4627
AI-assisted compressed sensing (ACS) in accelerating knee MR imaging: A pilot study in adults1Department of Radiology, west China hospital of Sichuan University, Chengdu, China, 2west China hospital of Sichuan University, Chengdu, China, 3MR Collaboration, Central Research Institute, United Imaging Healthcare, Shanghai, China
Synopsis
In knee MRI, patients with pain or limited motion can have difficult to endure a long-time imaging position. At the same time, the relatively high spatial resolution and good image quality were required in such musculoskeletal MRI. Therefore, shortening scan time and improving the image quality is the aim of current knee MRI.Our study compared conventional parallel imaging (PI) and artificial intelligence assisted compressed sensing (ACS) in terms of imaging quality and diagnostic performance in knee MRI, and achieved a 5-minute comprehensive examination of the knee, without compromising either image quality or visualization of anatomical and pathological structures.
Introduction
Approximately 25% of adults are suffering knee pain which is limiting the knee function and impairing the quality of life[1], and the prevalence of knee pain has increased almost 65% over the past 20 years[2]. Due to the excellent soft tissue contrast and high spatial resolution, magnetic resonance imaging (MRI) examination has become to the imaging gold standard for noninvasive and radiation-free evaluation of knee injuries and abnormalities[3]. Routine clinical knee MRI protocols which usually include fast spin-echo (FSE) sequences with T1, T2, or proton density (PD) weighted sequences with or without fat saturation (FS) may need at least 15 to 20 minutes [4]. Thus, when the scan time is long, patients with knee pain tend to move, which may bring motion artifacts and increase the risk of reduced image quality. Therefore, rapid MRI data acquisition is essential in clinical knee imaging. Recently, there has been interested in using deep learning (DL) to accelerate MR acquisition and reconstruction which could overcome the tradeoff between scan time and image quality of conventional sequence and reduce the noise level. The aim of this prospective study was to explore the value of ACS sequence in clinical routine examination and compare the performance of 5-mintute ACS-based knee sequences with conventional PI sequences in terms of image quality and diagnostic accuracy.Methods
Knee MRI of 18 healthy volunteers (male: female, 3:15; mean age, 26.78 ± 3.86 years) with 35 knees and 35 patients (male: female, 14:21; mean age, 43.97 ± 10.97 years) with 66 symptomatic knees were acquired randomly using conventional PI and artificial intelligence (AI) assisted compressed sensing (ACS) sequences (sagittal fast spin echo (FSE) T1-weighted images (T1WI), coronary FSE proton density-weighted (PDWI) and FSE T2-weighted images (T2WI) in both sagittal and transverse planes). A board-certified fellowship-trained musculoskeletal radiologist with 2 years of subspecialty experience drew regions of interest (ROIs) on the same slice of conventional PI- and ACS-MRI. The ROIs were drawn on grossly normal bone, muscle, cartilage, and meniscus. Objective image quality was assessed by signal-to-noise ratios (SNRs) and contrast-to-noise ratios (CNRs). For subjective image quality, motion artifacts and overall image impression were evaluated using a five-point scale by two radiologists. For diagnostic performance, the same two radiologists independently evaluated the menisci, ligaments abnormalities using a four-point scale, evaluated cartilage and subchondral bone marrow abnormalities using a four-point scale.Results
