4611
Effects of vascular territories on the efficiency of DANTE preparation pulse for ASL
Shota Ishida1, Hirohiko Kimura2, Naoyuki Takei3, Yasuhiro Fujiwara4, Tsuyoshi Matsuda5, and Nobuyuki Kosaka2
1Department of Radiological Technology, Faculty of medical sciences, Kyoto College of Medical Science, Nantan, Japan, 2Department of Radiology, Faculty of Medical Sciences, University of Fukui, Eiheiji, Japan, 3GE Healthcare, Tokyo, Japan, 4Department of Medical Image Sciences, Faculty of Life Sciences, Kumamoto University, Kumamoto, Japan, 5Division of Ultra-high Field MRI, Institute for Biomedical Science, Iwate Medical University, Shiwa-gun, Japan
1Department of Radiological Technology, Faculty of medical sciences, Kyoto College of Medical Science, Nantan, Japan, 2Department of Radiology, Faculty of Medical Sciences, University of Fukui, Eiheiji, Japan, 3GE Healthcare, Tokyo, Japan, 4Department of Medical Image Sciences, Faculty of Life Sciences, Kumamoto University, Kumamoto, Japan, 5Division of Ultra-high Field MRI, Institute for Biomedical Science, Iwate Medical University, Shiwa-gun, Japan
Synopsis
This study aimed to assess whether the efficiency of DANTE, a vascular suppression in ASL, is affected by vascular territories. CBF, transit times (TT), and their rates of change were determined in nine vascular territories from the proximal to distal regions. Although CBF reduction rates were not different among the territories, TT extension rates were lower in the distal region than in other regions. No correlation was observed between TT extension and CBF reduction rates. DANTE efficiency is not affected by transit time or vascular territories. Homogenous vascular suppression effects could be obtained by DANTE-ASL.
Introduction
Delays alternating with nutation for tailored excitation (DANTE) pulse1 is a vascular suppression (VS) technique of arterial spin labeling (ASL)2. The right-left differences in the DANTE-ASL signals were smaller than those in the motion-sensitized driven-equilibrium2. Furthermore, the DANTE efficiency is associated with velocity3. In our recent study, we demonstrated that DANTE could selectively eliminate microvascular signals and separate the spin compartments in the ASL4. Further studies have shown that a combination of a simplified two-compartment model and DANTE-ASL could measure arterial cerebral blood volume (CBVa)4. CBVa measurement using DANTE-ASL can be utilized to monitor cerebral hemodynamics in patients with chronic cerebrovascular diseases (CVDs), such as Moyamoya disease. In the early stages of CVDs, elevated CBVa is a typical feature necessary for maintaining cerebral blood flow (CBF) by compensating for decreased cerebral perfusion pressure. A remarkable extension of the arterial transit time (ATT) was observed in patients with CVDs5, and this factor is known to depend on the vascular territories, even in healthy volunteers5,6. Thus, the DANTE efficiency could be affected by the ATT because of its velocity sensitivity. This may reduce the clinical reliability of CBVa measurements using DANTE. Robustness to changes in ATT is a requirement for the clinical application of DANTE. Therefore, in the present study, we assessed whether DANTE efficiency was affected by vascular territories.Methods
We performed additional quantitative analyses on previously acquired data, in which sequential (n = 11) and Hadamard-encoded (n = 10) acquisitions were conducted on a 3.0-T MRI scanner (Discovery MR750, GE Healthcare, USA). DANTE was set as the previous condition (flip angle of 12.5° and gradient area of 10 µs T/m)3. For the sequential multidelay, 2.4 s labeling duration (LD) and three post-labeling delays (PLDs) were used (0.4, 1.2, and 2.0 s for non-DANTE and 0.8, 1.2, and 1.6 s for DANTE scans, respectively). For the Hadamard multidelay, 3.6 s LD was segmented into three LD blocks (0.7, 0.9, and 2.0 s). PLDs were 0.4 and 0.8 s for the non-DANTE and DANTE, respectively. An extra-encoding step in the Hadamard matrix enabled the computation of an additional ASL image with the entire LD (3.6 s) and PLDs (0.4 and 0.8 s) of the Hadamard setting. 3D-T1 weighted images were also obtained.Coregistration was performed on all the ASL images using individual 3D-T1 images. The signal-weighted delay method was used to estimate the initial transit time (TT)7. Subsequently, TT and CBF were calculated on a voxel-by-voxel basis using a least-squares solution with a single-compartment model. Consequently, we obtained TT without DANTE (TTnoVS), TT with DANTE (TTDANTE), CBF without DANTE (CBFnoVS), and CBF with DANTE (CBFDANTE). All parameter maps were spatially normalized to MNI space. White matter regions were excluded from the measurement target because of the low reliability of the ASL signals4. Based on the vascular territory atlas8, TTnoVS, TTDANTE, CBFnoVS, and CBFDANTE were determined by nine volumes of interest (VOIs), in which the anterior cerebral artery (ACA), middle cerebral artery (MCA), and posterior cerebral artery (PCA) were divided into three regions each (proximal, middle, and distal). The TT and CBF values were assessed for each territory, and the rates of TT extension and CBF reduction were evaluated.
