4554
Clinical application of 3.0T whole-heart non-contrast agent MRCA by using Compressed SENSE1Fuyang People's Hospital, fuyang, China, 2Fuyang People's Hospital, FuYang, China, 3the First Affiliated Hospital of Anhui Medical University, hefei, China
Synopsis
MR Coronary angiography (MRCA) technology can observe the anatomical morphology of coronary arteries and detect lumen stenosis, dilation, and abnormal wall lesions [1]. MRCA technology is relatively complex with long scanning time [2]. Compressed SENSE (CS) technology can greatly shorten the scanning time and improve the rate of succussed examination. This study aim to explore the clinical feasibility of Compressed SENSE technology in non-contrast agent MRA and explore the best acceleration factor of CS.
Introduction
Whole heart, non-contrast agent coronary angiography (MRCA) with long scanning time is a major obstacle for clinical examination. Compressed SENSE technique has been widely used in clinical examinations. Meanwhile, it can ensure the quality of the image and reduce the scanning time significantly.[3] The aim of this study was to explore the feasibility of the whole heart non-contrast MRCA based on compressed SENSE technology and explore the best accelerator factors for clinical and research use.Materials and Methods:
This study was approved by the Institutional Review Board and all participants signed written informed consent. Patients who had completed coronary artery CTA (CCTA) examination in our hospital were underwent whole-heart non-contrast coronary magnetic resonance angiography on 3.0T MR scanner (Ingenia CX, Philips, Netherland) All patients were suspected for acute coronary syndrome. They received four different scanning sequences: Conventional sequence SENSE2 (S2), the other three groups of sequences used compressed SENSE technology, acceleration factors were 4, 5, 6 (CS4, CS5, CS6). The S2 was considered as the control sequence and CCTA images were taken as