4631
Application of Multi-echo DIXON and HISTO to evaluate bone marrow fat/iron content in lumbar osteoporosis patients1Department of Radiology, Tianjin Medical University General Hospital, Tianjin, China, 2MR Scientific Marketing, Siemens Healthineers, Beijing, China
Synopsis
Our study investigated the feasibility of LiverLab technique, consisted of multi-echo DIXON and HISTO, to evaluate the vertebral BMFF and iron content for the diagnosis of osteoporosis. BMFF measured by multi-echo DIXON and HISTO was significantly increased in osteoporosis patients and strong negative correlation with BMD. Vertebral iron content had no difference in osteoporosis patients and no correlation with BMD. LiverLab technique, composed of multi-echo DIXON and HISTO, can quantitatively evaluate the changes in bone marrow fat content, and can be used as a potential biomarker for evaluating abnormal bone density and severity of osteoporosis.
Introduction
Osteoporosis is a disease characterized by reduced bone mineral density (BMD). Recent studies have found that MRI has the ability to monitor the amount of bone marrow fat and showed a reliable correlation with BMD by using single-echo magnetic resonance spectroscopy (1H-MRS)1. However, the difference in T2-relaxation between water and fat at different TE causes a bias in the quantification of bone marrow fat fraction (BMFF). In addition, many clinical observations suggest the iron overload is related to osteoporosis2. The LiverLab technique can be used for precisely quantitative analysis of fat and iron content in the liver lesion simultaneously, and consists of multi-echo DIXON and HISTO sequences. In order to overcome the bias as well as evaluate BMFF and iron content in the diagnosis of osteoporosis, we used LiverLab technique to measure the BMFF and iron content in L1-L4 vertebra and compared them with corresponding BMD measured by Dual energy X-ray absorptiometry (DXA).Methods
The study was approved by the local Institutional Review Board. All participants have written informed consent before each examination. 10 people (2 males and 8 females; age 61.9 ± 9.9) were recruited for this study. All the participants underwent examinations on a 3T MR scanner (MAGNETOM Skyra, Siemens Healthineers, Erlangen, Germany). The demographic information is summarized in Table 1. The sagittal multi-echo DIXON sequence was used for fat quantification with the following parameters: TE =1.1, 2.5, 3.7, 4.9, 6.2 and 7.4 ms; TR = 9.2 ms; slice thickness = 4.0 mm; flip angle = 4°; matrix size = 109×160; and FOV = 327×261mm2. BMFF map was calculated by using a multi-step adaptive fitting algorithm3. The sagittal HISTO sequence was used for fat and iron quantification with the following parameters: TE =12, 24, 36, 48 and 72ms; TR = 3000 ms; voxel = 15×15×15 mm3. BMFF and R2water map were calculated by using peak fitting of every TE to correct the T2 decay of each component4. BMD of L1-4 vertebra was measured with DXA. Based on the DXA values, the participants were divided into normal, osteopenia and osteoporosis group. The BMFF and R2water were compared among the three groups using one-way analysis of variance. The SNK-q method was used to compare the significant difference between any two groups. Linear correlation was performed using the Pearson correlation to evaluate the relationship between BMFF measured by DIXON and HISTO, BMFF measured by DIXON and BMD, BMFF measured by HISTO and BMD as well as R2water and BMD.Results
