4564
Non-linear Association Between NT-proBNP and Septal Native T1 in Non-ischaemic Dilated Cardiomyopathy1Department of Radiology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China, 2MR Collaboration, Siemens Healthcare, Shanghai, China, 3Department of Cardiology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China
Synopsis
This study investigated the relationship between cardiac magnetic resonance (CMR) T1 mapping parameters and N-terminal pro-B-type natriuretic peptide (NT-proBNP) in non-ischaemic dilated cardiomyopathy (DCM) patients. The results showed that, in DCM, a non-linear relationship existed between NT-proBNP and septal native T1, indicating a complex relationship between the secretion of NT-proBNP and myocardial diffuse fibrosis. When NT-proBNP is greater than the inflection point(1105 pg/ml), NT-proBNP may provide additional value for the judgment of myocardial diffuse fibrosis.
Introduction
Non-ischaemic dilated cardiomyopathy (DCM) has a high mortality rate and poor prognosis[1]. Heart failure is the main cause of death in DCM[2]. N-terminal pro-B-type natriuretic peptide (NT-proBNP) is widely used in clinical practice to evaluate the severity of heart failure. Meanwhile, it has been proved that the severity of myocardial fibrosis is closely related to the prognosis of DCM [3] [4] [5]. Therefore, evaluation of myocardial fibrosis by the noninvasive techniques is crucial in the clinical practice.T1 map image obtained by cardiac magnetic resonance (CMR), which quantitatively reflects the tissue characteristics, is sensitive for evaluating myocardial diffuse fibrosis [6]. However, whether the quantitative parameters derived from CMR T1 mapping technique are associated with the clinical severity of heart failure remains unclear. The purpose of this study was to evaluate the relationship between CMR T1 mapping parameters and NT-proBNP in DCM.Methods
In this study, a total of 113 patients diagnosed with non-ischaemic DCM underwent the CMR examination on a 3T scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany). Routine CMR protocols including a 5b(3b)3b MOLLI sequence for T1 mapping acquisition were performed to all the subjects. Typical parameters of T1 mapping were as follows:FOV 340-380mm; matrix size, 197x172; voxel size, 1.3x1.3x8mm3; bandwidth, 1085Hz/px; TR/TE, 2.9/1.15ms; and FA 35°. A region of interest (ROI) was drawn in the midinterventricular septum of the medium section of left ventricle (LV) to evaluate the septal native T1 and septal post T1, avoiding the anterior and inferior insertion parts of right ventricle (RV) (Fig.1). Hematocrit was collected within 24 hours of CMR. NT-proBNP was collected on admission. Univariate and multivariate linear regression models were performed to assess the relationship between NT-proBNP and septal native T1. Restricted cubic spline model was used to further explore the non-linear relationship between NT-proBNP and septal native T1.Results