The total scan time was reduced from 8:02 to 4:50 min with ACS (39.8% reduction) (-56s, 34.6% reduction in sag T2WI, -32s, 39.5% reduction in sag T1WI, -40s, 36.4% reduction in cor PDWI, -64s, 49.6% reduction in tra T2WI). SNRs of bone, muscle, cartilage, and meniscus in ACS images were significantly higher than those in PI images (p < 0.05) (figure1). Moreover, CNRs of ACS sequences were higher than those of PI images (p < 0.05, excepting bone-cartilage in sagittal T2W images) (figure2). For qualitative image quality (figure3), with a good inter-observer agreement, ACS sequences reduced motion artifacts and increased overall image quality compared with conventional PI sequences except in T1WI images. And the inter-method and inter-reader agreements between PI and ACS images were good or excellent.Discussion
In the past few years, there were various CNN method proposed to reconstruct the knee images, such as variational network (VN)[5], the model-based dee-learning architecture (MoDL)[6], and deep density priors (DDP)[7]. In our research, the AI module in ACS aims to mitigate reconstruction artifacts from conventional methods especially at higher acceleration level and make the final results closer to the image, additionally, without sacrifice of fidelity to the information of the collected data. This AI module is trained based on the designed residual network (Resnet)[8, 9] which is widely used in mainstream CNN, for example, SRRESNET[10], Pix2pix[11], which can solve the problem of gradient disappearance, ensure the convergence of the network and improve the reconstruction performance. In recent years, the individual knee sequences trained by specialized DL reconstruction models to accelerate the acquisition velocity and obtain image quality enhancement[5, 12]. For multi-sequence training on clinical knee MRI routine protocol, Recht’s study demonstrated the comparable image quality and diagnostic interchangeability of the DL-assisted knee MR acceleration [12] by using retrospective undersampling data. Different with the above researches, our knee protocol involved four separate scans and collected in three different plane orientations, procuring multiple image contrast and different viewing. Moreover, our networks perform on prospectively undersampled data which may be more conducive to study the reliability of the AI module.Acknowledgements
We thank the Department of Radiology at West China Hospital. We also thank all the patients and their families for participation and cooperation in our study.References
1. Bunt, C.W., C.E. Jonas, and J.G. Chang, Knee Pain in Adults and Adolescents: The Initial Evaluation. (1532-0650 (Electronic)).
2. Nguyen, U.S., et al., Increasing prevalence of knee pain and symptomatic knee osteoarthritis: survey and cohort data. (1539-3704 (Electronic)).
3. Committee, C.S., ACR – SSR PRACTICE GUIDELINE FOR THE PERFORMANCE AND INTERPRETATION OF MAGNETIC RESONANCE IMAGING ( MRI ) OF THE SHOULDER. 2010.
4. Matcuk, G.R., et al., Compressed Sensing MR Imaging (CS-MRI) of the Knee: Assessment of Quality, Inter-reader Agreement, and Acquisition Time. (1880-2206 (Electronic)).
5. Hammernik, K., et al., Learning a variational network for reconstruction of accelerated MRI data. (1522-2594 (Electronic)).
6. Liu, F., et al., High-performance rapid MR parameter mapping using model-based deep adversarial learning. (1873-5894 (Electronic)).
7. Tezcan Kc Fau - Baumgartner, C.F., et al., MR Image Reconstruction Using Deep Density Priors. (1558-254X (Electronic)).
8. Lu, T., et al., pFISTA-SENSE-ResNet for parallel MRI reconstruction. (1096-0856 (Electronic)).
9. Fu, Z., et al., A multi-scale residual network for accelerated radial MR parameter mapping. (1873-5894 (Electronic)).
10. Ledig, C., et al. Photo-Realistic Single Image Super-Resolution Using a Generative Adversarial Network. in IEEE Computer Society. 2016.
11. Isola, P., et al. Image-to-Image Translation with Conditional Adversarial Networks. in IEEE Conference on Computer Vision & Pattern Recognition. 2016.
12. Hyun, C.M., et al., Deep learning for undersampled MRI reconstruction. (1361-6560 (Electronic)).
Figures
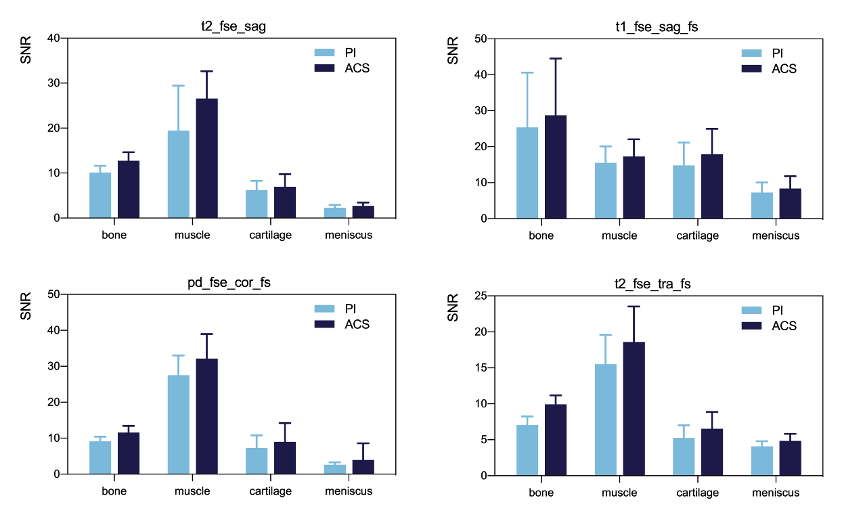
Figure 1. Statistical analysis of SNRs between PI and ACS knee sequences on original images.
