4555
Motion-resolved 4D Real-time Flow MRI1Institute of Science and Technology for Brain-Inspired Intelligence, Fudan University, Shanghai, China, 2University of Texas at Austin, Austin, TX, United States, 3Beijing PINS Medical Co., Ltd, Beijing, China, 4Department of Cardiology, Zhongshan hospital Fudan University, Shanghai, China, 5Philips Healthcare, Shanghai, China, 6Human Phenome Institute, Fudan, Shanghai, China
Synopsis
Conventional 4D flow MRI requires electrocardiogram gated cine acquisition and respiration control to measure flow dynamics associated with one synthetic cardiac cycle. This often leads to low acquisition efficiency and also cannot resolve beat-by-beat nor respiratory-related flow variations. This work presents a new 4D real-time flow MRI method which is able to simultaneously resolve respiratory and cardiac motion. Compared to conventional 4D flow MRI, the proposed method well captures the beat-by-beat flow variations and respiration-related flow dynamics. Its feasibility for aortic flow was demonstrated in several healthy subjects and also patients with atrial fibrillation.
Introduction
4D flow MRI enables comprehensive assessment of 3D hemodynamics, and has been applied in a number of clinical studies. Conventional 4D flow MRI techniques utilize electrocardiogram (ECG) gated cine acquisition, along with respiration control, to acquire time-resolved flow information that is corresponding to one synthetic cardiac cycle. This leads to low imaging efficiency, as irregular heart beating and respiration motion often cause data rejection in the acquisition process. Moreover, the cine-based approach prohibits measurements of beat-by-beat flow variations and also respiratory-resolved flow dynamics that could be of clinical interest in patients especially with cardiac arrythmia and/or cardiopulmonary diseases. In contrast, real-time flow imaging[1-3] is able to provide several promising advantages to address the above limitations. Recently, self-gated 5D flow methods[4-6] have been introduced to enable assessment of respiration-related flow dynamics. In this abstract, we present a subspace imaging approach to 4D real-time flow MRI, which simultaneously resolves cardiac and respiratory motion information. We validated the proposed method in an aortic flow application with both healthy subjects and patients with atrial fibrillation.Methods
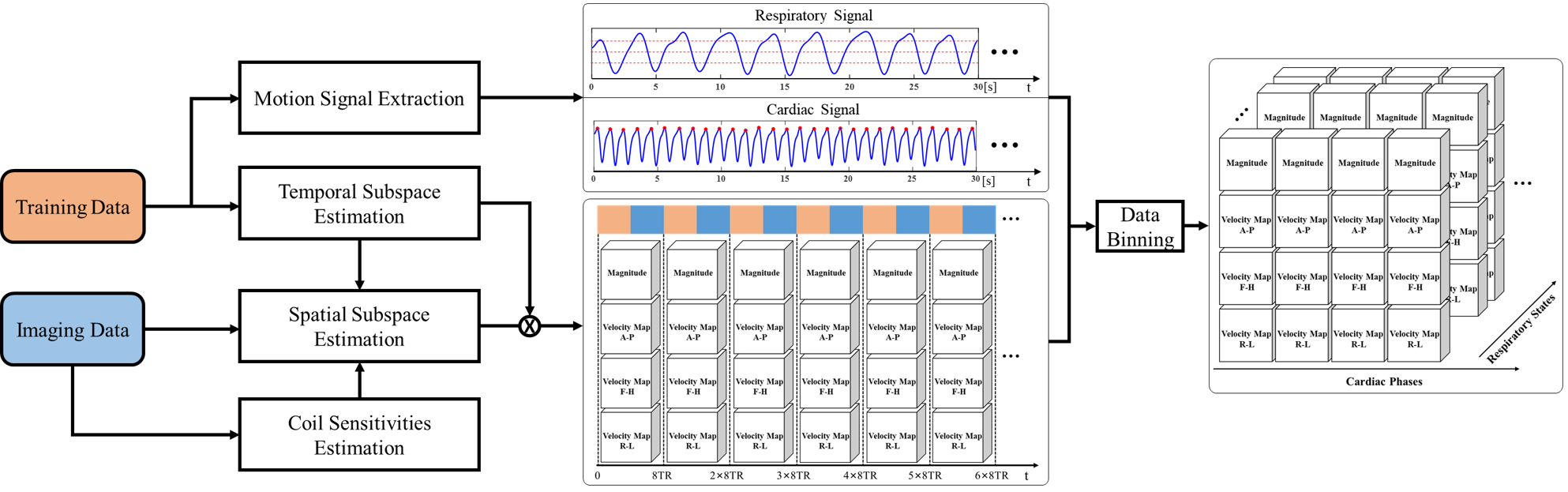
The proposed subspace imaging features with the following acquisition strategy: we acquire two sets of (k, t)-space data in a continuous and interleaved way: 1) a training data set acquired repeatedly from the k-space center with high temporal resolution, and 2) an imaging data set acquired in a random scheme from the outer k-space region with high spatial resolution. Specifically, the read-out of the k-space is placed along superior-inferior direction of the subject. Thus, the training data can be used to extract respiratory and cardiac motion signals via principal component analysis and coil channel