Results and Discussion
Table 1 shows the CBF, TT, and their rates of change. Similar trends were observed for the CBF reduction and TT extension rates between the multidelay techniques. In both multidelay methods, the TT extension rates were lower in the distal region than in others. These findings indicate that the DANTE efficiency is independent of the multidelay method. CBF reduction and TT extension rates were smaller with sequential as compared to those with Hadamard (Table 1 and Figure 1).Figure 2 shows the CBF and TT maps calculated from each multidelay dataset using a single-compartment model. Shorter TTnoVS and TTDANTE were observed with Hadamard compared to the sequential. This could be attributed to the difference in LDs between the methods. While sequential multidelay uses 2.4 s LDs for all the boluses, Hadamard LDs were 0.7, 0.9, and 2.0 s. Shorter LDs of the Hadamard led to reduced signal-to-noise ratio (SNR), which could cause TT underestimation5. Inaccurate TTs make the CBF measurement inaccurate. Differences in the bolus design could cause different baseline TT and CBF values, which could result in differences in the rates of change between the techniques.
Figure 3 shows the relationship between TT extension and CBF reduction rates. No correlation was observed. Figure 4 also shows that TTnoVS and TTDANTE were not correlated with the CBF reduction rate (i.e., degree of signal reduction by DANTE), which indicates that the DANTE efficiency is not affected by TT (i.e., vascular territories). In contrast, TT extension rates were negatively correlated with TTnoVS. This could be due to the smaller CBVa in the peripheral regions because the vessel size and fraction in a voxel decreased approaching the periphery. Thus, we considered that this was due to physiological vascularity rather than DANTE efficiency.
Conclusion
DANTE efficiency is not affected by transit time or vascular territories. Homogenous VS effects were observed by DANTE-ASL in all regions of the brain.Acknowledgements
No acknowledgement found.References
- Li L, Miller KL, Jezzard P. DANTE-prepared pulse trains: a novel approach to motion-sensitized and motion-suppressed quantitative magnetic resonance imaging. Magn Reson Med. 2012;68:1423-1438.
- Matsuda T, Kimura H, Kabasawa H, Kanamoto M. Three-dimensional arterial spin labeling imaging with a DANTE preparation pulse. Magn Reson Imaging. 2018;49:131-137.
- Fujiwara Y, Kimura H, Ishida S, et al. Intravascular signal suppression and microvascular signal mapping using delays alternating with nutation for tailored excitation (DANTE) pulse for arterial spin labeling perfusion imaging. MAGMA. 2020;33:367-376.
- Ishida S, Kimura H, Takei N, et al. Separating spin compartments in arterial spin labeling using delays alternating with nutation for tailored excitation (DANTE) pulse: A validation study using T2-relaxometry and application to arterial cerebral blood volume imaging. Magn Reson Med. 2021.
- Ishida S, Kimura H, Isozaki M, et al. Robust arterial transit time and cerebral blood flow estimation using combined acquisition of Hadamard-encoded multi-delay and long-labeled long-delay pseudo-continuous arterial spin labeling: a simulation and in vivo study. NMR Biomed. 2020:e4319.
