4567
Deep-learning for automatic assessment of paradoxical movement in left ventricular aneurysm after myocardial infarction using CMR cine imaging1Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, China, 2Philips Healthcare, Shanghai, China
Synopsis
We propose an automatic diagnostic model for left ventricular aneurysm after myocardial infarction. A epicardium segmentation model was established by mixing 2- and 3-chamber images of 90 healthy volunteers, and the dice in all cohorts exceeded 0.95. Five heartphaseimages around end-systolic and end-diastolic stages, multiplied by the predicted mask using the segmentation model were used as the input of the classification model. Data from 259 AMI patients were divided into training cohort (206) and independent testing cohort (53). ResNet was selected to extract the features of 2- and 3- chamber data. Finally, AUC achieved on 0.987/0.946 in training and testing cohort. The automtic deep learning model can be used as a scheme to dignose LVA after AMI, and has potential clinical value for early detection of the risk of the ventricular aneurysm in AMI patients.
abstract
INTRODUCTION:Left ventricular aneurysm(LVA) after myocardial infarction always formed due to a large infarct volume caused by the total occlusion of the proximal left anterior descending artery lack of collateral supply to the ischemia myocardium[1]. Left ventricular aneurysm occurs frequently in patients with anterior myocardial infarction and is the independent predictor of death[2]. This study researched whether the deep learning-convolutional neural network (DCNN) could provide accurately automated detection of paradoxical pulsation in regions of LVA through cardiac magnetic resonance (CMR) cine imaging. We hypothesis that a DCNN trained with cine images would provided quick and accurate diagnosis of LVA in AMI patients after reperfused by primary percutaneous coronary intervention (PPCI) with left anterior descending (LAD) culprit vessel.
METHODS:
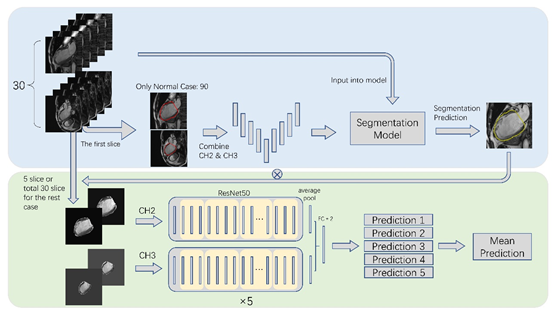
Our CMR study protocol was approved by the institutional ethics committee and was conducted according to the Declaration of Helsinki. Written informed consent was obtained from all participants. A total of 349 participants who underwent CMR with a 3.0T scanner (Ingenia, Philips Healthcare, Best, The Netherlands) were enrolled prospectively. 259 patients with acute myocardial infarction (AMI) were revascularized within 12 hours underwent CMR in the first week, among these, 163(62.93%) patients with LVA. Ninety normal volunteers were recruited as the health controls(HCs). The long-axis 2- and 3-chamber cine images of HCs were applied to built segmentation model of left ventricle and were randomly divided into training cohort (58 cases), validation cohort (15 cases) and testing cohort (17 cases). The long-axis 2- and 3-chamber cine images of the 259 AMI patients were used to establish a classification model for left ventricular aneurysm using DCNN. Therefore, CMR data were randomly split into 206 cases for 5 cross validation and 53 cases for independent testing cohort. The ROIs of the epicardium of the 90 HCs were delineated manually in the end diastole of both 2- and 3-chamber images by an experienced radiologists and saved as epicardium mask. The whole workflow was shown in Figure 1. Firstly, a basic 2D UNet segmentation model was built by HCs to extract the outline of heart. After that, the segmentation model was applied to predict the epicardium mask of AMI patients. We only selected 5 images on the end of systolic and diastolic as the input to better emphasize the cardiac changes. In order to reduce the background noise input into the classification network while reserve part of the information around the heart, we expanded the predicted epicardial mask by 11 pixels and then dotted it with the original image of the classification network. Two 2D ResNets were used to extract features from the data of 2- and 3-chamber images respectively, and the prediction results were obtained by combining the features through two full connection layer. The average of the 5 fold cross-validation results was used as the final result. Finally, we evaluated our segmentation model by Dice and classification model by receiver operating characteristic (ROC) curve and confusion matrix.
RESULTS:
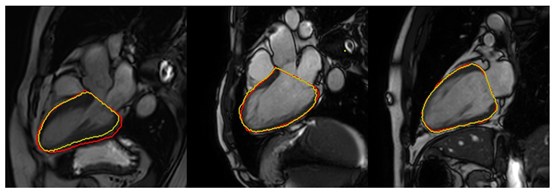
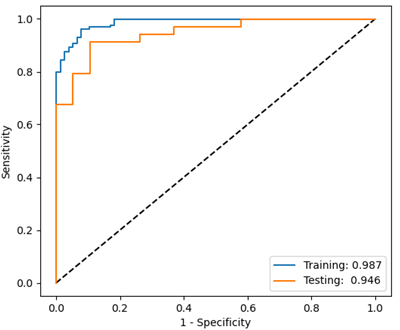
For segmentation model, the average dices on training, validation and testing were 0.970, 0.960 and 0.964. In Figure 2, we displayed three results of the lowest Dice (0.928), the median Dice (0.967) and the highest Dice (0.978) in the testing respectively. And for our classification model, the specific results were shown in Table 1 and the ROC curve was shown in Figure 3. The AUC achieved on 0.987 and 0.946 in training and testing cohort. And the sensitivities of both datasets exceeded 0.9, indicating that the model could well identify patients with ventricular aneurysm.
Discussion:
In current study, a deep-learning model were built to automaticly evaluate paradoxical movement in left ventricular aneurysm after myocardial infarction using cardac cine images, which includes automatic epicardial segmentation and LVA prediction. The epicardial segmentation model based on deep learning was constructed in the 2- and 3-chamber cine images of HCs and the average dices of the test cohort was 0.964, and the model was applied to the cine images of AMI. The performance of classification deep learning model of LVA can achive 0.946. The results suggested that the automtic deep learning model can be used as a scheme to dignose LVA after AMI, and has potential clinical value for early detection of the risk of the ventricular aneurysm in AMI patients.
But our model was still imperfect. Firstly, we only selected 5 images around the end of diastolic and systolic phase from 30 heart phases to build a 2D model, without fully utilizing the data. So a 3D model or a recurrent neural network can be selected. Secondly, the segmentation model was built by only a very small number of data. A more sophisticated and accurate segmentation model could be better. Finally, data from multiple centers can be selected to further verify the model performance.
Conclusion
In general, our deep learning models could provide quickly and accurately automated diagnosis and differentiation of LVA with CMR cine images in AMI patients.
Acknowledgements
Not applicable.References
1. Shen W, Tribouilloy C, Mirode A, Dufossé H, Lesbre J: Left ventricular aneurysm and prognosis in patients with first acute transmural anterior myocardial infarction and isolated left anterior descending artery disease. Eur Heart J 1992, 13(1):39-44.
2. Meizlish J, Berger H, Plankey M, Errico D, Levy W, Zaret B: Functional left ventricular aneurysm formation after acute anterior transmural myocardial infarction. Incidence, natural history, and prognostic implications. N Engl J Med 1984, 311(16):1001-1006.
Figures