the gold standard. Subjective image quality was scored by two experienced doctors and the scoring was based on a four-point system: (1) 4 points, clear vascular display, sharp lumen boundary; (2) At 3 minutes, the vascular display was sufficient and the lumen boundary was slightly blurred; (3) 2 marks, vascular visible, lumen boundary blurred, affecting lumen evaluation; (4) 1 point, the artifact was severe, and the lumen could not be evaluated or visible. The image quality score ≥3 was considered as good image quality and high diagnostic reliability. The image with a score of 1 was difficult to diagnose. The signal contrast CR value was measured and calculated, and the vessel with a score of 1 was abandoned,Record the CR of each segment, CR=(μvessel-μmyocardium)/[(σvessel2-σ myocardium2)-2], μ is the average signal intensity of the corresponding tissue, and σ is the variance of the corresponding tissue.The image quality of different segments of coronary arteries were compared among the four sequences.Results
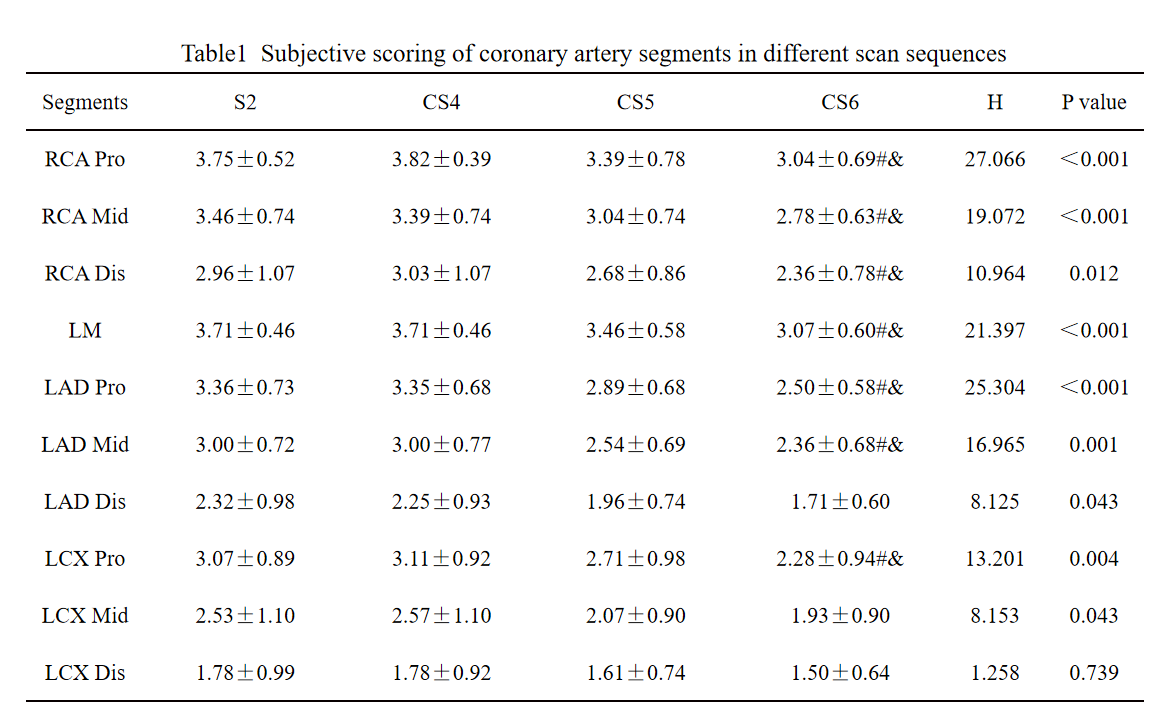
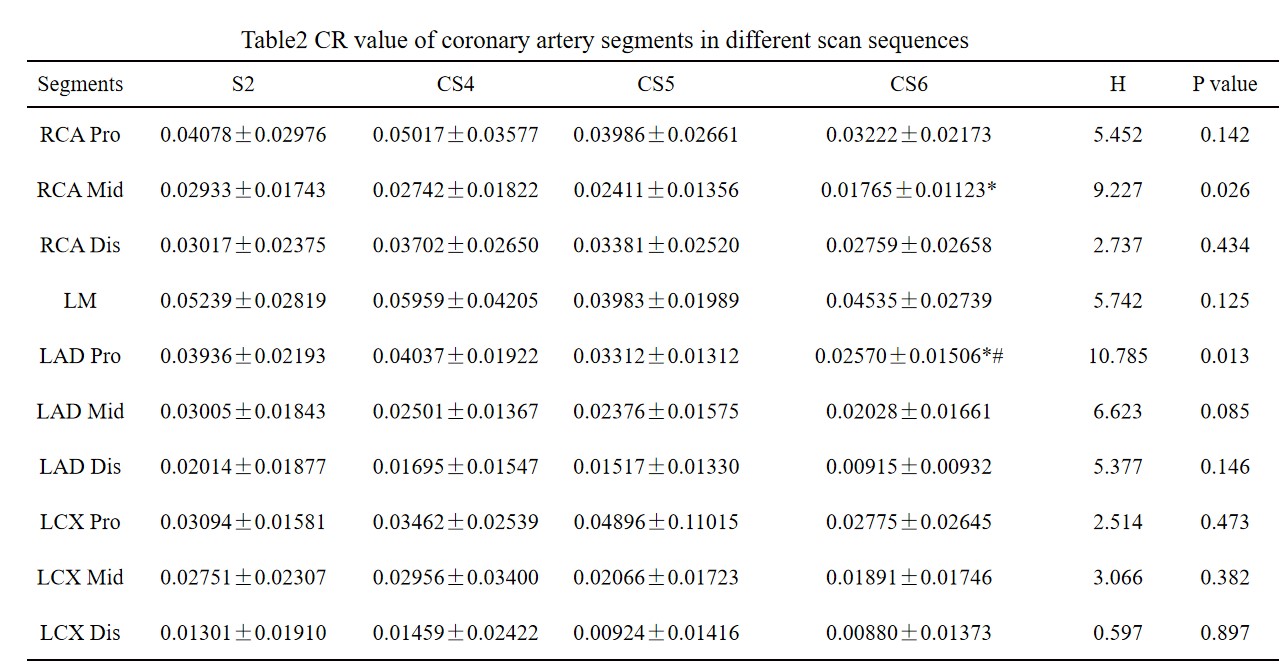
Twenty-eight patients were included in this study, and the subjective scored of image quality were 4 points with 294 segments, 3 points with 414 segments, 2 points with 246 segments, and 1 point with 166 segments. There were statistically significant differences in the subjective scores of each segment of coronary artery among groups S2, CS4, CS5 and CS6 except for the distal segment of LCX (P < 0.05). Further pin-wise comparison showed that the subjective scores of each segment of CS6 group were lower than those of S2 and CS4 group (P < 0.05)(Table 1). There were statistically significant differences in CR values between S2, CS4, CS5 and CS6 coronary artery segments in middle RCA and near LAD (P < 0.05), but there were no statistically significant differences in other segments (P > 0.05). Further pairwise comparison showed that the CR value of CS6 group