- Fujiwara Y, Matsuda T, Kanamoto M, et al. Comparison of long-labeled pseudo-continuous arterial spin labeling (ASL) features between young and elderly adults: special reference to parameter selection. Acta Radiol. 2017;58:84-90.
- Dai W, Robson PM, Shankaranarayanan A, Alsop DC. Reduced resolution transit delay prescan for quantitative continuous arterial spin labeling perfusion imaging. Magnetic Resonance in Medicine. 2012;67:1252-1265.
- Mutsaerts HJ, van Dalen JW, Heijtel DF, et al. Cerebral Perfusion Measurements in Elderly with Hypertension Using Arterial Spin Labeling. PLoS One. 2015;10:e0133717.
Figures
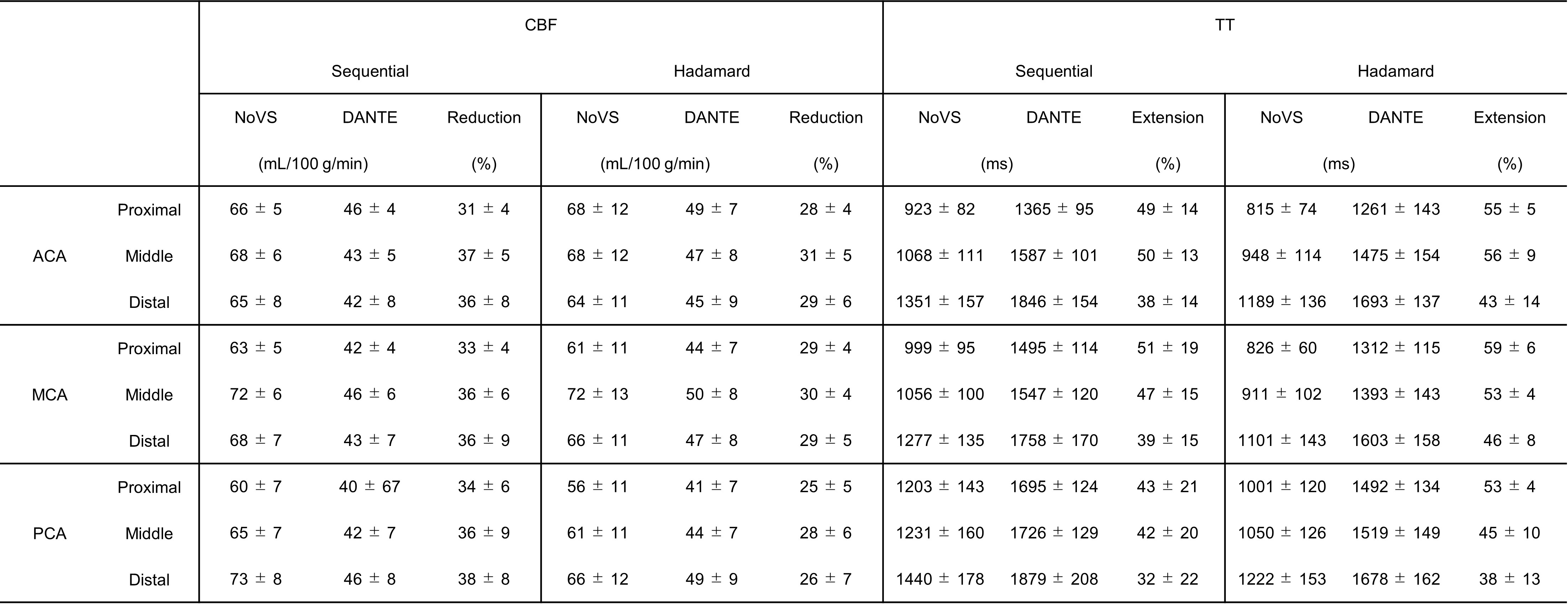
Table 1 The
CBF and transit time (TT) of each vascular territory. The CBF reduction and TT extension
rates were also presented. In both of the multidelay techniques, significant
CBF reduction and TT extensions were induced by DANTE. CBF reduction and TT
extension rates were smaller and larger with the sequential than those with the
Hadamard, respectively, but similarities in trends associated with vascular
territories were observed between the methods.
