4593
Preliminary study on plaque characteristics in young adults with symptomatic intracranial atherosclerotic stenosis1Department of MRI, Shaanxi Provincial People's Hospital, Xi'an, China, 2Philips Healthcare, Xi'an, China
Synopsis
This study used high-resolution magnetic resonance imaging (HRMRI) to explore plaque characteristics of young adults with symptomatic intracranial atherosclerotic stenosis (sICAS). Compared with old patients, young patients with sICAS have a smaller Maximum wall thickness and a greater ability to reconstruct, and are more prone to positive remodeling, which may cover up some patients with atherosclerotic stenosis. The results show great clinical importance for a better understanding of youth intracranial arterial plaque features and highlights the importance of HRMRI.
Introduction
Symptomatic intracranial atherosclerotic stenosis (sICAS) is an important cause of ischemic stroke worldwide1. However, in recent years, more and more young adults have appeared earlier traditional vascular risk factors such as hypertension, diabetes, hyperlipidemia, etc., and the incidence of stroke tended to be younger2. A recent large sample study in China showed that atherosclerosis accounted for 43.7% of ischemic stroke in young adults3. The absence of optimal treatment and preventive recommendations for young patients with stroke leads long-term management to a challenging situation. Atherosclerosis is an important mechanism in occurrence and development of ischemic stroke and accounts for an increasing proportion of the etiology of young stroke4. Although high-resolution magnetic resonance imaging (HRMRI) is increasingly used to evaluate sICAS diseases, including the characteristics of vascular wall lesions and the morphological and quantitative characteristics of plaques5, few researches focus on the plaque characteristics of sICAS in young adults. It is not clear whether there is a difference in the characteristics of atherosclerotic plaque between young and old (>50 years) adults6. Therefore, this study employed HRMRI to explore plaque characteristics of young adults with sICAS.Materials and Methods
