4598
Quantitative analysis of Symptomatic and Asymptomatic Atherosclerotic Middle Cerebral Artery Plaques Using 7T Magnetic Resonance Imaging1Department of Radiology, Beijing Tiantan Hospital, Capital Medical University, Beijing Neurosurgical Institute, Beijing, China, Beijing, China, 2MR Collaboration, Siemens Healthineers Ltd., Beijing, China, Beijing, China, 3Tiantan Neuroimaging Center of Excellence, China National Clinical Research Center for Neurological Diseases, Beijing, China, Beijing, China
Synopsis
A total of 40 MCA atherosclerotic plaques of 34 patients (20 symptomatic and 20 asymptomatic plaques) were quantitatively analyzed of plaque features including plaque burden, length, remodeling index, plaque distribution, and surface morphology using 7T vessel wall Magnetic Resonance Imaging (VW-MRI). Compared with the asymptomatic plaques, symptomatic MCA plaques had larger plaque length and higher plaque burden. Superior-wall distribution and irregular plaque surface were observed more commonly on the symptomatic MCA plaques. 7T VW-MRI is a promising method to evaluate the atherosclerotic plaque features at MCAs.
Introduction
Intracranial atherosclerotic stenosis (ICAS) is one of the most common causes of ischemic stroke in the Asian population.1 In subjects with asymptomatic middle cerebral artery (MCA) stenosis, the overall annual stroke risk is 2.8%, whereas in patients with symptomatic MCA stenosis the risk is 12.5%.2 In recent years, 3 T vessel wall Magnetic Resonance Imaging (VW-MRI) has been demonstrated to be an ideal tool to assess intracranial plaque instability.3 Superior wall plaque of MCAs has a positive association with the occurrence of penetrating artery infarction4. However, the normal middle cerebral artery wall thickness is only 0.2–0.3 mm, which is smaller than the current VW-MR imaging voxel dimensions acquired by 3T VW-MRI.5 It is hard to identify the vessel wall boundaries and to accurately quantify the plaque features under the limited spatial resolution. In this study, plaque characteristics, including plaque length, plaque burden, remodeling index, plaque distribution, and surface morphology were quantitatively analyzed using 7T VW-MRI, and the difference between symptomatic and asymptomatic atherosclerotic MCA plaques was investigated.Methods
From June 2021 to October 2021, thirty-four patients with MCA atherosclerotic plaques from Beijing Tiantan Hospital were enrolled in this study. Patients were recruited according to the following inclusion criteria: (1) had >30% unilateral/bilateral MCA stenosis (in M1 or M2 segment) confirmed by MR angiography; (2) with two or more traditional vascular risk factors including hypertension, hyperlipidemia, diabetes, smoking, et al; (3) sufficient documentation to be labeled as either symptomatic or asymptomatic MCA plaques.MRI was performed on a 7T MR scanner (MAGNETOM Terra, Siemens Healthcare, Erlangen, Germany) using a 32- channel Rx/8Tx head-coil. Three-dimensional time of flight (3D TOF) MRA was performed with maximum intensity projection (MIP) reconstruction to visualize the vascular morphology and MCA stenosis with the following parameters: TR/TE =17.0/4.59ms, FOV =180mm×165mm×36mm, flip angle = 20°, slice thickness=0.3mm, 144 slices, voxel size = 0.3mm×0.3mm×0.3 mm3, GRAPPA =3, time of acquisition (TA) = 7 min 14 s. Then a T1-weighted 3D Sampling Perfection with Application-optimized Contrast using different flip angle Evolutions (SPACE) sequences was carried out for the vessel wall imaging. The parameters were set as follows: TR/TE=1720/9.6ms, FOV=180mm×180mm×140mm, slice thickness=0.4 mm, 352 slices, voxel size =0.4 mm×0.4 mm× 0.4 mm3, the controlled aliasing in parallel imaging results in higher acceleration (CAIPIRINHA) factor =6, TA =9min59s.