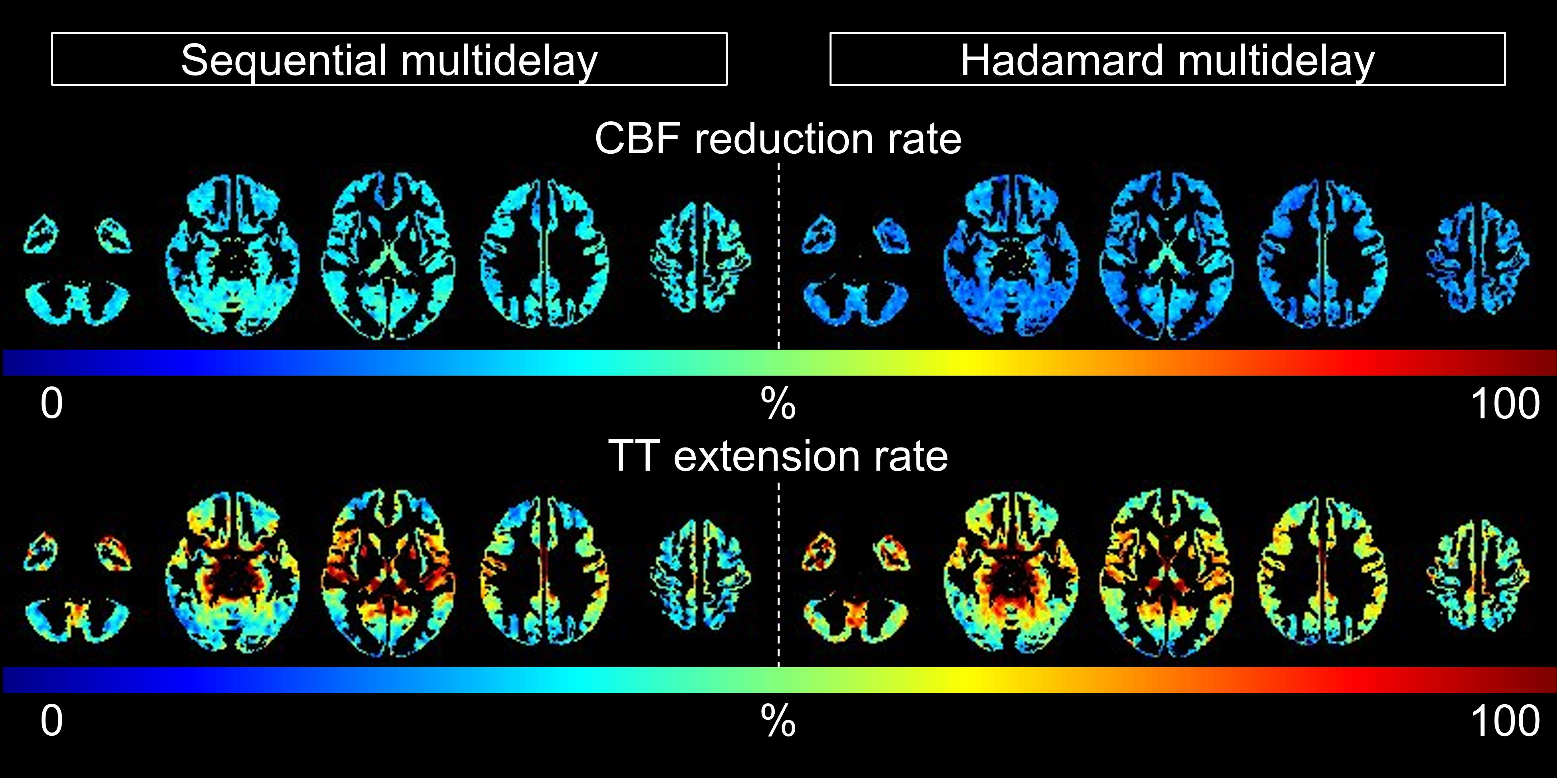
Figure 1 CBF
reduction and transit time (TT) extension maps of each multidelay scan. The
left and right panels show the maps obtained using sequential and Hadamard
multidelay techniques, respectively. CBF reduction rates are independent of
vascular territories. Conversely, TT extension rates were different among the
territories.
