4606
Assessment of Cerebral Perfusion in Moyamoya Disease with Dynamic pCASL using a Variable-TR scheme with Optimized Background Suppression1Molecular Imaging and Diagnosis, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan, 2Philips Japan, Tokyo, Japan, 3Radiology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan, 4Division of Radiology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan, 5Philips Healthcare, Tokyo, Japan
Synopsis
The aim of the present study was to determine whether the dynamic pCASL using a variable-TR scheme with optimized background suppression is useful for assessing cerebral perfusion in patients with Moyamoya disease by comparing with 123I-IMP SPECT. ASL dynamic data at 10 time points are acquired by changing the label duration and post label delay. Significant correlations were found between SPECT-CBF and ASL-CBF and between arterial transit time (ATT) and cerebrovascular reactivity (CVR) to acetazolamide challenge on SPECT. ATT was significantly longer in areas where the CVR was decreased than in areas where the CVR was maintained.
INTRODUCTION
Moyamoya disease is a progressive steno-occlusive disease involving the terminal internal carotid artery and the circle of Willis. The indication for bypass surgery is determined by the presence of ischemic symptoms and cerebral blood flow (CBF) status.Clinically, nuclear medicine examination is performed to evaluate CBF and cerebrovascular reactivity (CVR), however, there is no established MR method to quantify CBF