4562
Improvement of distortion-free cardiac IVIM-DWI using motion-compensated single-shot turbo spin echo DWI with fast elastic image registration
Yasuhiro Goto1, Nagao Michinobu2, Masami Yoneyama3, Johannes M Peeters4, Isao Shiina1, Kazuo Kodaira1, Yutaka Hamatani1, Takumi Ogawa1, Mana Kato1, and Shuji Sakai2
1Department of Radiological Services, Tokyo Woman's Medical University, Tokyo, Japan, 2Department of Diagnostic imaging & Nuclear Medicine, Tokyo Woman's Medical University, Tokyo, Japan, 3Philips Japan, Tokyo, Japan, 4Philips Healthcare, Best, Netherlands
1Department of Radiological Services, Tokyo Woman's Medical University, Tokyo, Japan, 2Department of Diagnostic imaging & Nuclear Medicine, Tokyo Woman's Medical University, Tokyo, Japan, 3Philips Japan, Tokyo, Japan, 4Philips Healthcare, Best, Netherlands
Synopsis
We evaluated the feasibility of the combined use of MoSE CINE imaging (to determine exact TD as a preparation procedure), MoCo-TSE-DWI acquisition and FEIR post-processing (to register the respective diffusion images) for improving the robustness of quantitative cardiac IVIM mapping. Combined use of the MoSe-CINE procedure for determining the exact cardiac trigger delay, MoCo-TSE-DWI acquisition, and FEIR post-processing to register among all source images, could be useful to increase the robustness of image quality and improve the quantitative accuracy in myocardial IVIM mapping.
Introduction
Cardiac DWI has a potential to achieve improved clinical diagnosis through novel micro-structural and functional assessment1. The intravoxel incoherent motion (IVIM) theory, proposed by Le Bihan et al.2, enables evaluation of living tissue diffusion movement and micro-vessel perfusion in vivo using quantitative parameters obtained from the multi-b-value DWI, and myocardial IVIM may play an important role assessment of various heart diseases3-6. In previous study, we reported a utility of cardiac turbo spin-echo based DWI (TSE-DWI) with peripheral gating in comparison with conventional EPI-DWI with cardiac gating7. Furthermore, MoCo-TSE-DWI, an M1-nulled DW-TSE using motion-compensated motion probing gradient (MPG), has been reported to improve myocardial signal un-uniformity due to myocardial slight movement8.Empirically, to obtain clinically acceptable myocardial diffusion images, there are two important requirements especially for minimizing the influence of cardiac motion-related artifacts: choice of exact cardiac trigger delay (TD) and image registration-based motion correction.Commonly, the exact TD for the acquisition is determined by using system automatic pre-set timing, but there is still sub-optimal choice of TD in some cases, resulting in deterioration of quantitative accuracy. Recently, we proposed a Motion-Sensitive (MoSe) CINE imaging for determining accurate TD setting which leads to increase the robustness of image quality in quantitative myocardial mapping9.On the other hand, small motions of the heart may still occur due to