clustering[7]. Meanwhile, a temporal subspace V can also be estimated from the same training data set using singular value decomposition. Then the continuously real-time flow images can be finally determined from the calculated V and a spatial subspace U derived based on a low-rank constrained image reconstruction[8]. Note that both the extracted motion signals and reconstructed flow images naturally share the same duration and temporal resolution (i.e. 8TR), which can be directly used to assess real-time flow dynamics with synchronized five-dimensional (i.e., x-y-z-cardiac-respiratory) information. To facilitate an explicit analysis of respiration effects on flow, we further distribute the reconstructed flow images into four respiratory states and appropriate cardiac phases based on extracted motion signals. Hence, a 5D flow image datasets corresponding to an averaged cardiac cycle and respiratory cycle can also be formulated. The data processing scheme is summarized in Fig. 1.For a proof-of-concept study, we recruited six healthy volunteers (6 males, age: 23-31 years old) and two patients with atrial fibrillation (2 males, age: 48 and 57 years old) in the imaging experiments of the aorta. All the imaging experiments were conducted at a 3.0 T whole body MR scanner (Ingenia, Philips Healthcare, Best, the Netherlands). For comparison, we also performed conventional 4D flow imaging with only retrospective ECG-synchronization and a standard 4D flow imaging with additional respiratory navigator gating for each healthy subject. The imaging parameters for all scans are as follows: spatial resolution = 2.4 × 2.4 × 2.4 mm, matrix size Nx=82±3/Ny=108/Nz=20±2, flip angle = 5°, repetition time/echo time = 4.3/2.5 ms, and encoding velocity = 200/150/150 cm/s (FH/AP/RL).
Results
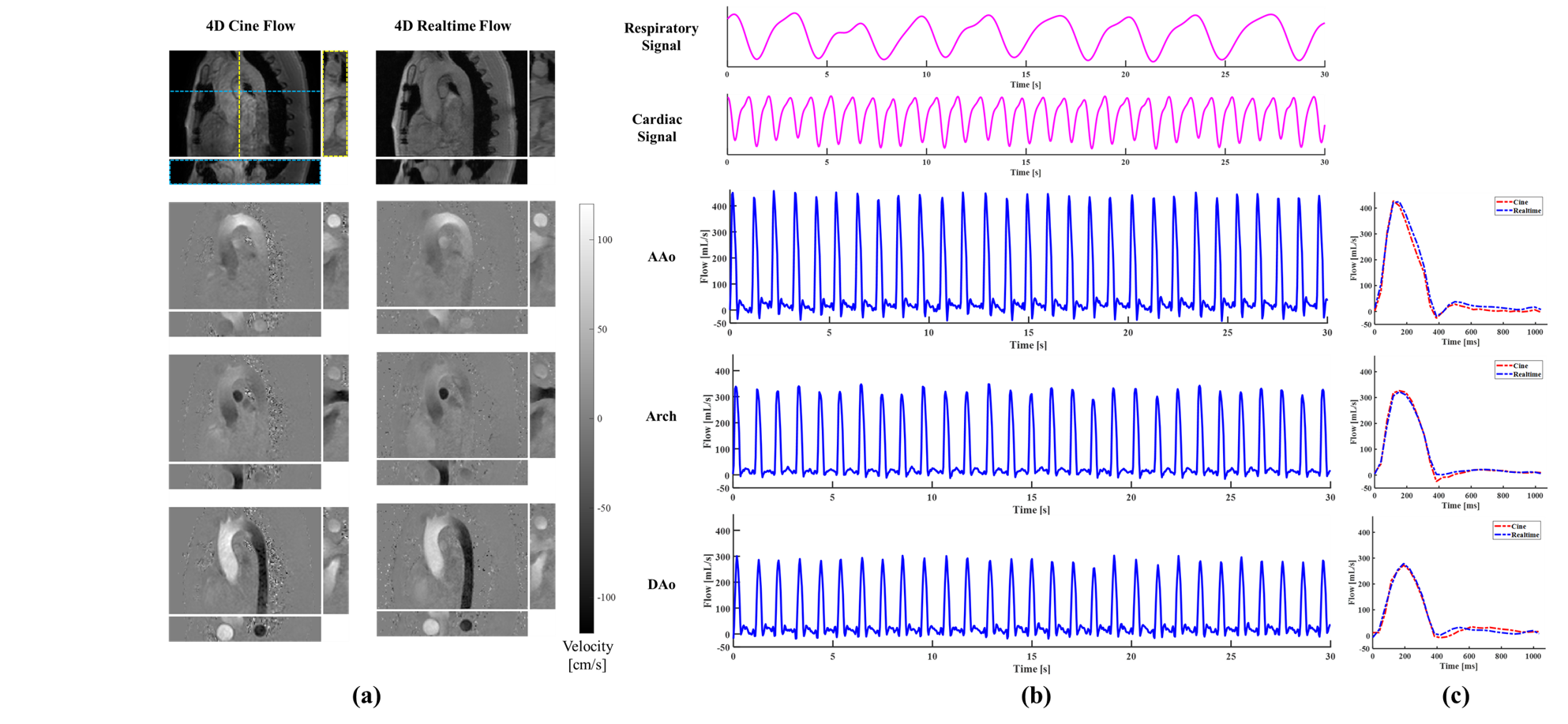
Fig.2(a) shows the magnitude images with three-directional velocity maps at a systolic phase for a healthy subject. As can be seen, the proposed method provides similar reconstruction quality to the conventional 4D flow imaging method. Fig.2(b) shows the flow waveforms associated with ascending aorta, aortic arch, and descending aorta, and the synchronous respiratory and cardiac motion signals during thirty seconds for the same subject. It is evident that the extracted cardiac motion signals and the reconstructed flow waveforms have the same periodicity. As is shown in Fig.2(c), the synthesized flow waveforms of one cardiac cycle averaged from the reconstructed real-time flow images well match those from the conventional cine imaging. Fig.3 shows the reconstructions for one patient with atrial fibrillation. It can be seen that the proposed method can well resolve the beat-by-beat pathological flow changes and respiratory and cardiac motion variations. Fig. 4 shows the reconstructed magnitude and velocity magnitude images with four respiratory bins for a healthy subject. The displacement of the aorta can be clearly seen to range from the end-expiration to end-inspiration. It is worth noting