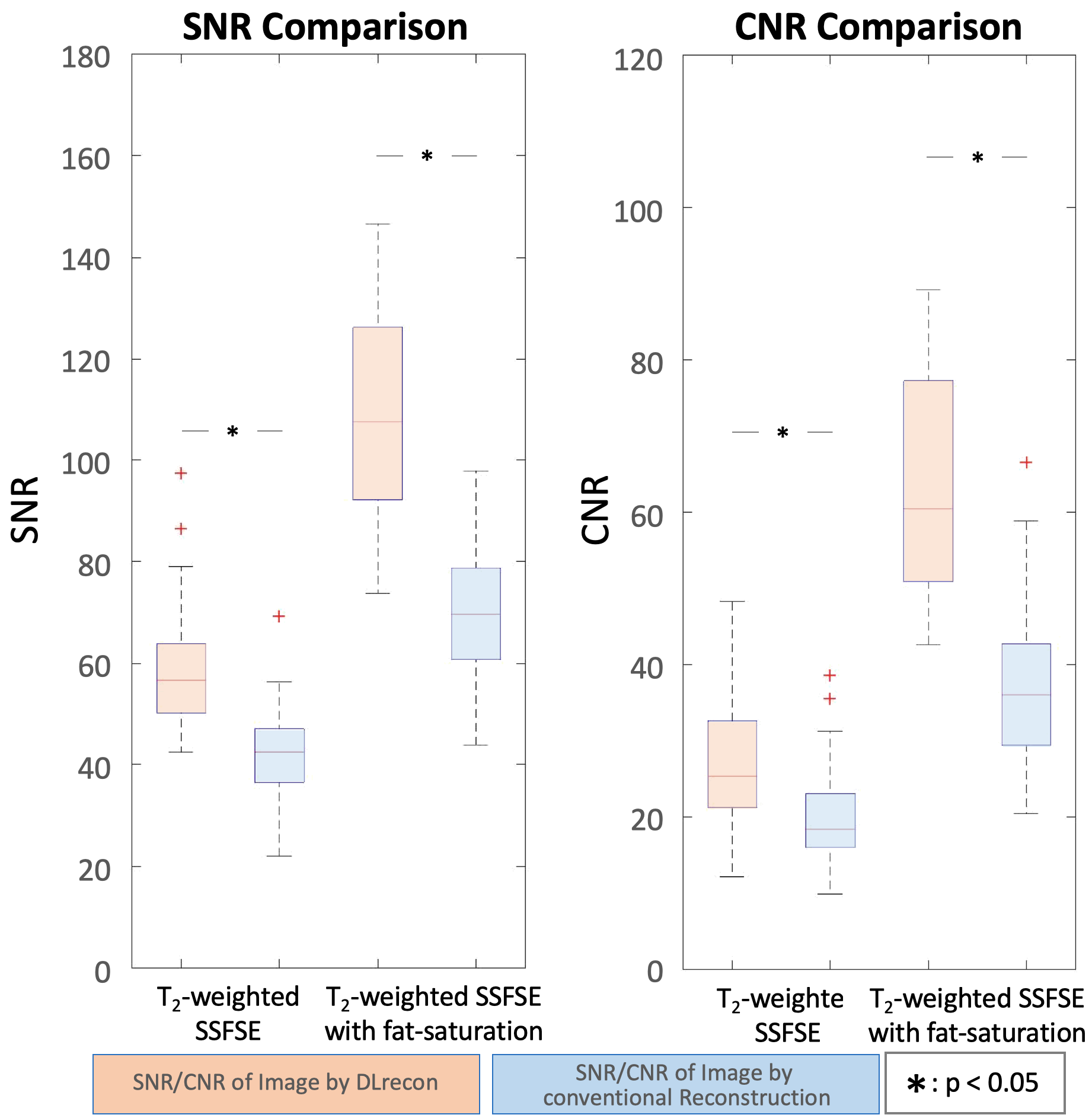
Figure 3. The comparing of SNR and CNR between DL and non-DL T2-weighted SSFSE MRCP images with/without fat-saturation.

Table 1. The comparing of clinical scores between images by DLrecon and conventional reconstruction in 5 selected regions.
DOI: https://doi.org/10.58530/2022/4659