The vessel wall imaging data were processed using VesselMass software (Leiden University Medical Centre, version V2020-EXP). The parameters were evaluated by the maximal lumen narrowing (MLN) cross-section of blood vessels, including maximum wall thickness, lumen area (LAMLN), maximum outer area (OAMLN), maximum wall area. The reference lumen was defined as the MCA segment of normal appearance proximal to the stenotic site. The following formulas were used: Stenosis Degree = (1-LAMLN/LARef) ×100%6; Remodeling Index (RI) = OAMLN/OARef (the remodeling mode is classified according to RI value: RI >1.05 is positive remodeling [PR], RI <0.95 is negative remodeling [NR], 0.95< RI <1.05 is no reconstruction)7; Plaque Burden (PB) = maximum wall area/ OAMLN8. All these data were measured twice by a neuroradiologist without knowing the clinical details, and the averages were calculated and applied.
All quantitative data were expressed as means ± standard deviations (SD). Categorical variables were analyzed using Chi-square test or Fisher exact test. Continuous variables were compared using a t-test between symptomatic and asymptomatic side MCAs. A P value <0.05 was considered to be statistically significant.
Results
The clinical characteristics of patients are summarized in Table 1. A total of 40 MCA plaques in 34 patients were analyzed (20 symptomatic plaques, and 20 asymptomatic plaques. Table 2 summarized the plaque features of the two groups. The stenosis degree on the asymptomatic MCAs was significantly lower than that on the symptomatic MCAs (P<0.011). An irregular plaque surface was more commonly found in the symptomatic plaques. Superior-wall location was observed more frequently on the symptomatic plaques than the asymptomatic plaques (80% vs. 20%, P<0.001). The symptomatic plaque exhibited a larger length (13.42±5.96 vs. 9.01±3.36 mm, P=0.007) and higher plaque burden (0.85±0.12 vs. 0.58±0.18, P=0.031) compared with the asymptomatic plaques (Figure 1 and 2).Discussion and Conclusion
In this study, our results showed that the symptomatic MCA plaques had a larger length and higher plaque burden than the asymptomatic plaques. The plaque length might be a significant feature to evaluate the long-axis plaque burden. Also, superior-wall plaque distribution, which would affect the orifice of the perforating branches, was found more in symptomatic lesions. Irregular plaque surface of MCAs was observed more commonly in the symptomatic plaques, which was consistent with the previous study.9 Our results revealed that 7T VW-MRI produce a clear delineation of the intracranial artery wall and characterize the plaque features in both symptomatic and asymptomatic side MCAs.Acknowledgements
We sincerely thank the participants in this study.References
- Johnson CO, Nguyen M, Roth GA, et al. Global, regional, and national burden of stroke, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. The Lancet Neurology. 2019;18(5):439-458.
- Kern R, Steinke W, Daffertshofer M, Prager R, Hennerici M. Stroke recurrences in patients with symptomatic vs asymptomatic middle cerebral artery disease. Neurology. 2005;65(6):859-864.
- Kim BS, Chung PW, Park KY, et al. Burden of Intracranial Atherosclerosis Is Associated With Long-Term Vascular Outcome in Patients With Ischemic Stroke. Stroke. 2017;48(10):2819-2826.
- Xu WH, Li ML, Gao S, et al. Plaque distribution of stenotic middle cerebral artery and its clinical relevance. Stroke. 2011;42(10):2957-2959.
- Mandell DM, Mossa-Basha M, Qiao Y, et al. Intracranial Vessel Wall MRI: Principles and Expert Consensus Recommendations of the American Society of Neuroradiology. AJNR Am J Neuroradiol. 2017;38(2):218-229.
- Xu WH, Li ML, Gao S. In vivo high-resolution MR imaging of symptomatic and asymptomatic middle cerebral artery atherosclerotic stenosis. Atherosclerosis. 2010;212.
- Zhang DF, Chen YC, Chen H, et al. A High-Resolution MRI Study of Relationship between Remodeling Patterns and Ischemic Stroke in Patients with Atherosclerotic Middle Cerebral Artery Stenosis. Front Aging Neurosci. 2017;9:140.
- Teng Z, Peng W, Zhan Q, et al. An assessment on the incremental value of high-resolution magnetic resonance imaging to identify culprit plaques in atherosclerotic disease of the middle cerebral artery. Eur Radiol. 2016;26(7):2206-2214.