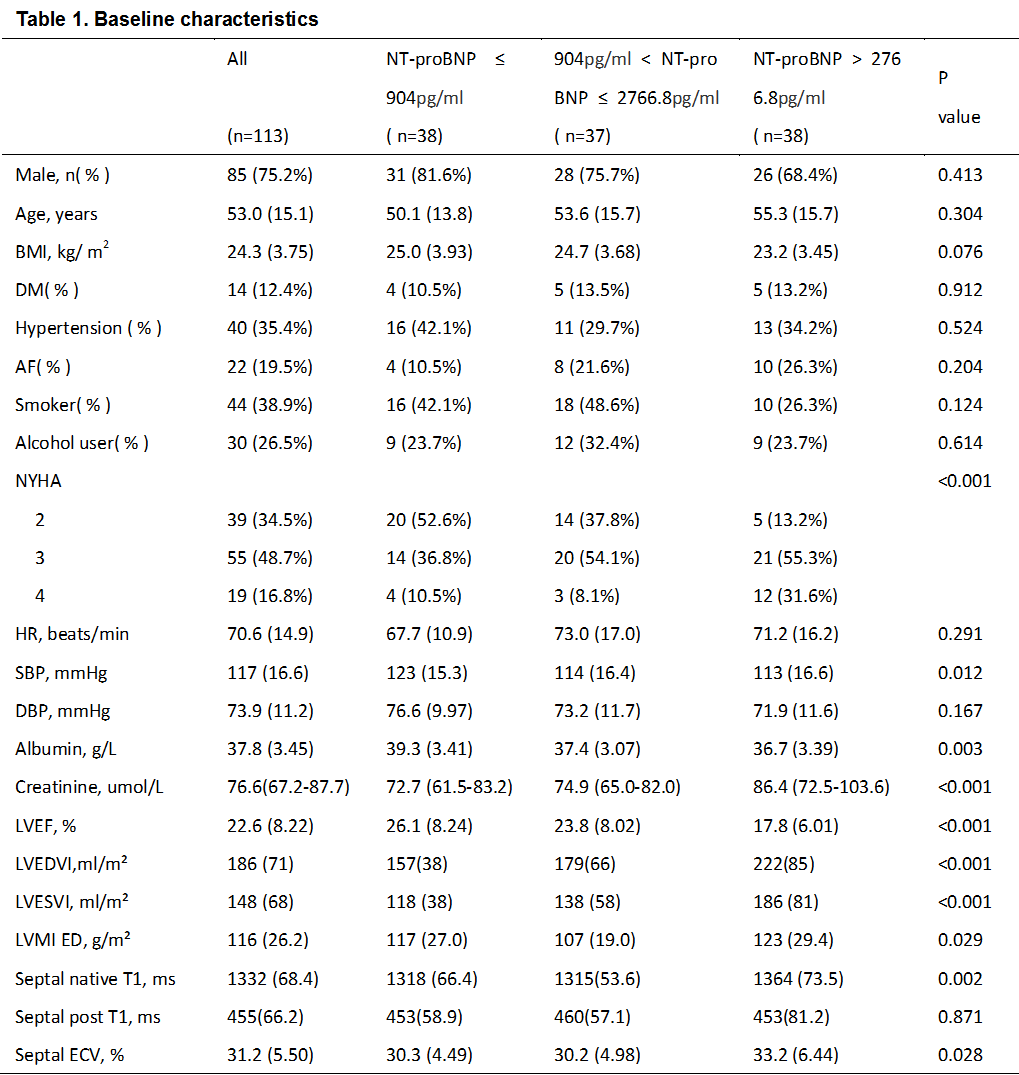
Patients were divided into three groups according to the tertile of NT-proBNP. The baseline characteristics of the three groups are shown in Table 1. Septal ECV differed among the three groups, but was not as significant as septal native T1 (P =0.028 vs. P =0.002). After adjusting for cofounding factors including sex, hypertension, smoker, alcohol user, DBP and body mass index (BMI), compared with patients in the lowest tertile of NT-proBNP , the adjusted mean septal native T1 was 32.99 (95% confidence interval [CI]4.02, 61.95) unit higher for patients in the highest tertile( Table 2). By smooth curve fitting, a non-linear relationship was observed between log2 -transformed NT-proBNP and septal native T1 (Fig.2A). After fully adjusting for confounders, the restricted cubic spline curve exhibited a non-linear relationship between NT-proBNP and septal native T1 (P for non-linearity=0.001) (Fig.2B). Threshold effect analysis indicated that the inflection point of NT-proBNP was 1105 pg/ml. When NT-proBNP > 1105 pg/ml, NT-proBNP was positively correlated with septal native T1 (β= 22.76, 95% CI =9.83, 35.70; P <0.001).When NT-proBNP less than the inflection point, NT-proBNP displayed a negative correlation trend with septal native T1, but the difference was not statistically significant (β= -16.83, 95% CI = -38.08, 4.43; P=0.12) ( Table 3).Discussion and Conclusions
In this study, a non-linear relationship between NT-proBNP and septal native T1 was identified in patients with DCM. This result suggests a complicated relationship between myocardial diffuse fibrosis and the production of NT-proBNP. NT-proBNP mainly synthesized in and secreted from the LV, increased wall tension or stretch may stimulate its secretion [7, 8]. When NT-proBNP ≤ 1105 pg/ml, mild fibrosis may facilitate its reduction by restricting the expansion of ventricle, which means the myocardium still has compensatory ability in DCM. However, if there is too much fibrosis, the stiffness of the myocardium increases, fibrosis may promote the production of NT-proBNP which leads to poor outcomes. This study helps us understand the dual role of myocardial diffuse fibrosis. Depending on the value of NT-proBNP. we may identify whether myocardial diffuse fibrosis plays a positive or negative role. When NT-proBNP>1105 pg/ml, NT-proBNP may help identify the degree of myocardial diffuse fibrosis, while when NT-proBNP ≤ 1105 pg/ml, myocardial diffuse fibrosis may cannot be judged by NT-proBNP.Acknowledgements
No acknowledgement found.References
1. Reichart D, Magnussen C, Zeller T, Blankenberg S. Dilated cardiomyopathy: from epidemiologic to genetic phenotypes: A translational review of current literature. J Intern Med 2019; 286: 362-372.