in this disease. The quantification of CBF with single-phase arterial spin labeling (ASL) is limited in tissues with a long arterial transit time (ATT). The use of time-encoded ASL in Moyamoya disease has been reported1. This method is time-efficient and can provide a high SNR; however, due to the sub-bolus concept, the implementation of long label duration and post-labeling delay is challenging, and timing flexibility is limited. We have developed a variable-TR pCASL scheme with dynamically optimized background suppression (BGS) and 3D acquisition2. The purpose of our study was to evaluate the clinical utility of this scheme in the evaluation of cerebral perfusion in Moyamoya disease by comparing with single photon emission computed tomography (SPECT).METHODS
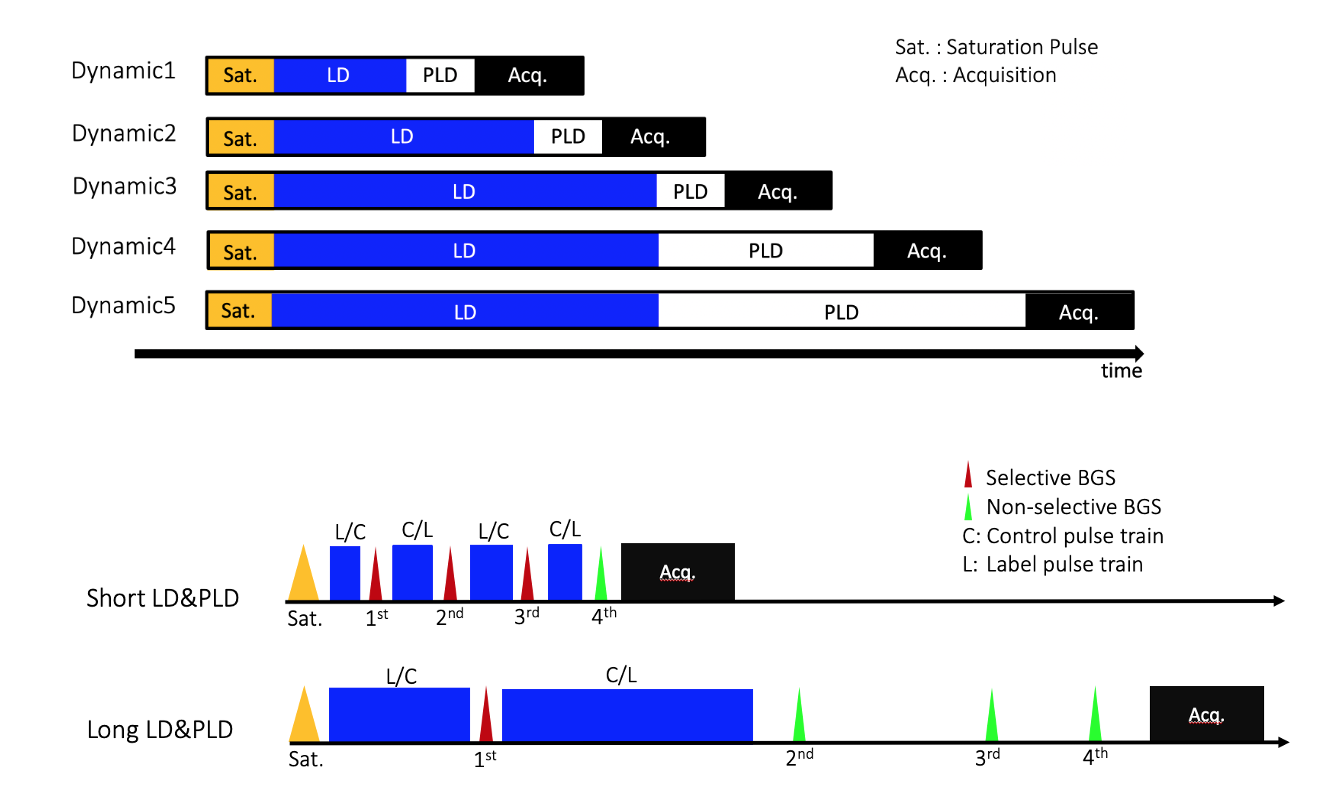
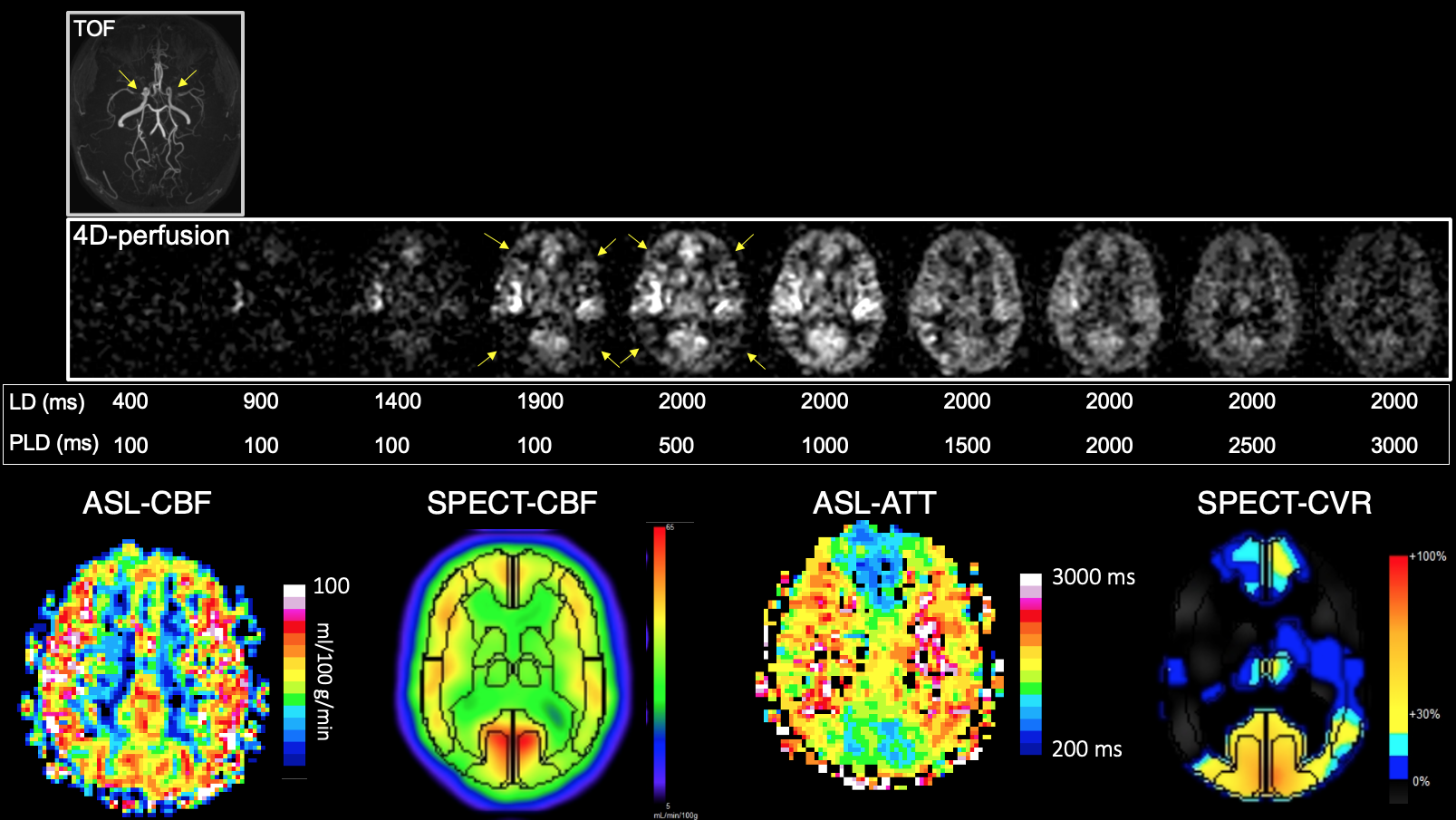
[Patients] Twenty-four patients with Moyamoya disease (31.4±18.2 years) were included in the present study.[MRI] ASL images was obtained on a 3T scanner (Ingenia Elition 3.0T, Philips Healthcare, Best, The Netherlands). In the variable-TR scheme, dynamic pCASL data were acquired by changing label duration (LD) and post label delay (PLD, Figure 1). Four BGS pulses were inserted in LD and PLD. Ten LD and PLD combinations (shortest LD and PLD:400ms, 100ms and longest LD and PLD:2000ms, 3000ms) were used. The 3D-GRASE with whole brain coverage was used. Scan time was 2min30s. From dynamic ASL data, CBF and ATT maps were created using general kinetic model of Buxton3.