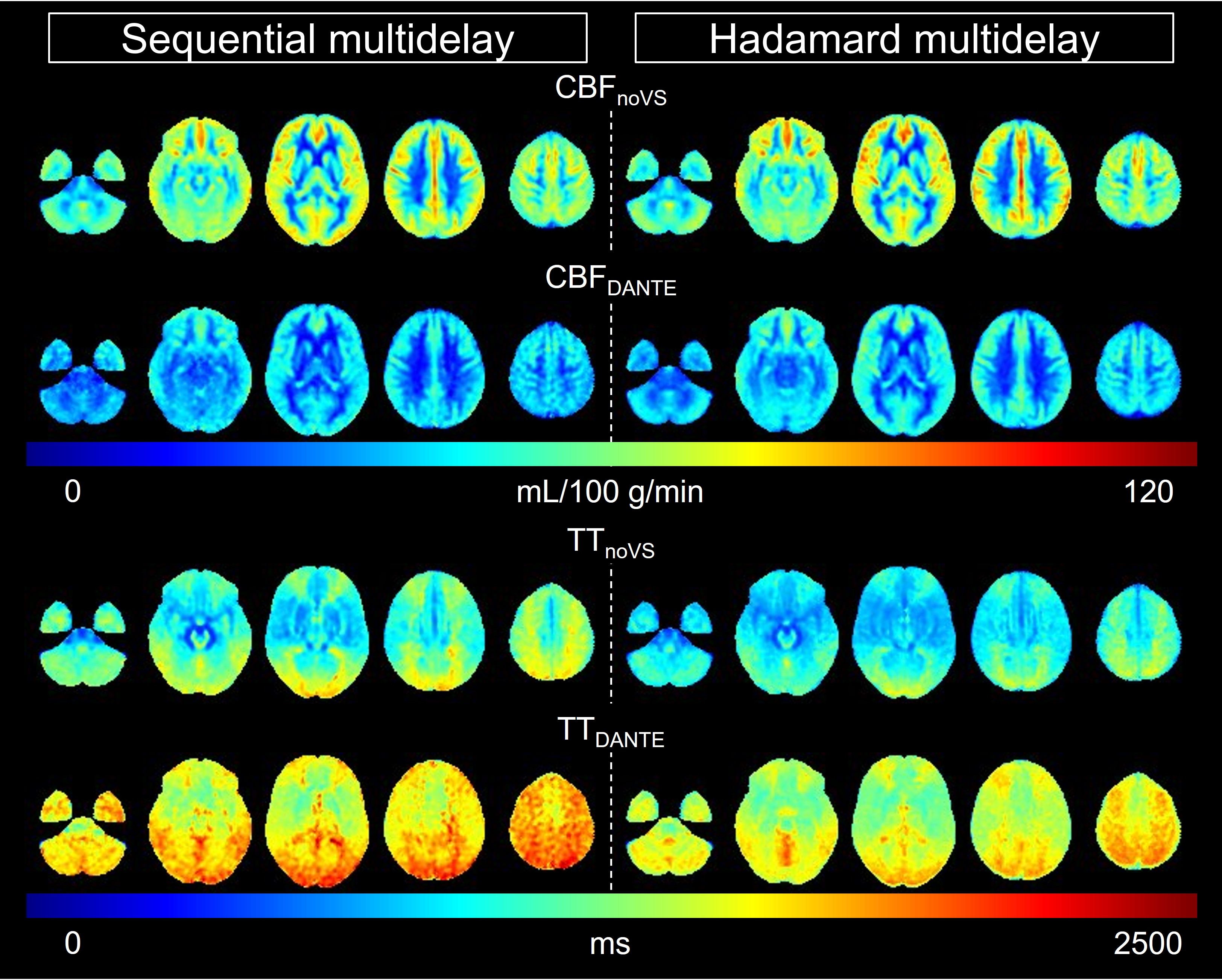
Figure 2 CBF
and transit time (TT) maps with a single-compartment model. Significant CBF
reduction and TT prolongation by DANTE were evident. A similar tendency was
observed between the multidelay scans. Both of the TTs obtained by Hadamard
multidelay were shorter than those obtained by sequential multidelay.