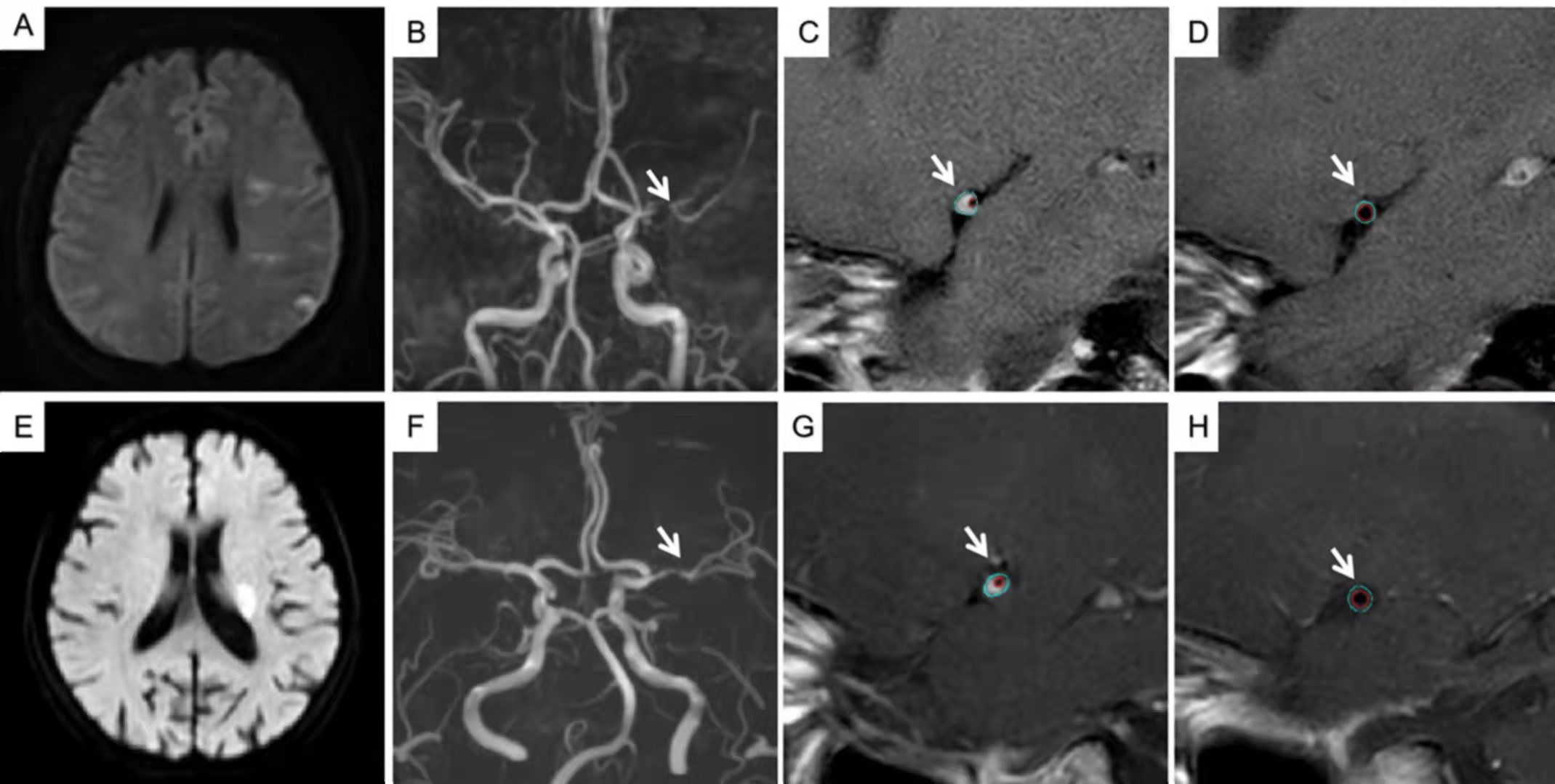
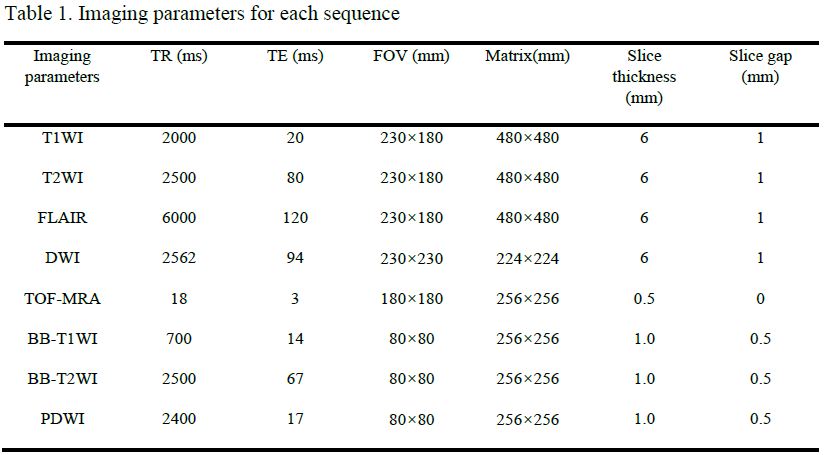
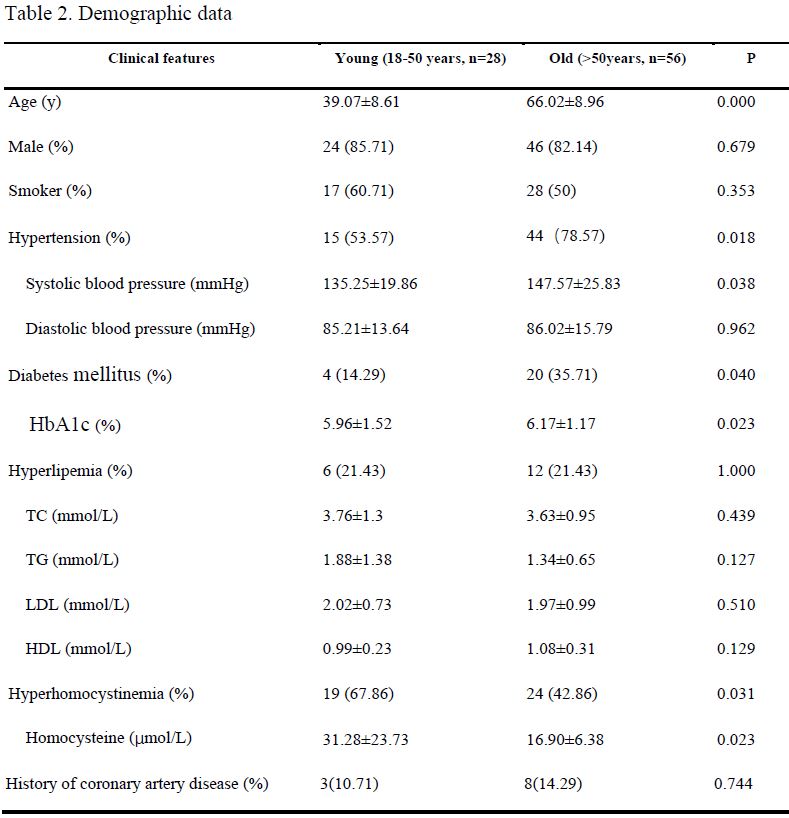
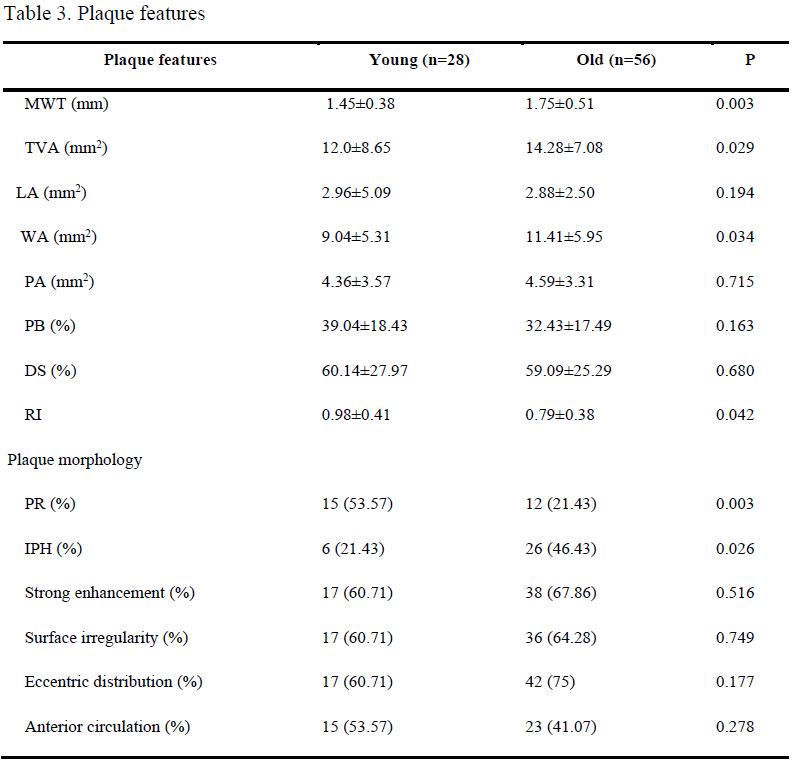
Consecutive patients with sICAS were retrospectively collected from December 2017 to July 2020. All patients underwent MR imaging using a 3.0 T MR scanner (Ingenia CX, Philips Healthcare, the Netherlands) with a 32-channel head coil. Imaging sequences and parameters were presented in table 1. A total of 84 participants were finally evaluated, and 28/56 were assigned to young/old group (table 2). Two experienced neuroradiologists (with 12 and 6 years of experience, respectively) were blinded to the any clinical information and HRMRI scans were analyzed for qualitative and quantitative indicators of vascular walls and plaque at the maximal lumen narrowing (MLN) site. Maximum wall thickness (MWT), total vessel area (TVA), and lumen area (LA) were measured 3 times and the values were then averaged. Then wall area (WA), plaque area (PA), plaque burden (PB), degree of stenosis (DS), remodeling index (RI), and remodeling types can be calculated by the above indicators. The intraclass correlation coefficient (ICC) was used to find the inter-observer reproducibility for the measurements. Logistic regression (binary variables) analyses were performed to assess the differences in plaque features between young and old adult after adjusting for confounding factors, and the results were expressed by the regression slope (β) or odds ratio (OR), together with corresponding 95% confidence intervals (CIs). Clinical risk factors were considered to be confounding factors when the P value was less than 0.1 during comparison analysis between young and old adult. All statistical analyses were performed by SPSS 25.0.Results