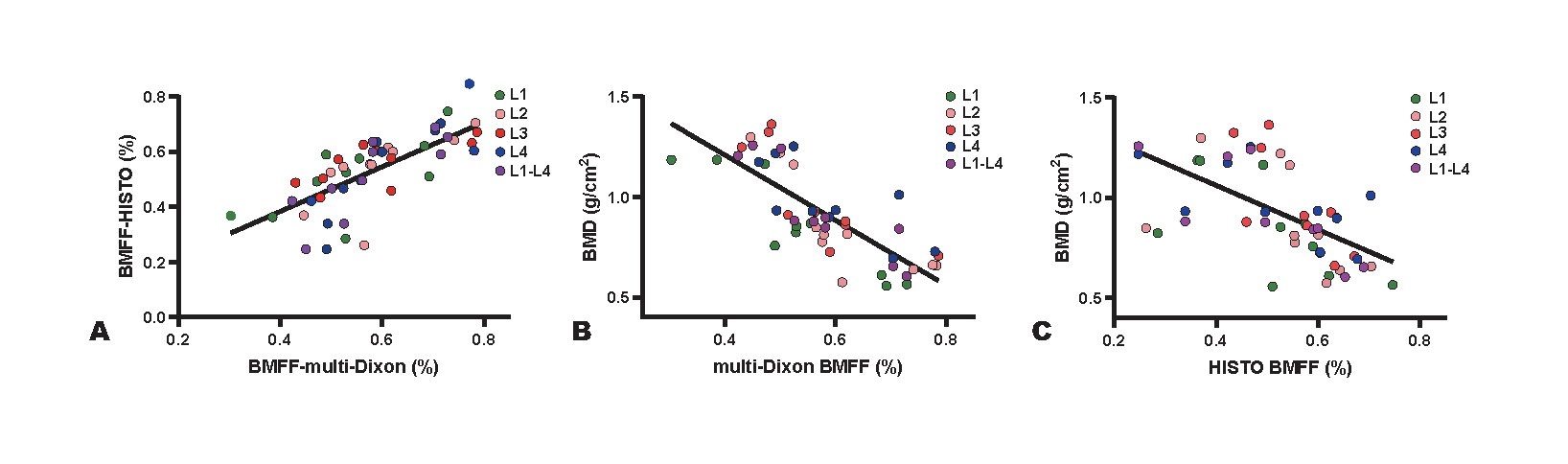
According to the BMD measured by DXA, there were 3 participants with normal bone density, 4 with osteopenia and 3 with osteoporosis. A significant difference (P < 0.05) existed in the BMD measured by DXA and BMFF measured by multi-echo DIXON in any vertebra among the three groups (Table 2). The post hoc test demonstrated that BMFF measured by multi-echo DIXON had significant differences between normal and osteopenia, normal and osteoporosis, osteopenia and osteoporosis. The BMFF of L1 and L2 had no difference (P> 0.05), while the BMFF of L3, L4 and L1-L4 had significant differences among the three groups measured by HISTO (P <0.05). The post hoc test shown that there was significant difference in BMFF measured by HISTO between normal and osteoporosis. The BMFF was lower in the normal group than the osteopenia and osteoporosis group. The BMFF measured by multi-echo DIXON was greater than that measured by HISTO (55.83% ± 4.08 vs 51.55% ± 11.88, P = 0.190 in osteopenia, 71.59% ± 6.49 vs 64.23% ± 5.95, P = 0.007 in osteoporosis). No difference existed (P > 0.05) in the R2water in any vertebra among the three groups (Table 2). A strong positive correlation was found between BMFF measured by multi-echo DIXON and that measured by HISTO (r = 0.721, P < 0.001) (Figure 1). There was a significant negative correlation between BMFF measured by multi-echo DIXON and BMD (r = -0.786, P < 0.001) as well as BMFF measured by HISTO and BMD (r = -0.591, P < 0.001) (Figure 1). There is no correlation between R2water and BMD.Discussion
We investigated the feasibility of LiverLab technique to evaluate the vertebral BMFF and iron content by multi-echo DIXON and HISTO for the diagnosis of osteoporosis. Our results suggest that BMFF measured by multi-echo DIXON and HISTO both can be used to identify osteopenia and osteoporosis. No difference and correlation existed between vertebral iron content and BMD. Multi-echo DIXON and HISTO are fast quantitative method and easily performed in routine spine examination, allowing BMFF measurement and determining further examination and treatment. However, the study sample size was small, limiting the study quality. Further a larger sample size is needed to corroborate our findings.Conclusions
Multi-echo DIXON and HISTO in MRI as effective and nonionizing methods to access vertebral BMFF have potential value to reflect bone density. It can be used as a tool for detecting osteoporosis in clinical practice.Acknowledgements
We thank the all participants in this study.References
1. Ann V Schwartz, Sigurdur Sigurdsson, Trisha F Hue, et al. Vertebral bone marrow fat associated with lower trabecular BMD and prevalent vertebral fracture in older adults. J Clin Endocrinol Metab, 2013. 98(6):2294-300.
