4636
Quantitative assessment of bone erosion in patients with rheumatoid arthritis using ZTE-MRI1Biomedical Engineering College, Hubei University of Medicine, Shiyan Hubei, China, 2GE Healthcare, Beijing, China, 3Department of Radiology, Taihe Hospital, Hubei University of Medicine, Shiyan Hubei, China
Synopsis
MRI is reckoned as the most sensitive tool for monitoring changes such as synovitis and bone marrow edema at early stage of rheumatoid arthritis (RA)[1, 2]. Our results showed that ZTE-MRI can better precisely detect bone erosion compared with fs PD as well as DR and reflect RA degree via the volume percentage of bone erosion over carpal bone. Overall, ZTE-MRI could be an alternative to routine PDWI in clinic practice to help clinicians make better diagnosis without influenced by bone marrow edema, joint effusion and thickening of the synovial membrane and also offer articular function assessment as radiography.
Introduction
Rheumatoid arthritis (RA) is a systemic autoimmune disease associated with chronic synovial cell proliferation and inflammatory cell infiltration. Studies have shown that early treatment can effectively slow down the destruction of synovium, cartilage and bone[3, 4]. Digital radiography was prescribed to assess articular function based on Steinbrocker X-ray stage while bone erosion in RA patients is normally assessed based on Rheumatoid Arthritis Magnetic Resonance Image Score (RAMRIS)[5]. Bone erosion plays an important role in description of RA severity and prediction of disease progress[6]. However, previous studies have not focused on the quantitative evaluation but qualitative assessment. Although some studies indicated conventional T1-weighted imaging can be utilized to detect bone