motion of the diaphragm, variations in R-R interval. For IVIM mapping, these variations of in-plane heart shape among b-values/MPG directions/signal averages can be mitigated by registering each image before creation of the parametric diffusion map. A method for the registration is called Fast Elastic Image Registration (FEIR)10, has proven accurate in cardiac T1 mapping11. FEIR has recently been applied for prostate diffusion imaging, resulting in reducing the misalignment between b0 images and high-b value images12. Moreover, the combined use of MoSE CINE imaging and FEIR further improves the robustness of myocardial relaxation mapping13.In this study, we evaluated the feasibility of the combined use of MoSE CINE imaging (to determine exact TD as a preparation procedure), MoCo-TSE-DWI acquisition and FEIR post-processing (to register the respective diffusion images) for improving the robustness of quantitative cardiac IVIM mapping.Methods
[Subjects] Conventional TSE-DWI (No FEIR), along MoCo-TSE-FEIR along b factor and direction (FEIRb&D), average (FEIRAve), and all (FEIRAll) with a 3.0T MR clinical imager (Ingenia, Philips Healthcare) for six healthy volunteers (age range: 26-44 years) were analyzed. [IVIM-DWI imaging parameters] FOV=300x300mm2, actual matrix size = 1.88 x 1.88 mm, Compressed SENSE-factor = 4.0, TE = 72ms, TR = 4beats, slice thickness = 12 mm, and three directions with b-values 1, 20, 50, 100, 150, 200, 300, 500 s/mm2. The actual trigger delay (TD) and data acquisition window were determined by CINE imaging. In each individual, three slices of left ventricular short-axis images were divided into 16 segments. The ADC, D*, D and f values of each segment were measured. These four parameters were defined by the following formula. The bi-exponential IVIM model is expressed as: SDWI /S0 = f*exp ( -bD*) + (1-f) *exp (-bD) where S0 is SDWI at b = 0 seconds/mm2, SDWI the signal intensity at a given b-value, D the self-diffusion coefficient, f the self-diffusion fraction, and D* the pseudo-diffusion coefficient. The coefficient of variation (CV), mean, and standard deviations for a total 96 of four parameters were calculated and compared among the four IVIM-DWI imaging. Statistical analysis was performed with Steel-Dwass test and judged the difference as significant at p<0.05.Results & Discussion
ADC in FEIRall was significantly smaller than that in FEIRave (p<0.0001) and No-FEIR (p=0.01), and was significantly greater than that in FEIRb&D (p=0.02). There was no significant difference in D*, D and f values among the four IVIM-DWI imaging (Table 1). CVs for all four parameters were smaller in FEIRall than in FEIRb&D FEIRave, and No-FEIR. For all four parameters, the CV in FEIRall was significantly smaller than that in No-FEIR. CV for ADC was significantly small in FEIRall than in FEIRb&D and FEIRave (Figure.1). FEIRall demonstrated small individual and site-specific difference in the parameters obtained from IVIM-DWI imaging, compared with other three imaging. ADC value showed the greatest difference among the four IVIM-DWI imaging. ADC value of FEIRall approximated the D value, while the other three imaging showed a discrepancy between ADC and D values. This result suggests that ADC obtained from FEIRall is theoretically the most accurate.Conclusion