2. Seferovic PM, Polovina MM, Coats AJS. Heart failure in dilated non-ischaemic cardiomyopathy. Eur Heart J Suppl 2019; 21: M40-M43.
3. Mandawat A, Chattranukulchai P, Mandawat A et al. Progression of Myocardial Fibrosis in Nonischemic DCM and Association With Mortality and Heart Failure Outcomes. JACC Cardiovasc Imaging 2021; 14: 1338-1350.
4. Kiaos A, Antonakaki D, Bazmpani MA et al. Prognostic value of cardiovascular magnetic resonance T1 mapping techniques in non-ischemic dilated cardiomyopathy: A systematic review and meta-analysis. Int J Cardiol 2020; 312: 110-116.
5. Becker MAJ, Cornel JH, van de Ven PM et al. The Prognostic Value of Late Gadolinium-Enhanced Cardiac Magnetic Resonance Imaging in Nonischemic Dilated Cardiomyopathy: A Review and Meta-Analysis. JACC Cardiovasc Imaging 2018; 11: 1274-1284.
6. Messroghli DR, Moon JC, Ferreira VM et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson 2017; 19: 75.
7. Nakagawa Y, Nishikimi T, Kuwahara K. Atrial and brain natriuretic peptides: Hormones secreted from the heart. Peptides 2019; 111: 18-25.
8. Yasue H, Yoshimura M, Sumida H et al. Localization and mechanism of secretion of B-type natriuretic peptide in comparison with those of A-type natriuretic peptide in normal subjects and patients with heart failure. Circulation 1994; 90: 195-203.
Figures
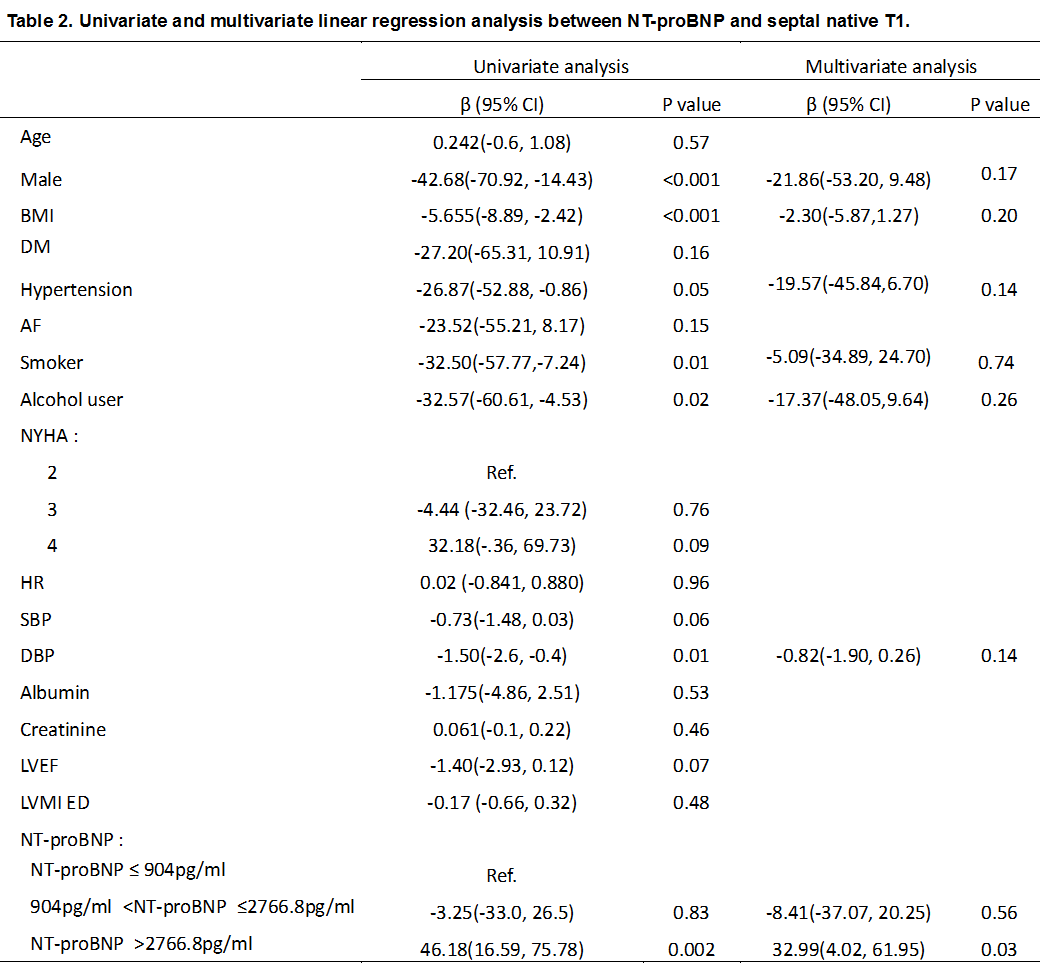
Variables with P values < 0.05 were included in multivariate analysis.