- Zhao DL, Deng G, Xie B, et al. High-resolution MRI of the vessel wall in patients with symptomatic atherosclerotic stenosis of the middle cerebral artery. J Clin Neurosci. 2015;22(4):700-704.
Figures
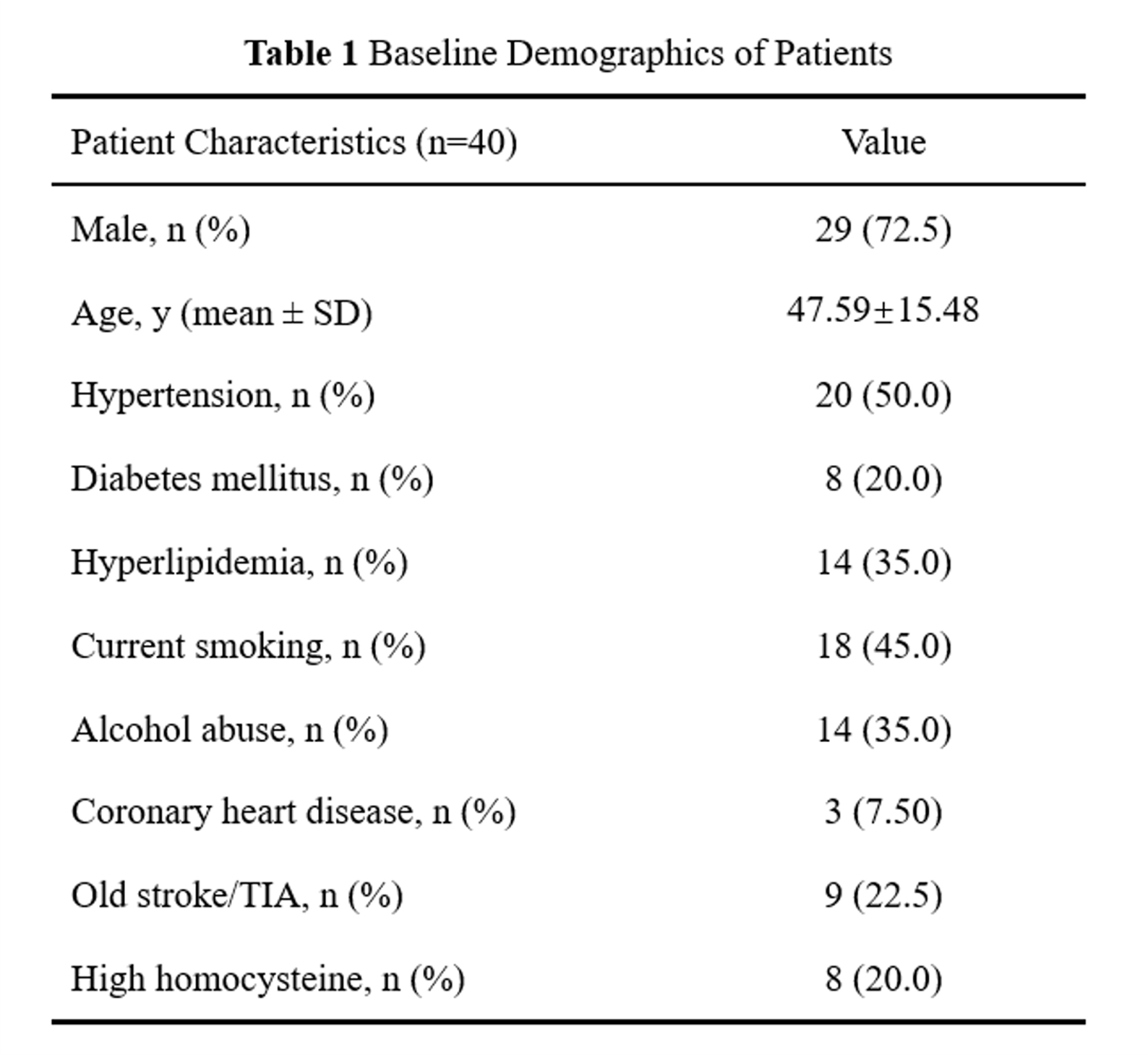
Table 1 Baseline Demographics of Patients
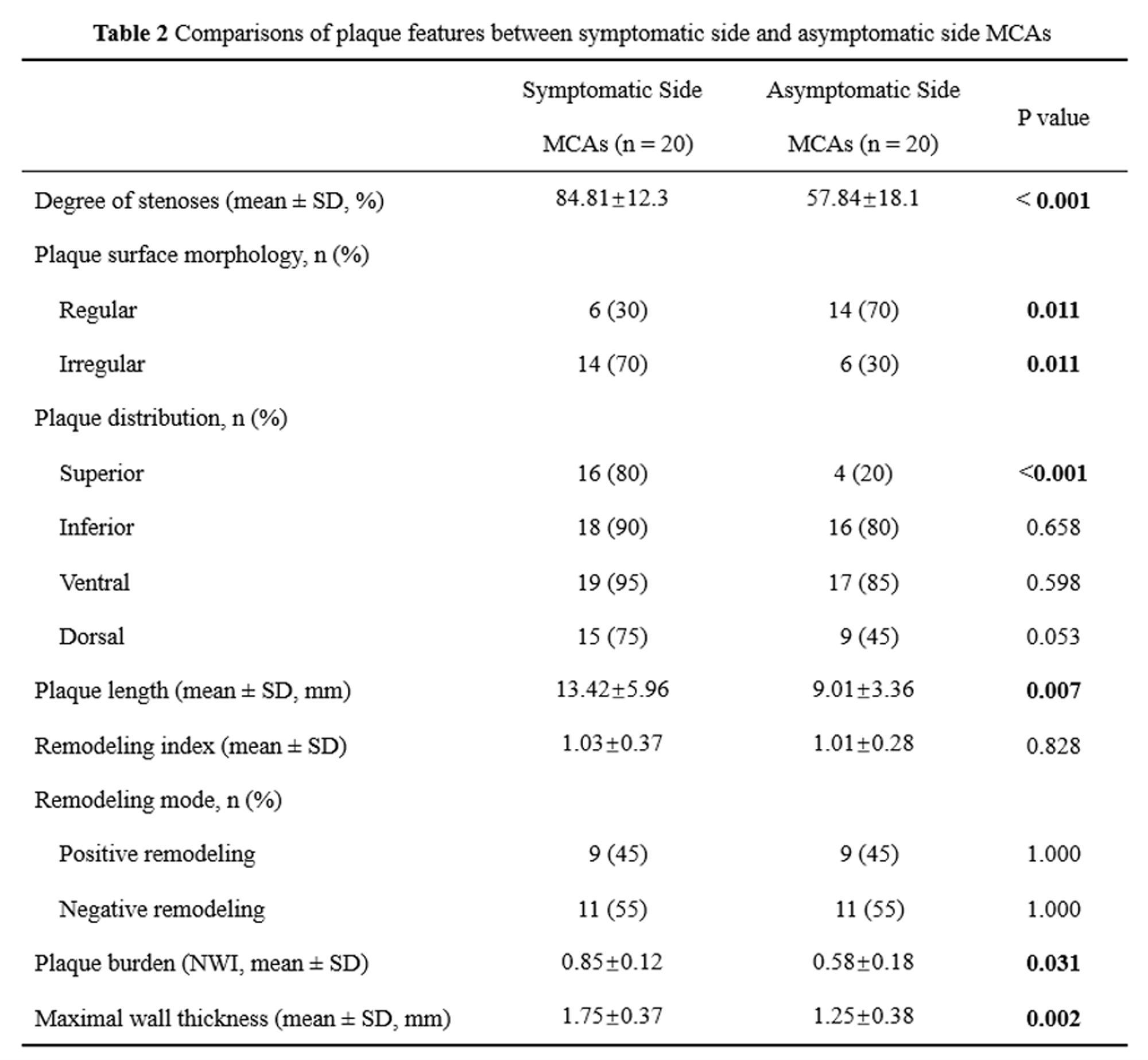