erosion, it has lower sensitivity to bone erosion than computed tomography [1, 2, 7] while a newly-emerged zero echo time MR imaging (ZTE-MRI) technique with the feature of capturing T2 relaxation time down to around has been shown to perform equivalently to CT[8, 9]. ZTE-MRI is a kind of PD-weighted imaging (PDWI) and its diagnosis performance on bone erosion and edema compared to conventional PD-weighted spin echo sequence has not been investigated. Therefore, we aimed to explore the feasibility of ZTE-MRI in quantitative assessment of RA degree.Materials and methods
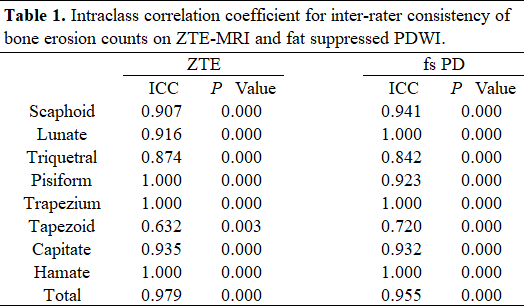
21 patients who conform to the American College of Rheumatism (ACR) classification were recruited in this study. On the same day, all patients underwent digital radiography and MRI examination including fat saturation proton density-weighted (fs PD) imaging and ZTE-MR imaging (Field of view, slice thickness, slice gap, and resolution were set the same). Two physicians graded RA degree on plain radiographs according to Steinbrocker radiographic stage [10], count the number of bone erosion on fs PD and ZTE images, and calculate the bone erosion proportion of bone erosion volume to the whole carpal volume on ZTE images. Bone erosion was defined as bone destruction with clear edges. Intraclass correlation coefficient (ICC) was used to test inter-rater and intra-modality consistency. Bone erosion counts and bone erosion volume ratio between sequences were analyzed by paired T-test or nonparametric Wilcoxon sign rank test depending on normal distribution. Spearman rank correlation test was used to calculate the correlation between bone erosion percentage and different grades.Results
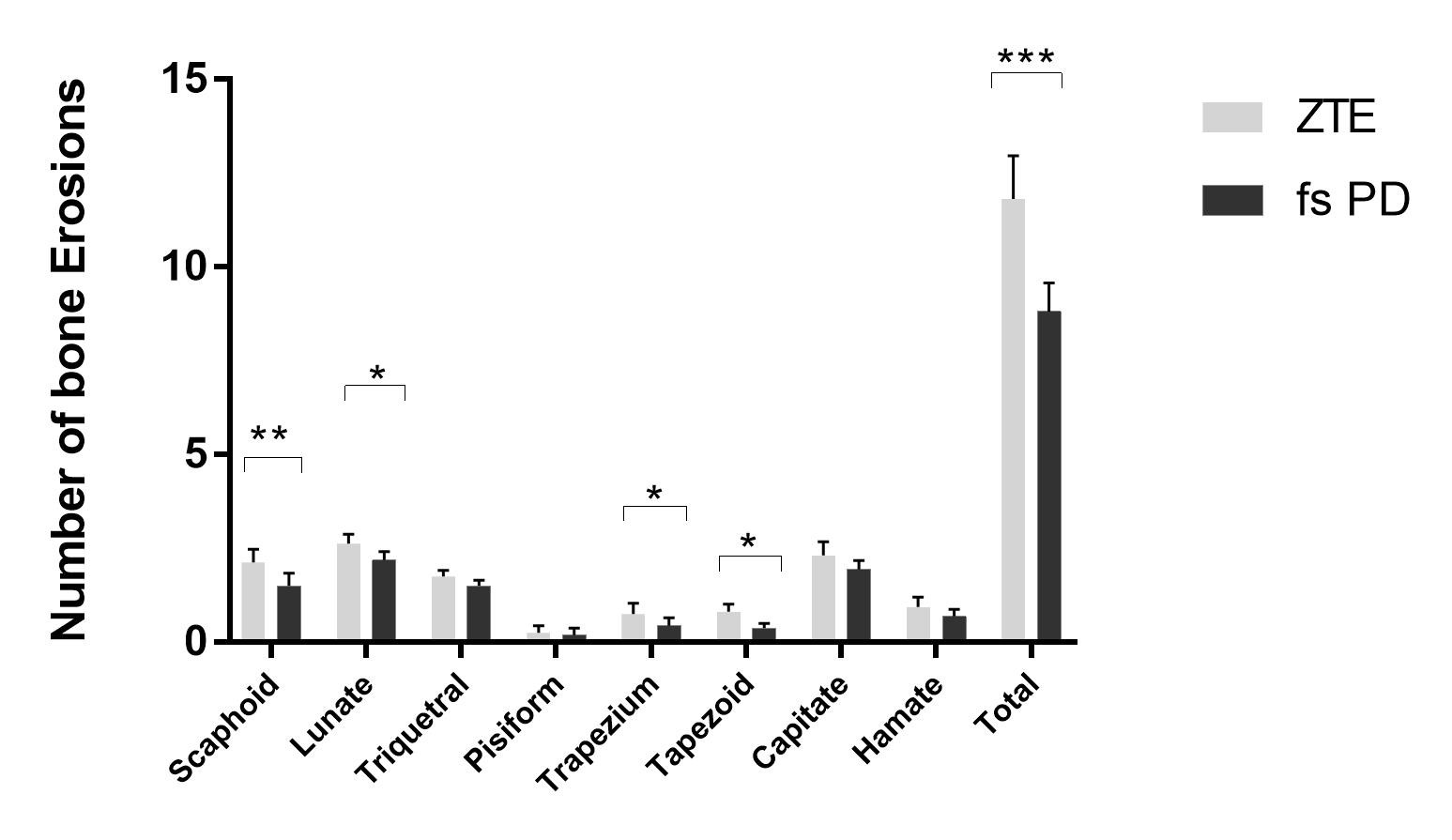