[SPECT] 123I-IMP SPECT with acetazolamide challenge was performed with dual table ARG method.
[Image Analysis] ASL and SPECT images were co-registered by affine registration using ImageJ. On a single slice at the basal ganglia, regions-of-interest were manually drawn in the anterior cerebral artery (ACA), middle cerebral artery (MCA, ventral/dorsal), and posterior cerebral artery (PCA) territories. CBF and ATT were measured on ASL, and CBF and CVR to an acetazolamide challenge were measured on SPECT. Areas with large infarction were carefully excluded.
RESULTS
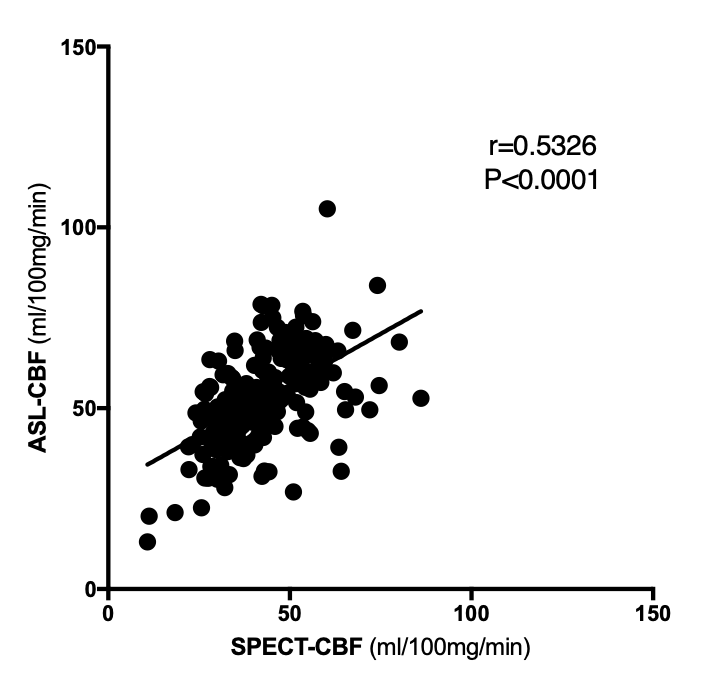
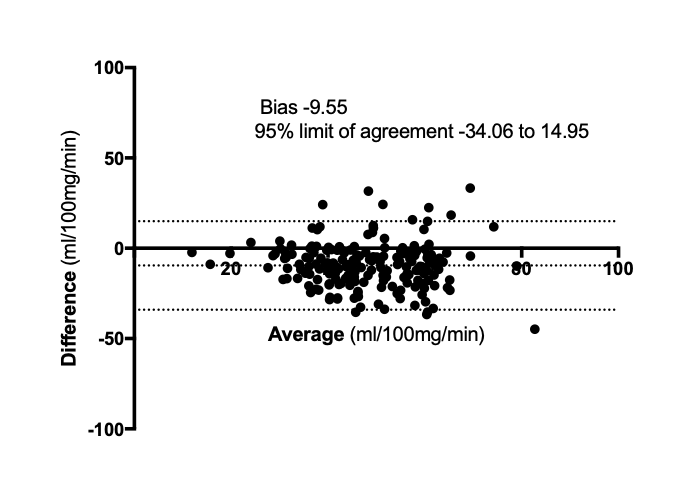
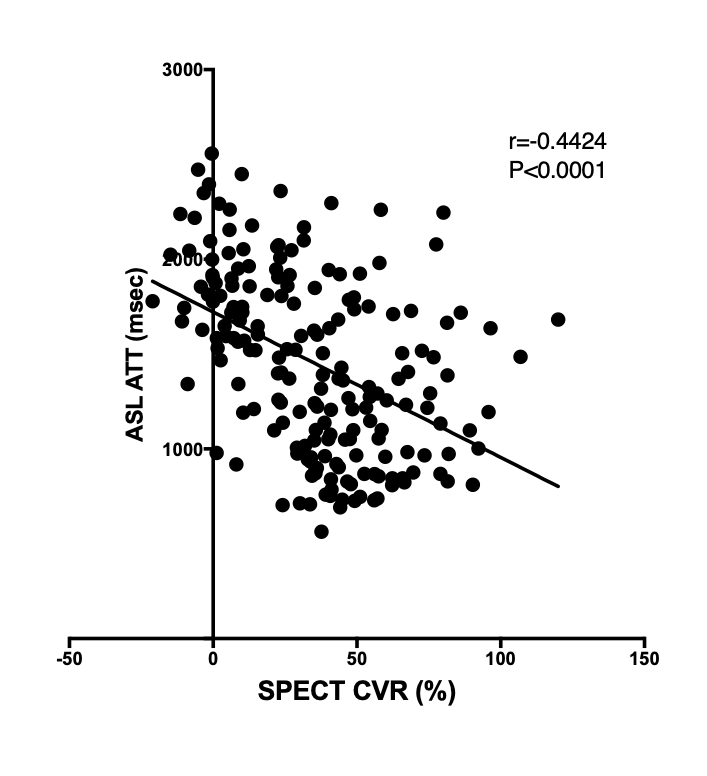
Figure 1 shows schematic drawings of the dynamic pCASL using the multi-TR scheme. Data acquisition at each time point consists of presaturation, and control or label modules followed by data acquisition. ASL dynamic data at 10 time points are acquired by changing the LD and PLD in each session. The BGS timing was optimized for short and long acquisitions. Four BGS pulses are inserted in LD and PLD. Figure 2 illustrates a representative case of Moyamoya disease. In this patient, CBF is preserved throughout the brain on both ASL and SPECT. However, ATT is prolonged on ASL in the bilateral MCA territories, which is almost identical to the area of decreased CVR on SPECT. Figure 3 shows the correlation between SPECT-CBF and ASL-CBF, indicating a significant moderate correlation between the two parameters (r=0.5326, P<0,0001). CBF measured by dynamic pCASL (52.5±13.3 ml/100mg/min, P<0.0001) was significantly higher than that measured by SPECT (43.0±12.6 ml/100mg/min). Figure 4 shows the Bland-Altman plot analysis for the CBF measurements on ASL and SPECT. There was no fixed or systematic error between the two measurements, but a relatively large variability was observed (bias=-0.955, 95% limits of agreement: from 34.06 to 14.95). Figure 5 shows the correlation between ATT measured with the dynamic pCASL and CVR to acetazolamide challenge measured by SPECT. ATT significantly correlated