4621
Can infrapatellar fat pad predict the incidence of knee osteoarthritis by using deep learning based on MRI? Data from osteoarthritis initiative1Department of Medical Imaging, The Third Affiliated Hospital of Southern Medical University, Guangzhou, China, 2Department of Radiology, Peking University Shenzhen Hospital, Shenzhen, China, 3Department of Computer Science & Engineering, The Chinese University of Hong Kong, Hong Kong, China
Synopsis
Infrapatellar fat pad (IPFP) is an important risk factor for the incident of radiographic knee osteoarthritis (iROA)1, 2. However, the potential of being an independent biomarker to predict iROA is untapped. Deep learning (DL) is a set of algorithms that enable computers to discover complicated patterns in large data sets3. In this study, we train a DL model to predict iROA with auto-segmented IPFP, comparing it to the DL model set up with corresponding whole knee MR images (MRI). The results reveal that IPFP alteration can predict iROA independently comparably to the whole knee MRI at one year before iROA.
Purpose and Introduction
IPFP is an intra-articular adipose tissue that secretes a variety of inflammation factors to induce a local knee inflammatory state, which is recognized as a major risk factor for knee osteoarthritis (KOA) onset1, 4. Previous studies found the signal intensity alteration of IPFP closely associated with the incident of radiographic KOA (iROA)1, 2, 5. Deep learning (DL) is the state-of-the-art technology that enables computers to discover complicated patterns in large data sets with a convolutional neural network (CNN). We aim at evaluating whether IPFP alteration can serve as an independent biomarker to predict iROA during 4 years or in 1 year by using the DL approach.Material and Method
Data of this study came from the international database Osteoarthritis Initiative (OAI). The 198 Knee Magnetic resonance (MR) images were used to train the IPFP segmentation DL model. A nested case-control cohort (iROA dataset) was used to train a DL model to predict iROA. Case knees and control knees were all present without radiographic KOA (Kellgren–Lawrence grade, KLG = 0 or 1) at baseline. Each knee accepted MR imaging and X-ray examination annually. Case knees developed iROA (KLG≥2) in a four-year follow-up visit while control knees didn’t. Case knees were matched with a control knee by age, sex, and contralateral radiograph KOA status. Knee sagittal intermediate weighted (IW) fat-saturated (FS) 2D turbo spin-echo (TSE) images of baseline and one year before iROA visit (P-1) were collected for IPFP segmentation and iROA prediction. Fixed flexion knee radiographs of each visit were collected for diagnosis of iROA. Knees without the above image data were eliminated. 701 knees (349 case: 352 control) at baseline and 673 knees (326 case: 347 control) at P-1 were used in this study.For the segmentation part, we use a pretrained 2D DenseNet 1616 for IPFP area segmentation. The segmentation network is fine-tuned on our private IPFP segmentation dataset (178 images training and 20 images for testing). We extract the IPFP area by the generated segmentation mask.Then we train DL model based on the extracted IPFP to predict iROA, using the data from BL or P-1 respectively. The corresponding unsegmented whole-knee-MRI-based DL model was trained for comparison. For the IPFP-based iROA prediction part, we fine-tune the 3D DenseNet1696 on the extracted IPFP part. For the whole-knee-MRI-based iROA prediction part, we fine-tune a pretrained 3D DenseNet169 on the iROA dataset for classification. The flow chart of the prediction task can be seen in figure 1.Dice similarity coefficient (DSC) was used for evaluating the segmentation model. Three widely known metrics: 1) Area under the Curve (AUC); 2) Specificity; 3) Sensitivity were used for evaluating the performance of the classification model. We also use Delong’s test to compare the performance between the IPFP-based model and the whole-knee-based model, while Delong’s test input is the concatenation of each fold prediction.Result and Discussion