Combined use of the MoSe-CINE procedure for determining the exact cardiac trigger delay, MoCo-TSE-DWI acquisition, and FEIR post-processing to register among all source images, could be useful to increase the robustness of image quality and improve the quantitative accuracy in myocardial IVIM mapping.Acknowledgements
No acknowledgement found.References
1. Nielles-Vallespin S, et.al, Cardiac Diffusion: Technique and Practical Application. J Magn Reson Imaging. 2020 Aug;52(2):348-368. doi: 10.1002/jmri.26912.2. Le Bihan, D. et al. Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology 1988;168, 497–505, https://doi.org/10.1148/radiology.168.2.3393671.3. Spinner GR, et al. Bayesian intravoxel incoherent motion parameter mapping in the human heart. J Cardiovasc Magn Reson. 2017 Nov 6;19(1):85. doi: 10.1186/s12968-017-0391-1.4. Xiang SF, et al. STROBE-A preliminary investigation of IVIM-DWI in cardiac imaging. Medicine (Baltimore). 2018 Sep;97(36):e11902. doi: 10.1097/MD.0000000000011902.5. Spinner GR, et al. On probing intravoxel incoherent motion in the heart-spin-echo versus stimulated-echo DWI. Magn Reson Med. 2019 Sep;82(3):1150-1163. doi: 10.1002/mrm.27777. 6. Xiang SF, et al. Intravoxel Incoherent Motion Magnetic Resonance Imaging with Integrated Slice-specific Shimming for old myocardial infarction: A Pilot Study. Scientific Reports 2019:9:19766. 7. Goto Y, et.al, Simple and robust cardiac diffusion weighted imaging using single-shot Turbo Spin-Echo with peripheral pulse gating. Proc. ISMRM:2016.3476). 8. Goto Y, et al, Improvement of distortion-free cardiac diffusion weighted imaging (DWI) using motion-compensated single-shot turbo spin-echo (MoCo-TSE) DWI. Proc. ISMRM:2020.2077.9. Shiina I, et al, Motion-Sensitive (MoSe) CINE imaging: utility for improving robustness of myocardial quantitative mapping. Proc. ISMRM:2020.2061.10. Kabus S, et al. Fast elastic image registration. Proc. MICCAI:2010. 81–89.11. Zhang S, et al. Cardiac magnetic resonance T1 and extracellular volume mapping with motion correction and co-registration based on fast elastic image registration. MAGMA. 2018 Feb;31(1):115-129.12. Buerger C, et al. Comparing nonrigid registration techniques for motion corrected MR prostate diffusion imaging. Med Phys. 2015 Jan; 42(1): 69–80. doi: 10.1118/1.4903262.13. Ogawa T, et al. Minimizing motion artifacts in myocardial quantitative mapping by combined use of motion-sensitive CINE imaging and FEIR. ISMRM:2021.1382.14. Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation,105:539-42,2002.Figures
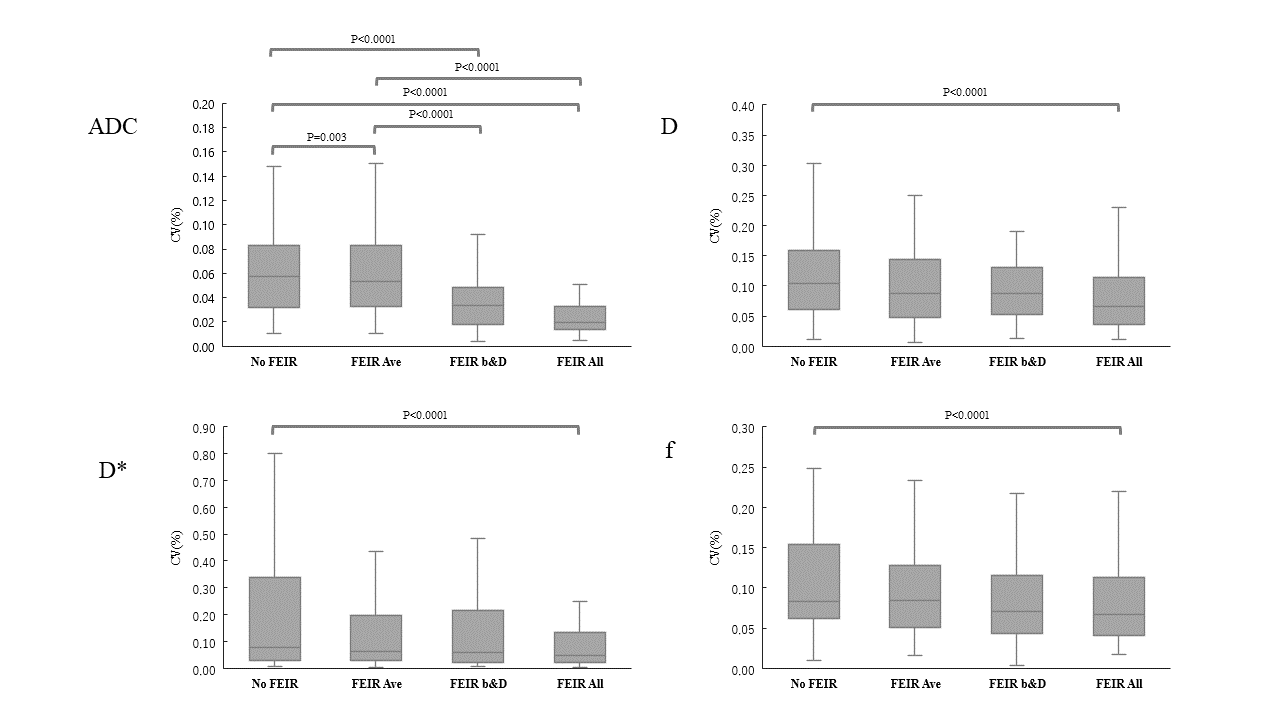
Figure
1. We show results of CV at the heart in each myocardial segments and each
FEIR.