was lower than S2 group (P < 0.05). The CR value of CS6 group was lower than S2 group and CS4 group (P < 0.05)(Table 2). CS4 and CS5 had no statistical difference in image quality compared with S2, and Compared with S2 and CS4, CS6 had statistically significant difference.The average scanning time of each sequence is 344.10±47.39, 270.36±37.07, 215.18±30.39 180.39±25.06, and the CS5 and S2 are shorter than the time by about 37.5%.Conclusion
Compressed SENSE technology can shorten the examination time ensuring the image quality. When the acceleration factor is 5, the time is obviously shortened and the image quality can be used in clinical practice.Acknowledgements
No acknowledgement found.References
[1]Sakuma H.Coronary CT versus MR angiography:the role of MR angiography.Radiology.2011:258(2):340—349. [2]Anderson JL, Adams CD, Antman EM et al (2013) 2012 ACCF/ AHA focused update incorporated into the ACCF/AHA 2007 guidelines for the management of patients with unstable angina/ non-ST-elevation myocardial infarction: a report of the american college of cardiology foundation/American heart association task force on practice guidelines. J Am Coll Cardiol 61:e179–e347[3]Jaspan ON,F1eysher R,Lipton ML.Compressed sensing MRI:a review of the clinical 1iterature.The British journal of radiology.2015:88(1056):20150487.Figures
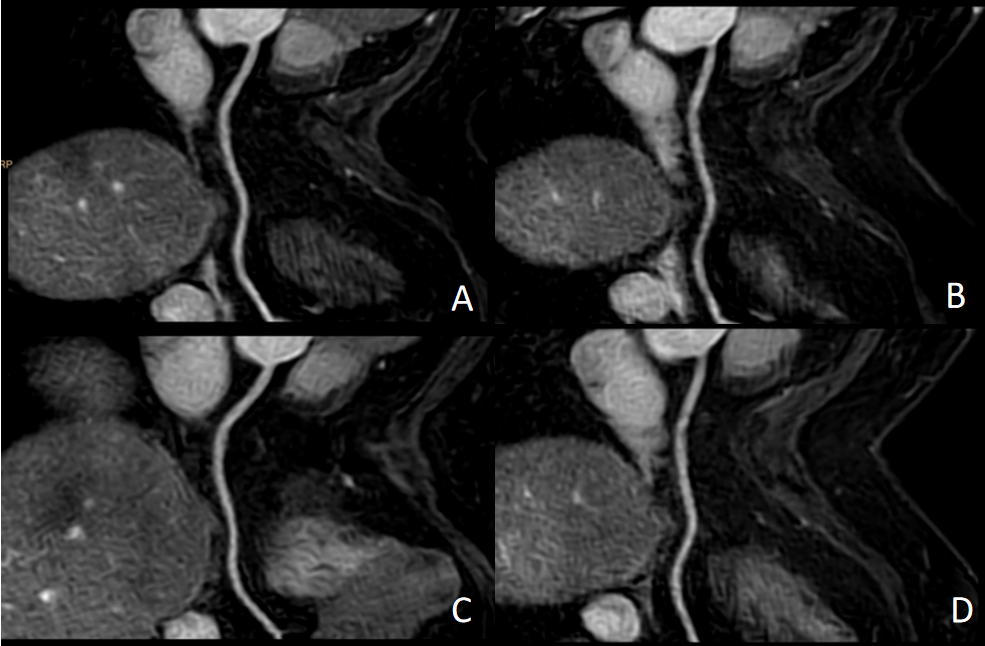
Fig.1 3.0T whole-heart CMRA without contrast in a 51-year-old woman.
A: S2 sequence with subjective score of 4 in the proximal and distal segments and rough tube wall in the middle segment.
B: CS4 sequence, with a subjective score of 4 in the proximal segment and rough tube wall in the middle and distal segments.
C:CS5 sequence. The subjective score of the proximal and distal segments is 4 points, and the middle segment is rough and the middle segment is rough.
D: CS6 sequence, with a subjective score of 4 in the proximal segment and rough tube wall in the middle and distal segments.