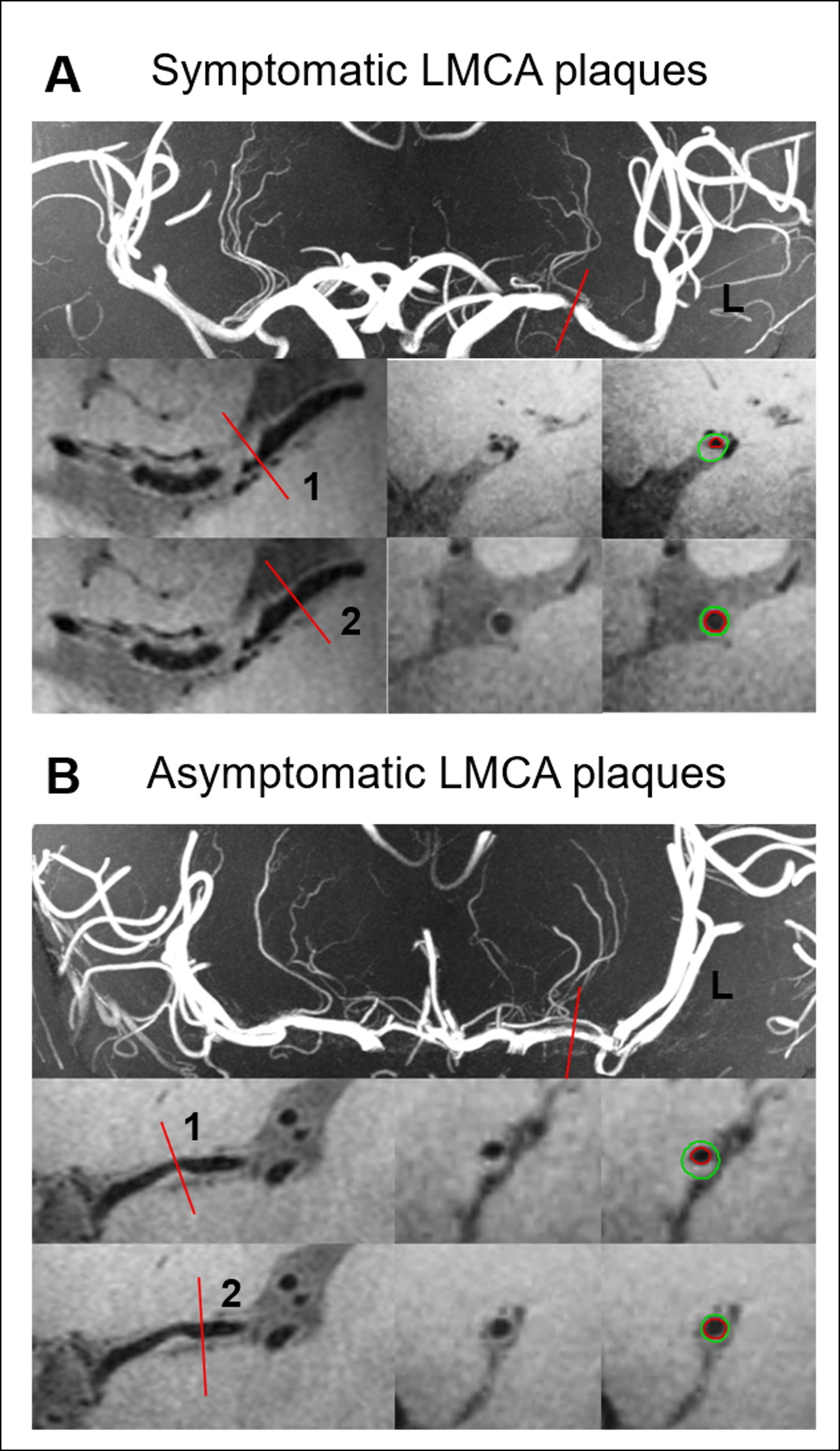
Figure 1. Two representative cases of symptomatic (A) and asymptomatic(B) MCAs plaques were shown on the TOF MRA MIP images and 3D T1 SPACE, respectively. The narrowest lumen plane was marked (red dashed lines) on the TOF MRA MIP images. The site of maximal lumen narrowing (MLN) (1) and the reference lumen (2) were acquired to reconstruct the sagittal images. In the sagittal images, the boundary of vessel wall (outer/inner wall) was semi-automatically tracked by the red and green contour, respectively. The plaque characteristics were calculated and analyzed.