2. G F Li, Y Z Pan, P Sirois, et al. Iron homeostasis in osteoporosis and its clinical implications. Osteoporos, 2012. 23(10):2403-8.
3. Zhong X, Nickel MD, Kannengiesser SA, et al. Liver fat quantification using a multi-step adaptive fitting approach with multi-echo GRE imaging. Magn Reson Med 2014; 72:1353.
4. Pineda N, Sharma P, Xu Q, et al. Measurement of hepatic lipid: high-speed T2-corrected multiecho acquisition at 1H MR spectroscopy--a rapid and accurate technique. Radiology. 2009; 252:568.
Figures
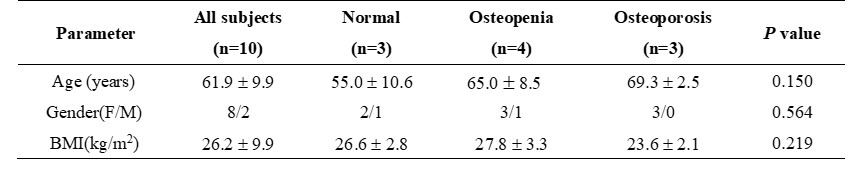
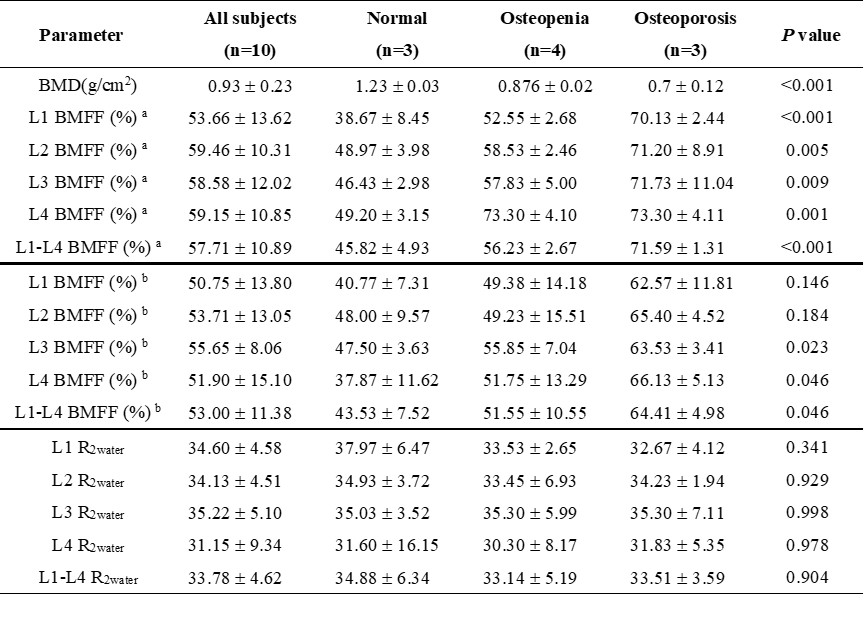
Table 2. Comparison of BMD measured by DXA, BMFF measured by multi-echo DIXON and HISTO, R2water measured by HISTO between normal, osteopenia and osteoporosis group. Plus-minus values are means ± SD. a BMFF measured by multi-echo DIXON. b BMFF measured by HISTO