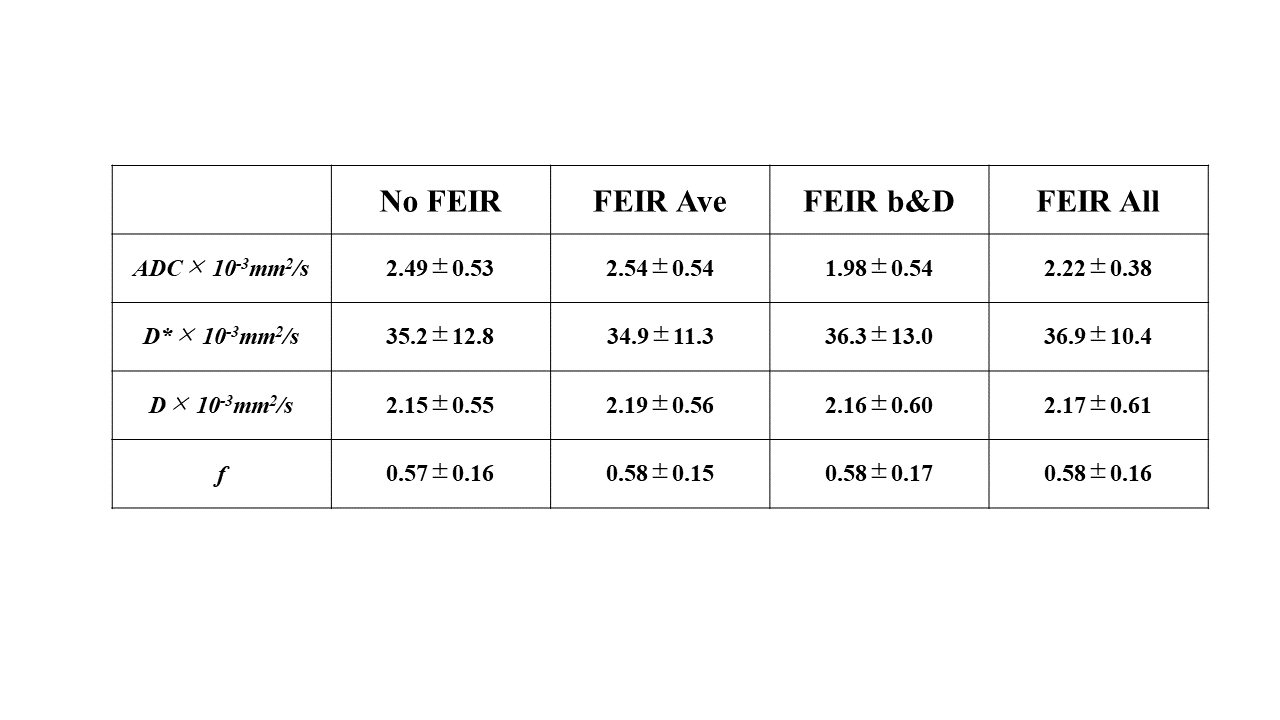
Table 1. IVIM parameters measured
on 16
myocardial segments of six volunteers.
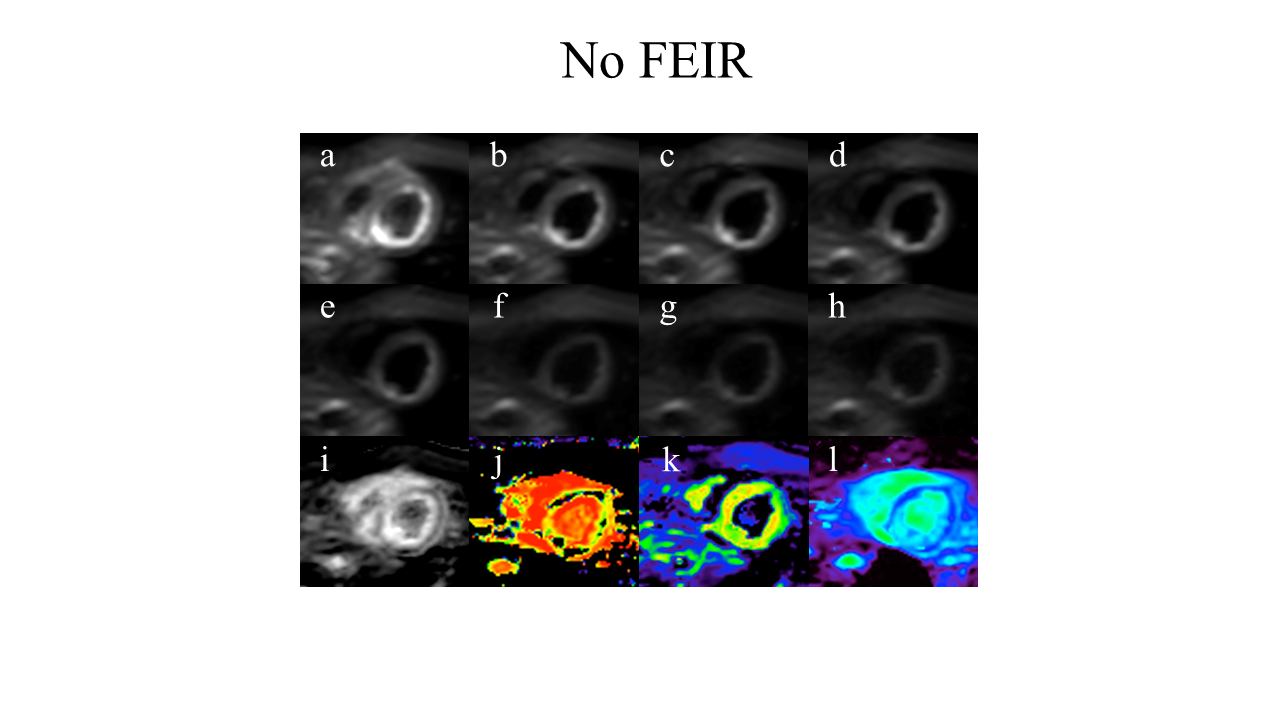
Figure
2. Example of conventional TSE-DWI(No FEIR) using MoCo-TSE-FEIR raw images of the mid-ventricular short axis
slices: b-value = 1,
20, 50, 100, 150, 200, 300, 500
s/mm2