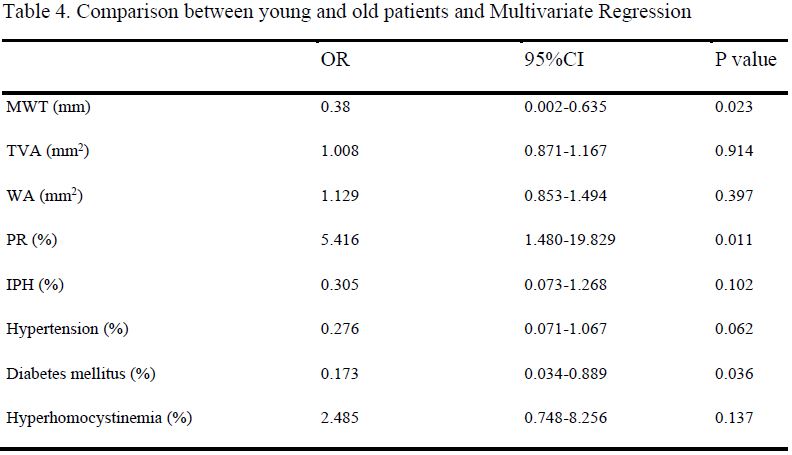
Figure 1 showed typical images and measurements of a young patient and an old patient. Compared with the old group, the young group had significantly less patients with hypertension, diabetes mellitus and significantly lower levels of systolic pressure, HBA1c. While more patients with hyperhomocysteinemia had significantly higher levels of homocysteine in young group. In asymptomatic intracranial arteries, MWT, TVA, WA in young group were significantly lower than those in old group. Compared with the old group, the young group had significantly more patients with positive remodelling and fewer patients with intraplaque hemorrhage (table 3). Multivariable regression analysis revealed that MWT, positive remodelling and the prevalence of diabetes mellitus remained significantly different between young and old adult groups after adjusting for clinical confounding factors (both P < 0.05, table 4). All other indices showed no significant difference between two groups.Discussion
We found that there were differences in plaque characteristics between young and old patients with sICAS through intracranial HRMRI. The maximum vessel wall thickness of young patients was significantly lower than those of old patients, which may represent the progression of atherosclerosis with age. In addition, young group with sICAS had more patients than old group in positive remodelling. The time of atherosclerotic plaque formation in young patients might shorter than old patients. When the development of plaque was still in the early stage, the vessel more inclined to positive remodelling. Besides, atherosclerotic plaque formation in old patients might be closely related to the long-term chronic development of hypertension. Vascular wall compliance was worse and tended to negative remodeling with the expand of life. Our results suggested that positive remodelling affects