Abbreviations: AF: atrial fibrillation; BMI: body mass index; DBP: diastolic blood pressure; DM:diabetes mellitus; EF: ejection fraction; HR: heart rate; LV: left ventricular; MI ED mass index in end diastole; NT-proBNP: N-terminal pro-B-type natriuretic peptide; NYHA: New York Heart Association; SBP: systolic blood pressure.

NT-proBNP were log2 transformed for fitting the piecewise binary linear regression model. Analysis was adjusted for sex, hypertension, smoker, alcohol user, DBP and BMI.
Abbreviations: BMI: body mass index; CI: confidence interval; DBP: diastolic blood pressure; NT-proBNP: N-terminal pro-B-type natriuretic peptide.
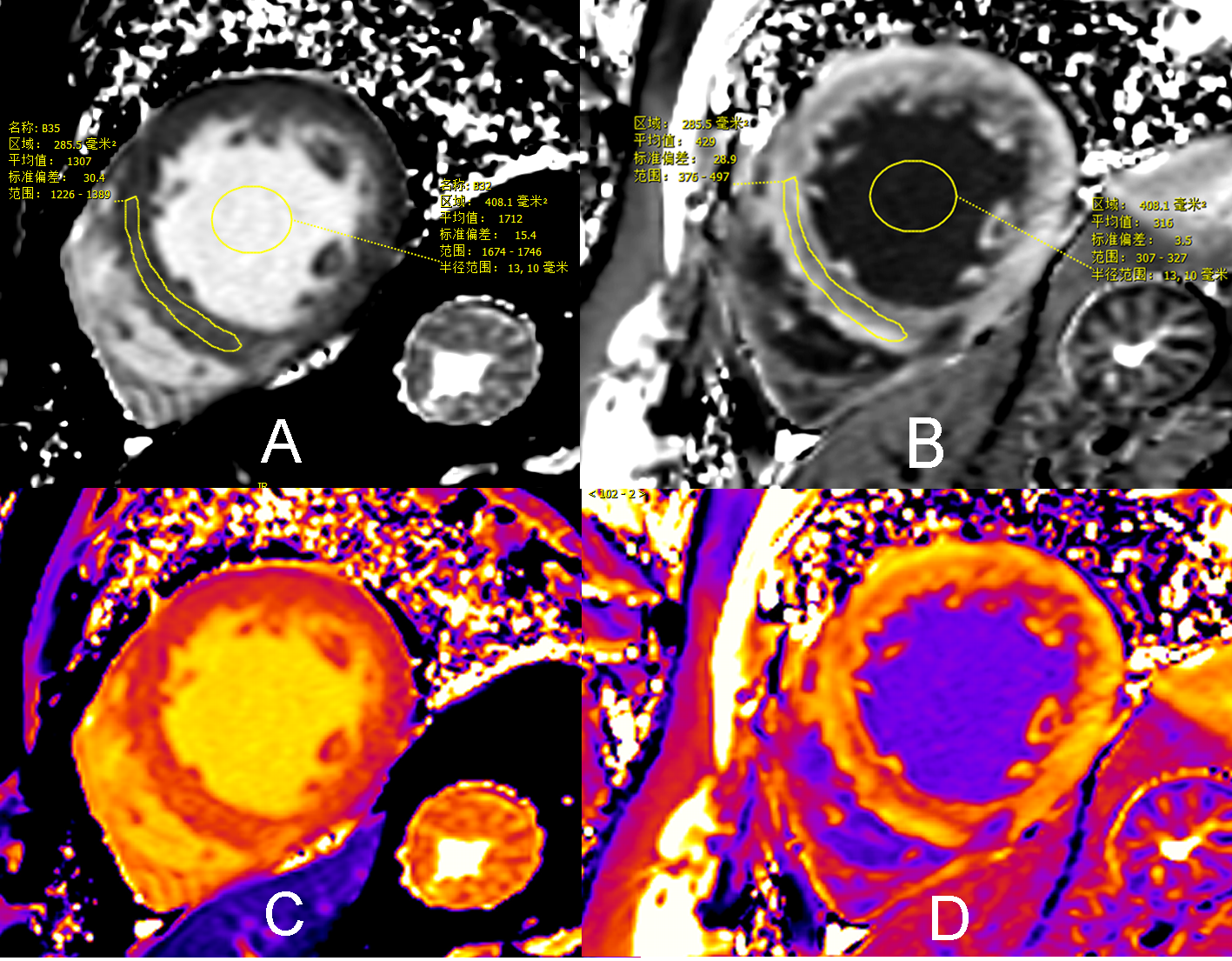
Fig.1 A region of interest (ROI) was drawn in the midinterventricular septum of the medium section of left ventricle (LV) to evaluate the septal native T1 (A) and septal post T1(B). C is the corresponding color image of A. D is the corresponding color image of B.