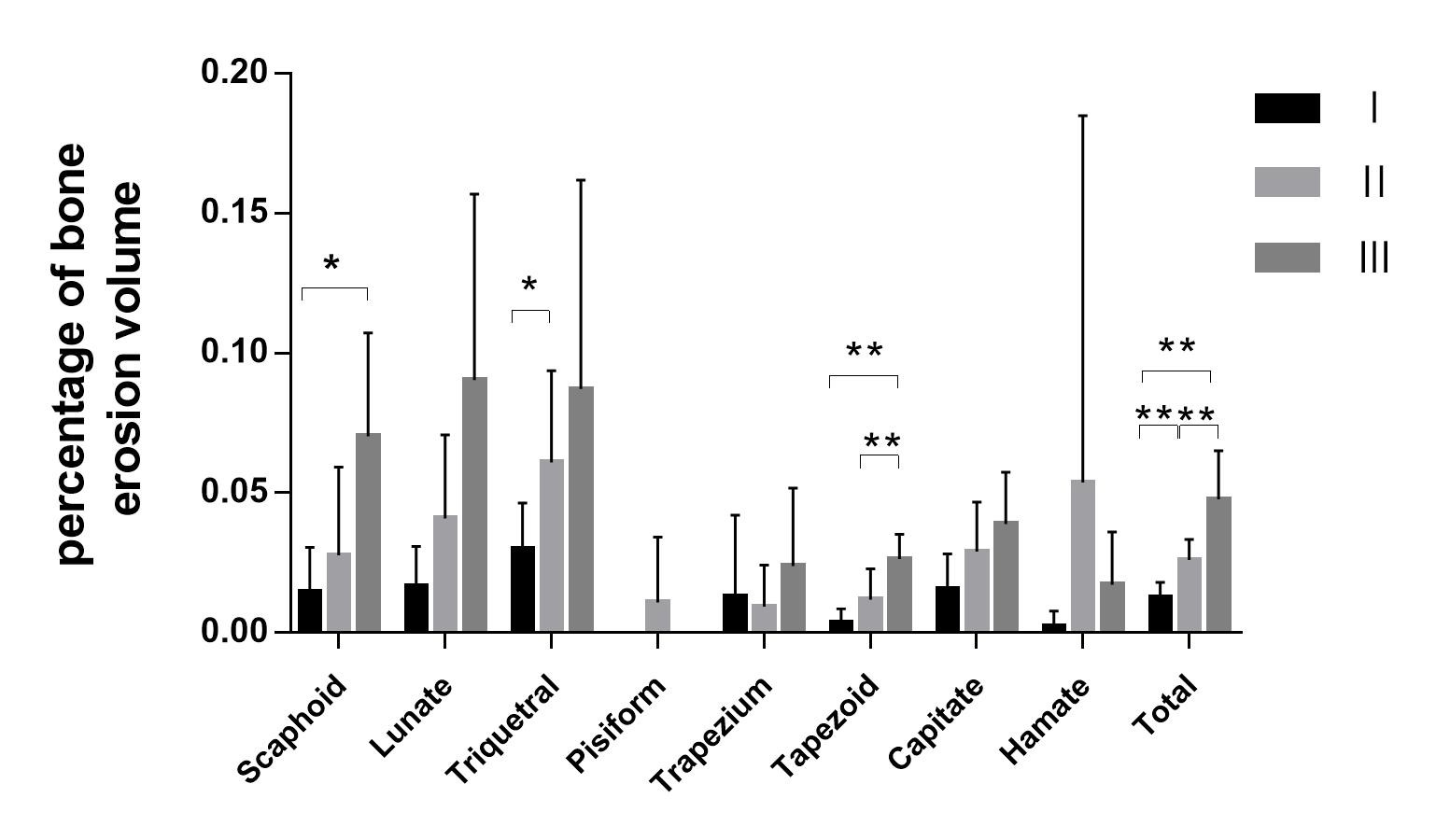
The number of bone erosion counted by two physicians showed good to excellent consistency on both ZTE-MRI and fs PD [ICC= (0.874-1.000), (0.720-1.000), p < 0.001) (Table 1). ZTE-MRI and fs PD showed significantly different number of bone erosion (p < 0.001) (Figure 1). The proportion of bone erosion in RA patients increased with Steinbrocker X-ray stage (Spearman's rho=0.875,P=0.000). Moreover, there were statistically significant differences in the proportion of bone erosion between each two subgroups as Steinbrocker X-ray stage I, II and III (p < 0.01) (Figure 2). For occurrence of bone erosion, scaphoid, lunate and triangular bone mostly initiated.Discussion
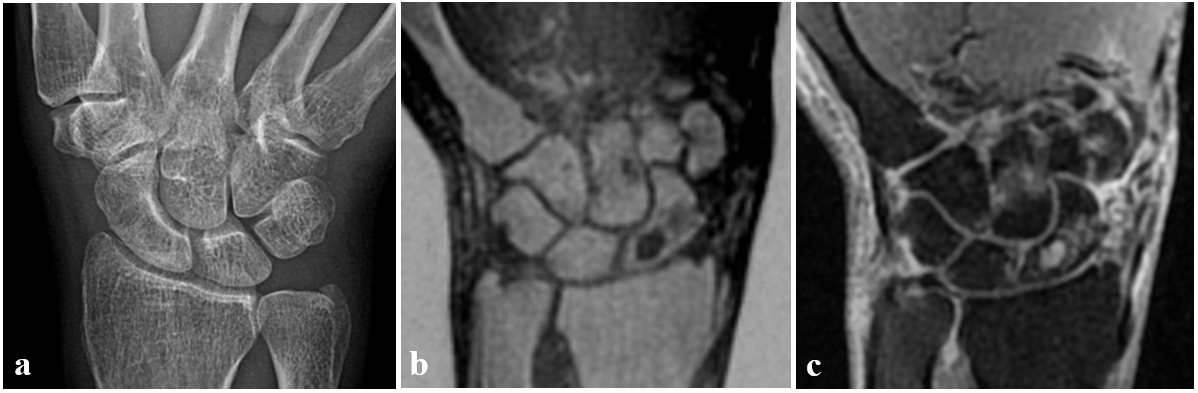
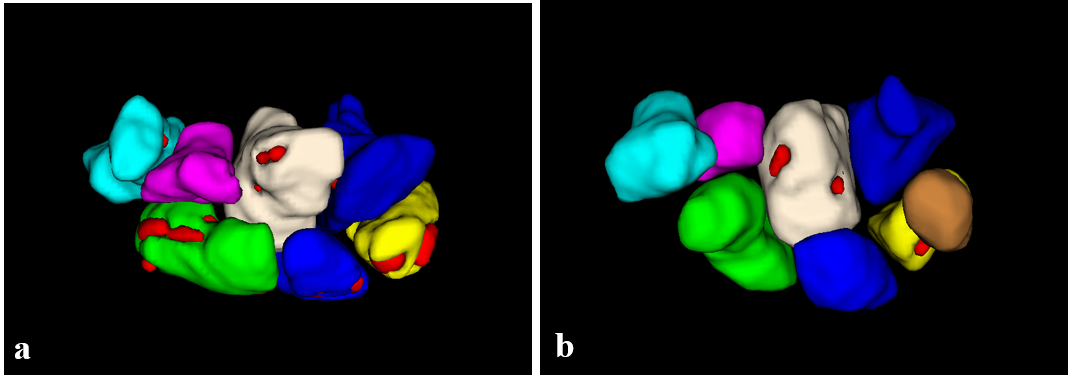
In our study, ZTE-MRI clearly delineated the boundary of bone erosion and provided finer and clearer images even with the presence of bone marrow edema, joint effusion and thickening of the synovial membrane than conventional fs PDWI (Figure 3). These image characteristics on conventional fs PDWI with the same imaging parameters (resolution and slice gap) appeared moderate to relatively high signal and presented the blurred edge of erosion and enlarged erosion size due to partial volume effect. Although plain radiographs were commonly used to assess articular function for RA patients, bone erosion could hardly be seen on plain radiographs due to low specificity and thus early erosion detection would be easily missing on plain radiographs. Compared to DR, radiation-free MRI, in particular ZTE-MRI, was relatively sensitive to bone erosion and edema and offer good image quality to differentiate inflammatory lesions from surrounding