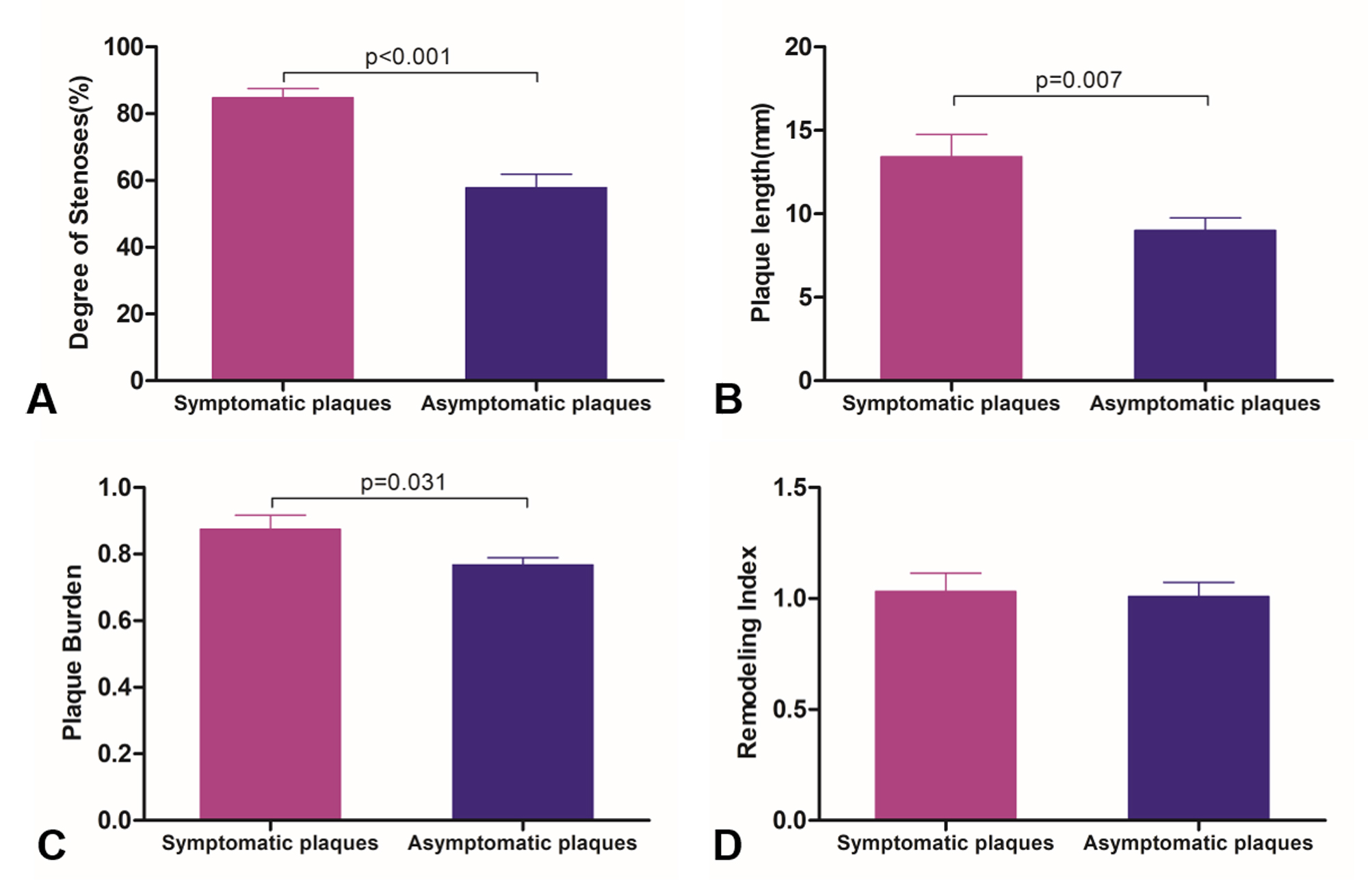
Figure 2. Comparison of the degree of stenoses, plaque length, plaque burden, and remodeling index in symptomatic and asymptomatic MCAs plaques. A p<0.05 was considered to be statistically significant.