(a-h) and calculated parametric
maps: ADC ( i ), D* ( j ), D( k ), and f ( l ) maps.
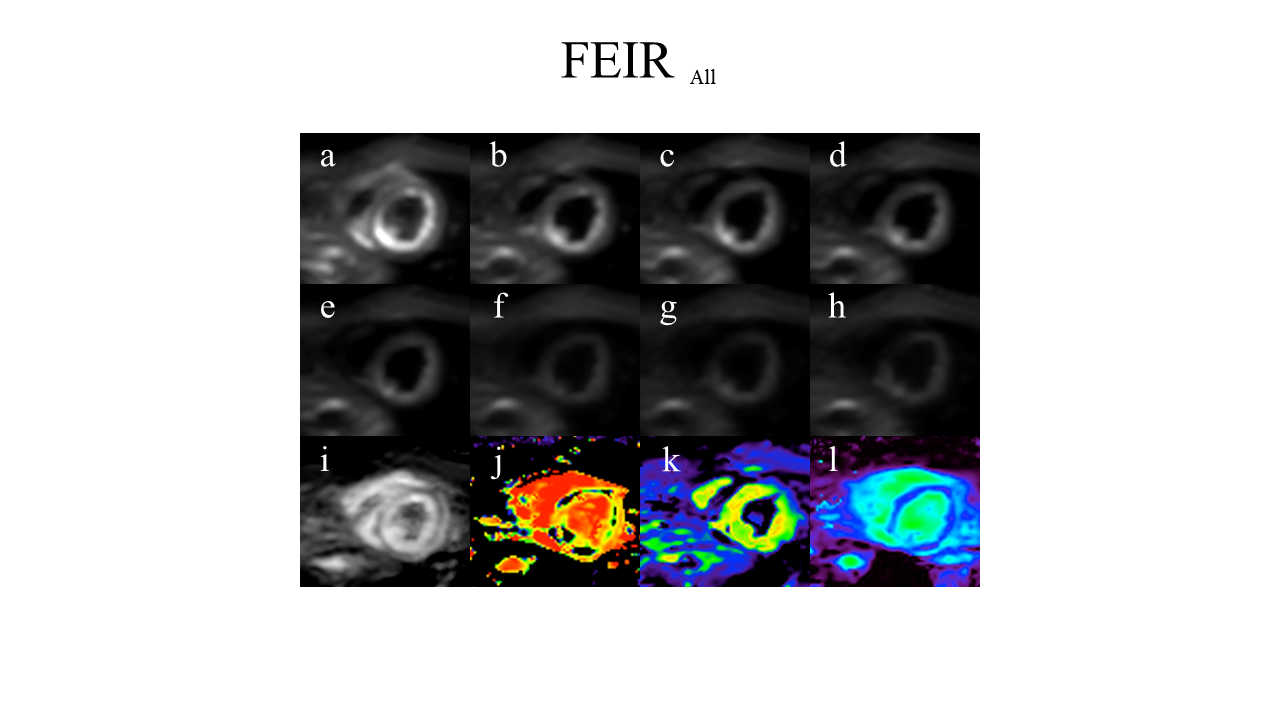
Figure
3. Example of IVIM-DWI using MoCo-TSE-FEIR raw images of the mid-ventricular short axis
slices: b-value = 1,
20, 50, 100, 150, 200, 300, 500
s/mm2
(a-h) and calculated parametric
maps: ADC ( i ), D* ( j ), D( k ), and f ( l ) maps.