The SNRs in ACS images were significantly higher than in conventional PI images. All P< 0.05.
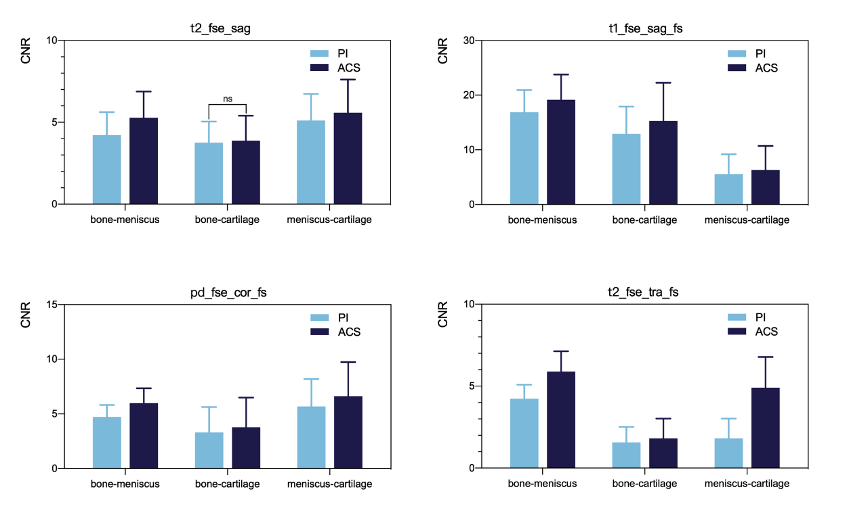
Figure 2. Statistical analysis of CNRs between PI and ACS knee sequences on original images.
The CNRs in ACS images were significantly higher than in conventional PI images (P< 0.05) except CNR of bone-cartilage (P=0.303).
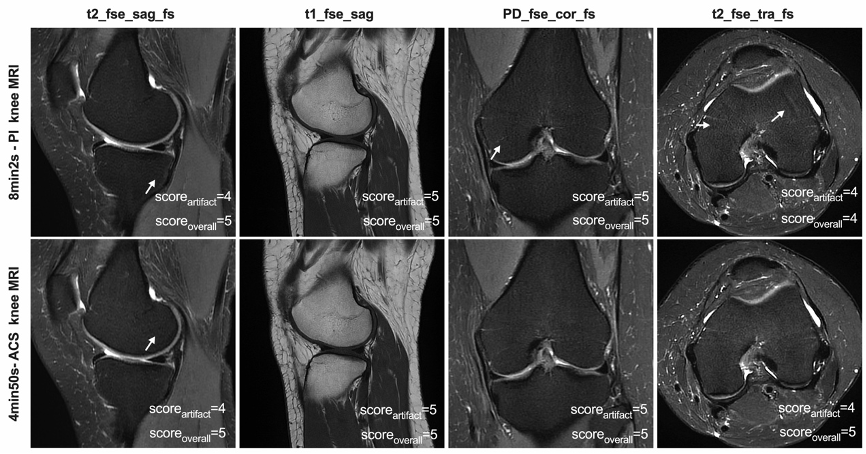
Figure 3. Example of image quality analysis in a 28-year-old female volunteer.ACS sequences reduces motion artifacts and increases overall image quality compared with conventional PI sequences. Except in T1WI images.
Soreartifact: score of motion artifacts; scoreoverall: score of overall image quality.