with CVR (r=0.4424, P<0.0001). ATT was significantly longer in areas where the CVR was decreased (CVR<18.4%; ATT=1812±353ms; P<0.0001) than in areas where the CVR was maintained (CVR>18.4%; ATT=1301±437ms). The ROC analysis showed a moderate accuracy with an AUC of 0.807, sensitivity of 87.7% and specificity of 70.4% when the cutoff value was set at 1518ms.DISCUSSION
There is a previous study that compared CBF with time-encoded ASL and SPECT in Moyamoya disease. The study by Setta et al. used CBF ratios and showed moderate correlations, but proportional errors were found1. In contrast, our study used absolute CBF values and showed moderate correlation and no proportional errors. The variable-TR scheme measures over a wide range of timepoints, which allows for accurate ATT correction and CBF quantification. Another previous study showed that ATT correlates with CVR in steno-occlusive cerebrovascular disease4, which is consistent with our results in Moyamoya disease. Our study indicates that ATT can be a useful parameter to reflect CVR in Moyamoya disease.CONCLUSION
Dynamic pCASL using a variable-TR scheme with optimized BGS was found to be useful for assessing cerebral perfusion in patients with Moyamoya disease.Acknowledgements
No acknowledgement found.References
1. Setta K, Matsuda T, Sasaki M, Chiba T, Fujiwara S, Kobayashi M, et al. Diagnostic Accuracy of Screening Arterial Spin-Labeling MRI Using Hadamard Encoding for the Detection of Reduced CBF in Adult Patients with Ischemic Moyamoya Disease. AJNR Am J Neuroradiol. 2021;42(8):1403-9.
2. Obara M, Togao O, Wada T, et al. Pseudo-Continuous Arterial Spin Labeling using Multiple Label- and Post-Label Duration with Optimized Background Suppression. ISMRM 2021
3. Buxton RB, et al. A general kinetic model for quantitative perfusion imaging with arterial spin labeling. Magn Reson Med. 1998;40(3): 383-96.
4. Choi HJ, Sohn CH, You SH, Yoo RE, Kang KM, Yun TJ, et al. Can Arterial Spin-Labeling with Multiple Postlabeling Delays Predict Cerebrovascular Reserve? AJNR Am J Neuroradiol. 2018;39(1):84-90.
Figures