more in young patients with sICAS. This indicated that we should pay more attention to young patients with no stenosis or mild stenosis, whom might at real high-risk due to positive remodelling. HRMRI is beneficial for screening high-risk plaques from young patients without obvious vascular stenosis in traditional imaging examination but with high risk factors for early onset of large artery atherosclerosis, providing imaging basis for early clinical intervention.Conclusion
In conclusion, we have described the difference between plaques in young and old adults with sICAS. Young patients who have a smaller MWT and a greater ability to reconstruct are more prone to positive remodelling compared with old patients. And this may cover up some patients with atherosclerotic stenosis. This is of great clinical importance for a better understanding of youth intracranial arterial plaque features and highlights the importance of HRMRI for this purpose.Acknowledgements
No acknowledgement found.References
1. Arenillas JF. Intracranial atherosclerosis: current concepts. Stroke 2011;42(1 Suppl): S20–S23.
2. Feigin VL, Roth GA, Naghavi M, et al. Global burden of stroke and risk factors in 188 countries, during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet Neurol 2016; 15: 913–24.
3. Li F, Yang L, Yang R, et al. Ischemic Stroke in Young Adults of Northern China: Characteristics and Risk Factors for Recurrence. European Neurology 2017; 77(3-4):115.
4. Corrado D, Thiene G, Basso C, et al. Atherosclerotic Plaque Healing. N Engl J Med.2021 01 21; 384(3): 292-293.
5. Mandell DM, Mossa-Basha M, Qiao Y, et al. Intracranial vessel wall MRI: principles and expert consensus recommendations of the American Society of Neuroradiology. AJNR Am J Neuroradiol 2017;38(2):218–229.
6. Ekker M S, Boot E M, Singhal A B, et al. Epidemiology, aetiology, and management of ischaemic stroke in young adults. The Lancet Neurology, 2018, 17(9):790-801.
Figures