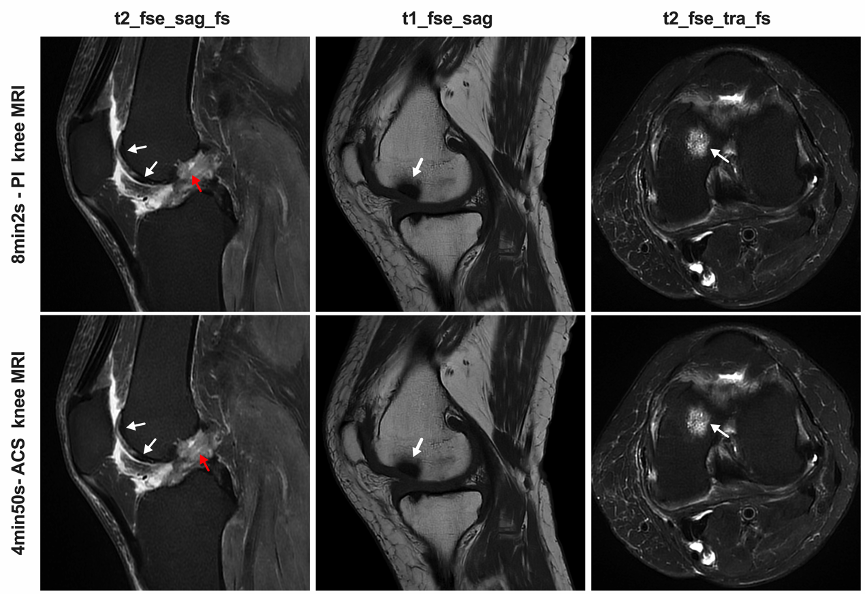
Figure 4 Left knee magnetic resonance images of a 59-year-old woman with a history of knee pain (osteoarthritis).
Demonstrated the LCF cartilage defects (white arrows in sag T2WI, scored 2/2), LFC edema (red arrows in sag T2WI, scored 3/3) and MCF subchondral bone marrow lesion (white arrows in sag T1WI and tra T2, scored 1/1).
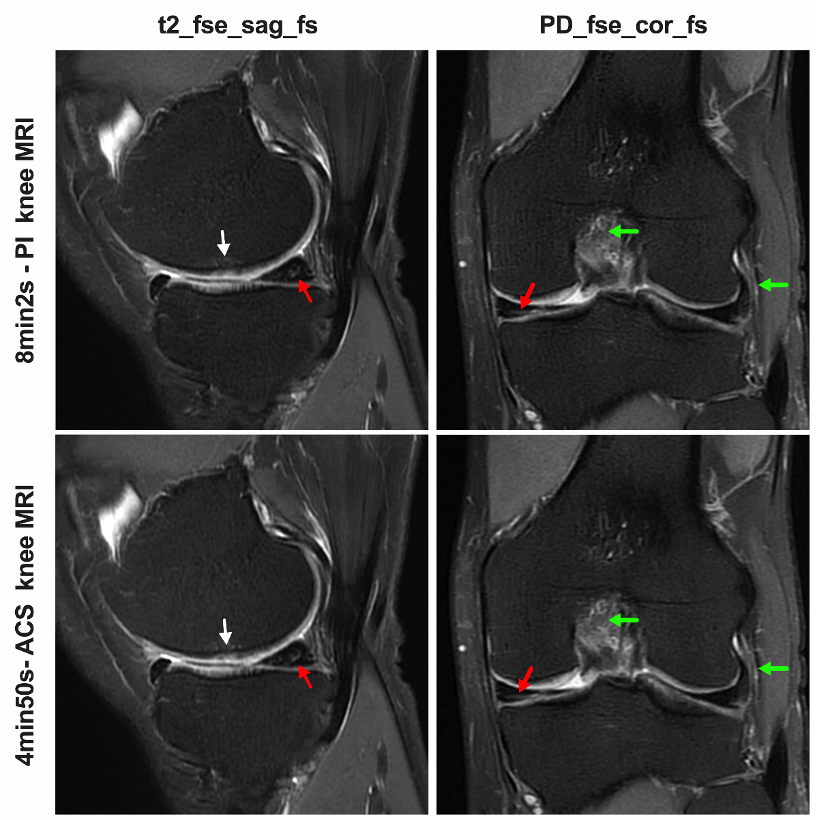
Figure 5 Left knee magnetic resonance images of a 59-year-old man with a history of knee pain (meniscus tear).
Demonstrated the MM meniscus tears (red arrows in sag T2WI and cor PD, scored 3/3), LFC edema (green arrows in cor PD, scored 3/3); LCL edema (green arrows in cor PD, scored 2/2).