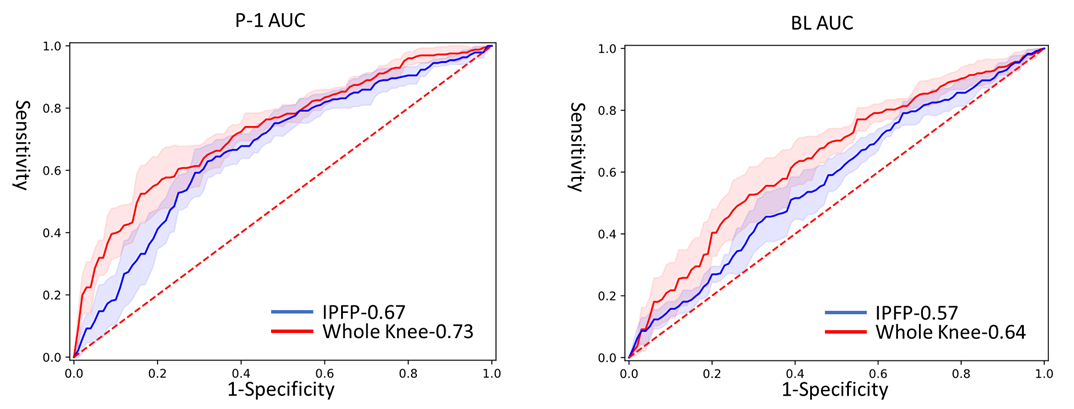
For the segmentation part, DSC is 0.89 for the testing set. In the P-1 period, the whole-knee-MRI-based model yields the best performance of AUC 0.73 while the IPFP-based model yields a comparable performance of AUC 0.67 (P= 0.123). In the baseline period, both prediction models got poor performance: whole-knee-MRI-based model yields AUC of 0.64 while IPFP-based model yields AUC of 0.57 (P= 0.031). The results of prediction models can be seen in table 1 and figure 2.We chose the IPFP as a surrogate to predict knee osteoarthritis because it is a source of inflammation. Besides, it’s a relatively regular and larger structure compared to other organs in the knee and accurate segmentation is easier to accomplish. A previous study found IPFP MRI signal alteration at baseline or P-1 is a risk factor for the onset of radiographic KOA1, 2, 5, even after adjusting for age, sex, BMI, alignment, cartilage, and meniscal damage2. The results of our study show that IPFP can serve as an alternative independent biomarker for predicting iROA in a year but is not very useful for predicting iROA at baseline, which means that inflammation of IPFP is not that obvious at the beginning and become severe as disease progression. Therefore, it’s vital to modify the inflammation of IPFP as early as possible. Our whole-knee-MRI-based model can successfully predict iROA a year in advance. The advantage of this model is skipping of segmentation step which is experience-depending and may sacrifice most features other than the region of interest. The main limitation of our study is that we only train a model with single MR sequence images and miss some valuable features on other sequences. Besides, we didn’t compare the prediction performance with other abnormalities in the knee such as cartilage lesion or bone marrow lesion, which is our next work.Conclussion
IPFP can be regarded as an independent biomarker comparably to whole knee MRI when predicting incidents of knee osteoarthritis in a year. However, it is difficult to use IPFP MRI alteration at baseline to predict incidents of knee osteoarthritis during four years.Acknowledgements
Keyan Yu and Chuanyang Zheng contributed equally to this work.
Xiaodong Zhang and Qi Dou are both co-corresponding authors.
Funding: This project is supported by the National Natural Science Foundation of China (grant No. 81801653).
References
1. Atukorala I, Kwoh CK, Guermazi A, Roemer FW, Boudreau RM, Hannon MJ, et al. Synovitis in knee osteoarthritis: a precursor of disease? Ann Rheum Dis 2016; 75: 390-395.
2. Felson DT, Niu J, Neogi T, Goggins J, Nevitt MC, Roemer F, et al. Synovitis and the risk of knee osteoarthritis: the MOST Study. Osteoarthritis Cartilage 2016; 24: 458-464.
3. Lundervold AS, Lundervold A. An overview of deep learning in medical imaging focusing on MRI. Z Med Phys 2019; 29: 102-127.
4. Berenbaum F. Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!). Osteoarthritis Cartilage 2013; 21: 16-21.
5. Wang K, Ding C, Hannon MJ, Chen Z, Kwoh CK, Hunter DJ. Quantitative Signal Intensity Alteration in Infrapatellar Fat Pad Predicts Incident Radiographic Osteoarthritis: The Osteoarthritis Initiative. Arthritis Care Res (Hoboken) 2019; 71: 30-38.
6. Huang G, Liu Z, Maaten Lvd, Weinberger KQ. Densely Connected Convolutional Networks. Proceedings of the IEEE conference on computer vision and pattern recognition 2017: 4700-4708.
Figures