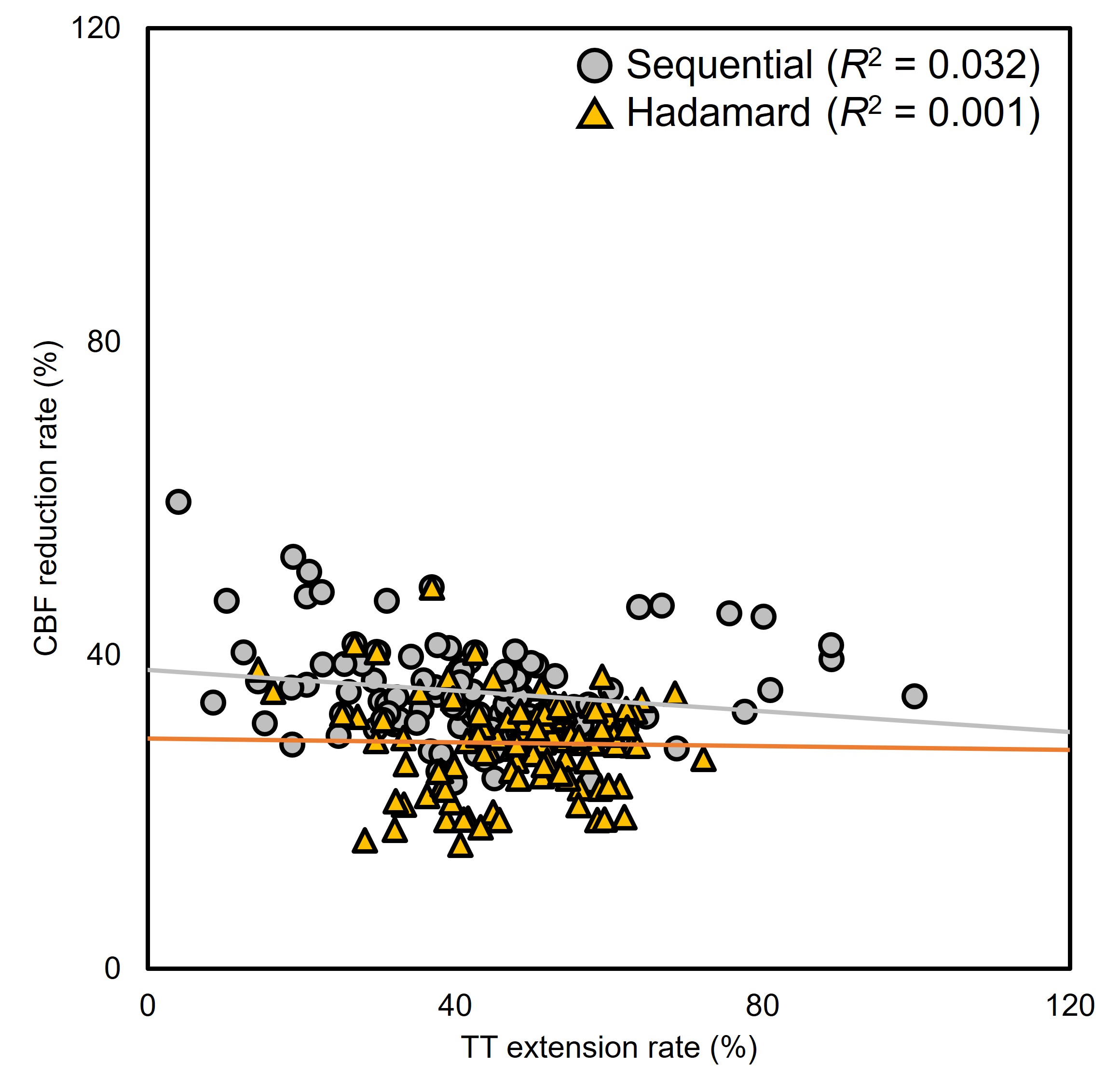
Figure 3 Relationship
between transit time (TT) extension and CBF reduction rates. In both of the
multidelay methods, the TT extension rates were not correlated with CBF
reduction rates.