that the respiration-resolved flow variations can be observed from the velocity maps. Fig. 5 shows a Bland-Altman analysis of the peak velocities and net flow from the proposed method in the end-expiratory state versus those flow quantities obtained from conventional 4D flow imaging using respiratory-gating for all six healthy subjects. As can be seen, the flow quantities from the proposed method are in good agreement with those from cine flow imaging.Discussion and Conclusions
In this work, we presented the first demonstration of 4D real-time flow MRI with simultaneous respiratory and cardiac motion resolved. The proposed method is capable of measuring beat-by-beat flow variations as well as respiration-related flow dynamics. In the future work, it is useful to study its clinical utility for patients with various cardiac and cardiopulmonary diseases.Acknowledgements
This work was supported by the National Natural Science Foundation of China (No. 81971583), National Key R&D Program of China (No. 2018YFC1312900), Shanghai Natural Science Foundation (No. 20ZR1406400), Shanghai Municipal Science and Technology Major Project (No.2017SHZDZX01, No.2018SHZDZX01) and ZJLab.References
[1] Joseph AA, Kowallick JT, Merboldt KD, Voit D, Schaetz S, Zhang S, Sohns JM, Lotz J, Frahm J. Real-time flow MRI of the aorta at a resolution of 40 msec. J Magn Reson Imaging 2014;40(1):206-213.
[2] Traber J, Wurche L, Dieringer MA, Utz W, von Knobelsdorà-Brenkenhoà, F, Greiser A, Jin N, Schulz-Menger J. Real-time phase contrast magnetic resonance imaging for assessment of haemodynamics: from phantom to patients. Eur Radiol 2016;26(4):986-996.
[3] Haji-Valizadeh H, Feng L, Ma LE, Shen D, Block KT, Robinson JD, Markl M, Rigsby CK, Kim D. Highly accelerated, real-time phase-contrast MRI using radial k-space sampling and GROG-GRASP reconstruction: a feasibility study in pediatric patients with congenital heart disease. NMR Biomed 2020 May;33(5):e4240.
[4] Cheng JY, Zhang T, Alley MT, Uecker M, Lustig M, Pauly JM, Vasanawala SS. Comprehensive multi-dimensional MRI for the simultaneous assessment of cardiopulmonary anatomy and physiology. Sci Rep 2017 Jul 13;7(1):5330.
[5] Walheim J, Dillinger H, Kozerke S. Multipoint 5D flow cardiovascular magnetic resonance - accelerated cardiac- and respiratory-motion resolved mapping of mean and turbulent velocities. J Cardiovasc Magn Reson 2019 Jul 22;21(1):42.
[6] Ma LE, Yerly J, Piccini D, Di Sopra L, Roy CW, Carr JC, Rigsby CK, Kim D, Stuber M, Markl M. 5D flow MRI: A fully self-gated, free-running framework for cardiac and respiratory motion-resolved 3D hemodynamics. Radiol Cardiothorac Imaging 2020 Nov 12;2(6):e200219.
[7] Zhang T, Cheng JY, Chen Y, Nishimura DG, Pauly JM, Vasanawala SS. Robust self-navigated body MRI using dense coil arrays. Magn Reson Med 2016;76:197–205.
[8] Sun A, Zhao B, Li Y, He Q, Li R, Yuan C. Real-time phase-contrast flow cardiovascular magnetic resonance with low-rank modeling and parallel imaging. J Cardiovasc Magn Reson 2017 Feb 10;19(1):19.
Figures