tissues and to elevate accuracy of quantifying proportion of bone erosion via sketching volume of interests instead of visual assessment (Figure 4). With better conspicuity of bone erosion on ZTE-MRI, volume of bone erosion and percentage of bone erosion volume to the whole carpal volume were measured and quantitatively reflect RA degree for patients instead of qualitative assessment by Steinbrocker X-ray stage. scaphoid, lunate and triangular bone were the incidence of bone erosion in order in our study, suggesting orthopedists should pay more attention to these three sites when only DR was prescribed to yet-to-confirmed RA patients. Moreover, ZTE-MRI can provide not only structural abnormalities (e.g. edema and erosion) but also functional evaluation (i.e., erosion volume positively correlated with articular function based on Steinbrocker X-ray stage) with higher sensitivity and specificity than convectional PDWI and DR .Conclusions
Overall, ZTE-MRI could be an alternative to routine PDWI in clinic practice to help clinicians make better diagnosis without influenced by bone marrow edema, joint effusion and thickening of the synovial membrane and also offer articular function assessment.Acknowledgements
No acknowledgement found.References
1. da Mota LM, Cruz BA, Brenol CV, Pereira IA, Fronza LS, Bertolo MB, et al. 2011 Consensus of the Brazilian Society of Rheumatology for diagnosis and early assessment of rheumatoid arthritis. Rev Bras Reumatol 2011; 51(3):199-219.
2. Hodkinson B, Van Duuren E, Pettipher C, Kalla A. South African recommendations for the management of rheumatoid arthritis: an algorithm for the standard of care in 2013. S Afr Med J 2013; 103(8 Pt 2):576-585.
3. Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet 2016; 388(10055):2023-2038.
4. Barile A, Arrigoni F, Bruno F, Guglielmi G, Zappia M, Reginelli A, et al. Computed Tomography and MR Imaging in Rheumatoid Arthritis. Radiol Clin North Am 2017; 55(5):997-1007.
5. Østergaard M, Peterfy C, Conaghan P, McQueen F, Bird P, Ejbjerg B, et al. OMERACT Rheumatoid Arthritis Magnetic Resonance Imaging Studies. Core set of MRI acquisitions, joint pathology definitions, and the OMERACT RA-MRI scoring system. J Rheumatol 2003; 30(6):1385-1386.
6. Malla S, Vyas S, Bhalla AS, Kumar U, Kumar S, Gupta AK. Ultrasonography in Early Rheumatoid Arthritis of Hand and Wrist Joints: Comparison with Magnetic Resonance Imaging. Indian J Orthop 2020; 54(5):695-703.
7. Lee CH, Srikhum W, Burghardt AJ, Virayavanich W, Imboden JB, Link TM, et al. Correlation of structural abnormalities of the wrist and metacarpophalangeal joints evaluated by high-resolution peripheral quantitative computed tomography, 3 Tesla magnetic resonance imaging and conventional radiographs in rheumatoid arthritis. Int J Rheum Dis 2015; 18(6):628-639.
8. W.Y. Liu H.T.Wu, C.E. Lin, H.L. Lee, W.Y. Guo Evaluation of the Condyle Position and Volume in the Temporomandibular Joint Using Zero Echo Time MRI. In: Annual Meeting of the International Society for Magnetic Resonance in Medicine (ISMRM) May 2018.
9. Y. Li SH, W.V. Liu, X. Li Diagnostic performance of zero echo time imaging and T1-weighted fast spin echo on sacroiliac joint bone erosions using CT as the gold standard. . Annual Meeting of the International Society for Magnetic Resonance in Medicine (ISMRM) May 2020.
10. Steinbrocker O, Traeger, C. H. & Batterman, R. C. Terapeutic criteria in rheumatoid arthritis. J Am Med Assoc 1949; 140:659–662
Figures