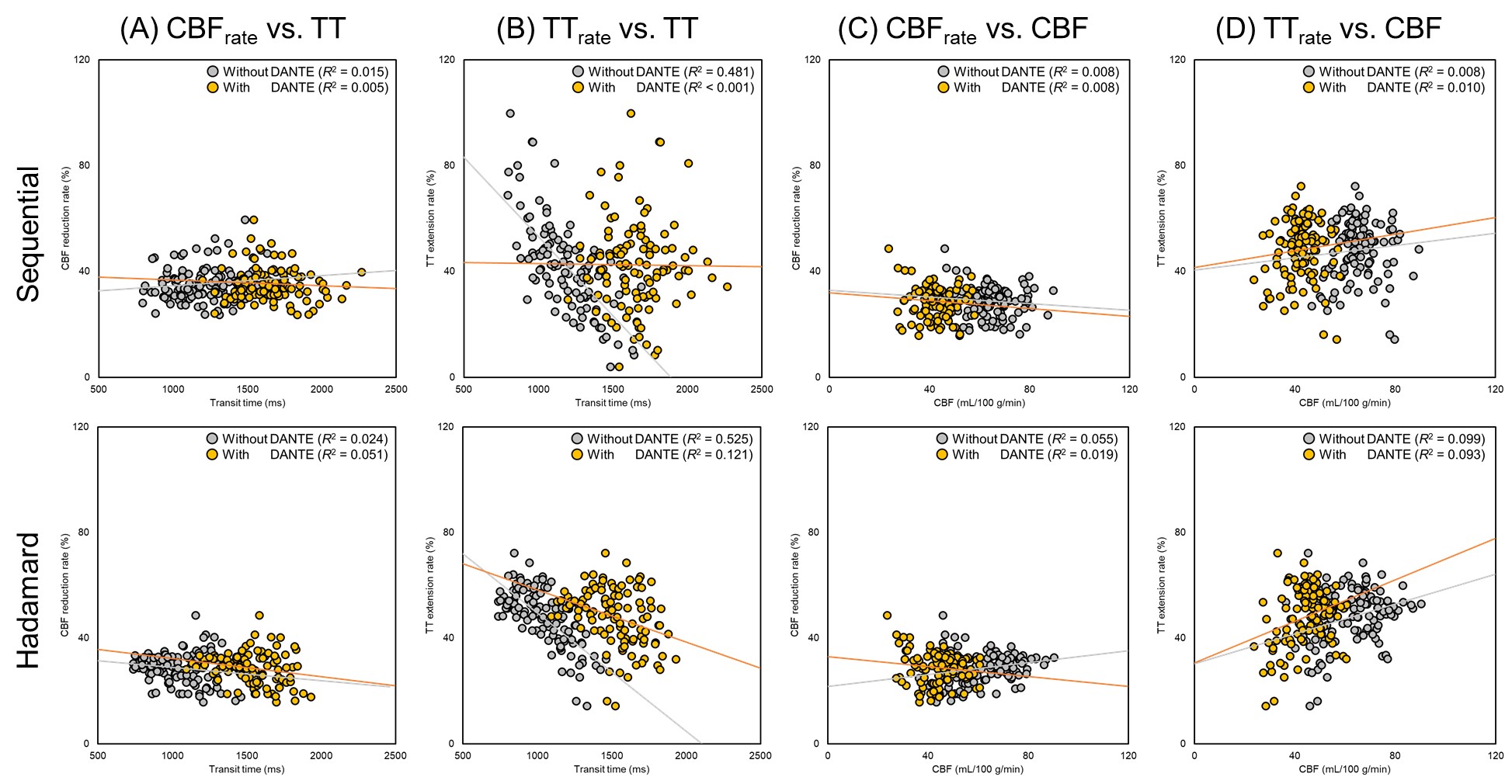
Figure 4 Relationship
between (A) CBF reduction rate (CBFrate) and transit times (TTs)
with and without DANTE, (B) TT extension rate (TTrate) and TTs, (C)
CBFrate and CBF, and (D) TTrate and CBF, respectively.
DOI: https://doi.org/10.58530/2022/4611