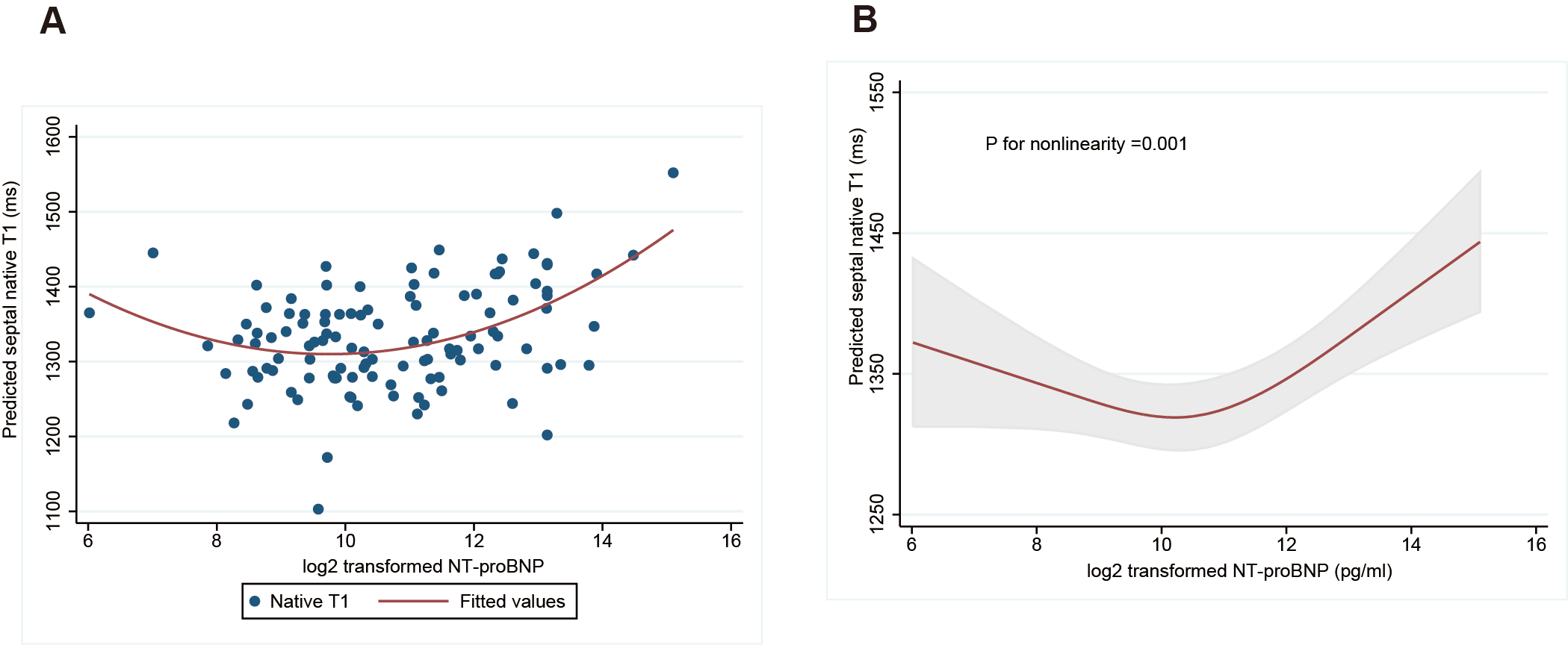
Fig.2 The unadjusted relationship between log2 transformed NT-proBNP and septal native T1 (A), and adjusted restricted cubic spline plot of the association between NT-proBNP and septal native T1 (B). Analysis was adjusted for sex, hypertension, smoker, alcohol user, DBP and BMI.
Abbreviations: BMI: body mass index; DBP: diastolic blood pressure; NT-proBNP: N-terminal pro-B-type natriuretic peptide.