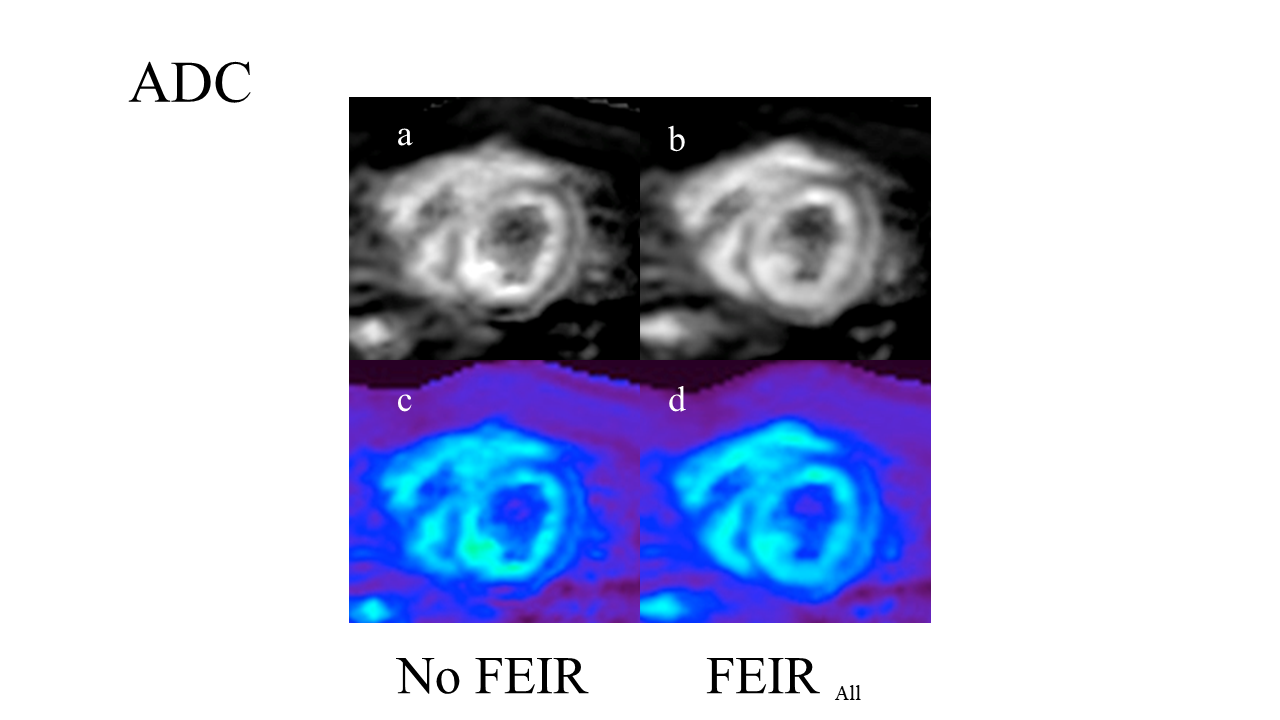
Figure
4. Results of MoCo-TSE-FEIR (FEIR All) and conventional TSE-DWI (NO
FEIR) for ADC map by one representative volunteer are shown. The signal
uniformity of the cardiac wall was improved with FEIR All as compared with No FEIR .
DOI: https://doi.org/10.58530/2022/4562