4552
The Value of Free-breathing 4D-Flow MRI in Children with Extrahepatic Portal Venous Obstruction: A Preliminary Study1Radiology, Guangzhou Women and Children’s Medical Center, Guangzhou, China, 2Pediatric Surgery, Guangzhou Women and Children’s Medical Center, Guangzhou, China, 3MR Scientific Marketing, Siemens Healthineers, Guangzhou, China
Synopsis
This preliminary study has investigated the feasibility of free-breathing 4D-flow MRI to evaluate portal hemodynamics in children with EHPVO. Free-breathing 4D-flow MRI is feasible and hopeful for the comprehensive 3D visualization and quantification of portal vein flow dynamics in 14 children and the peak velocity had similar diagnostic efficiency to ultrasound in our study. In the future, we intend to compare 4D-flow parameters with intraoperative manometry of the portal vein system and use the noninvasive radionics methodology to estimate portal vein hemodynamics in children.
Purpose
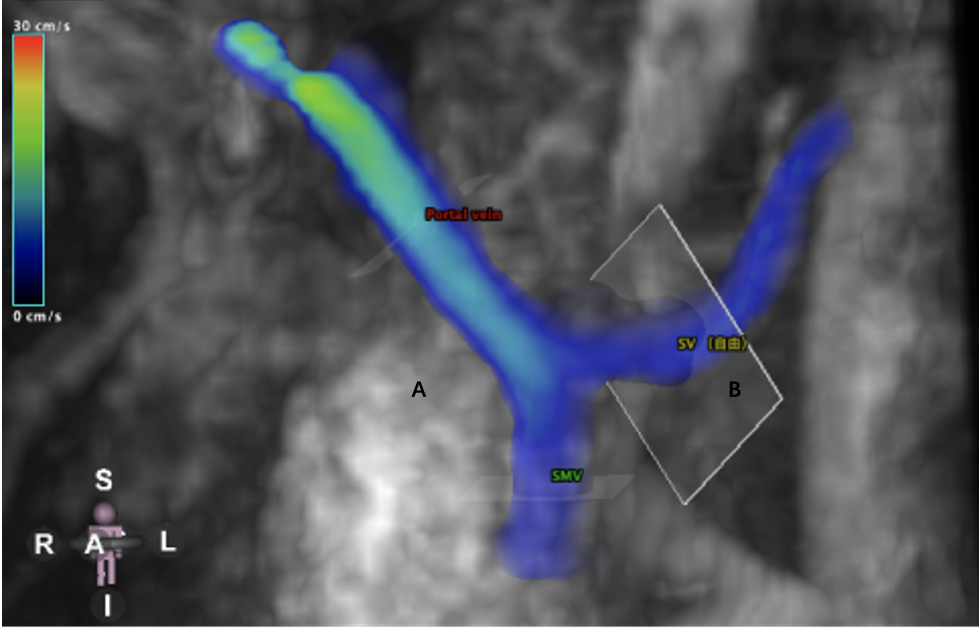
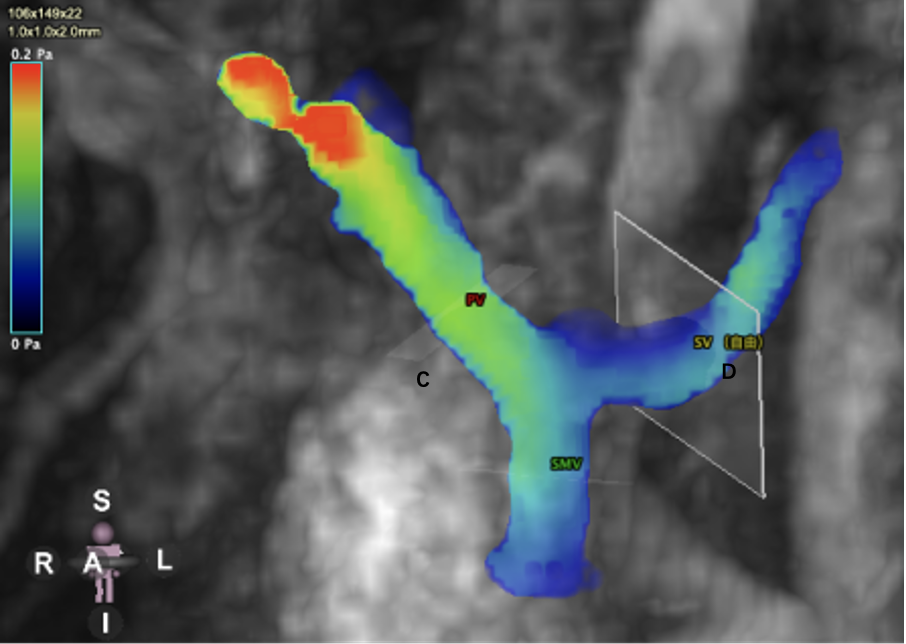
Extrahepatic portal vein obstruction (EHPVO) was defined as thrombosis of the extrahepatic portal vein (PV) [1]. It was usually considered as the cause of portal hypertension in 70% of pediatric patients and the most common reason for upper gastrointestinal bleeding in children [2, 3]. We had already studied the CT value of children with EHPVO [4]. With the clinical application of new MRI technologies, 4D-flow analysis already had some outstanding performance in the cardiovascular system. Unlike traditional 2D flow analysis, 4D-Flow velocity coding is carried out in three spatial directions, so that we can analyze hemodynamics refer to wall shear stress (WSS), pulse wave velocity (PWV), kinetic energy, turbulent kinetic energy (TKE), vorticity, pressure gradient, and flow component analysis all kind of parameters anywhere in the acquisition area. Since most of EHPVO occurs in childhood and children can't hold their breath. In this study, we tried to prospectively apply free-breathing 4D-flow MRI on the portal venous system [5-9], evaluate the portal vein hemodynamics in children, and compare with the results of the ultrasound.Methods
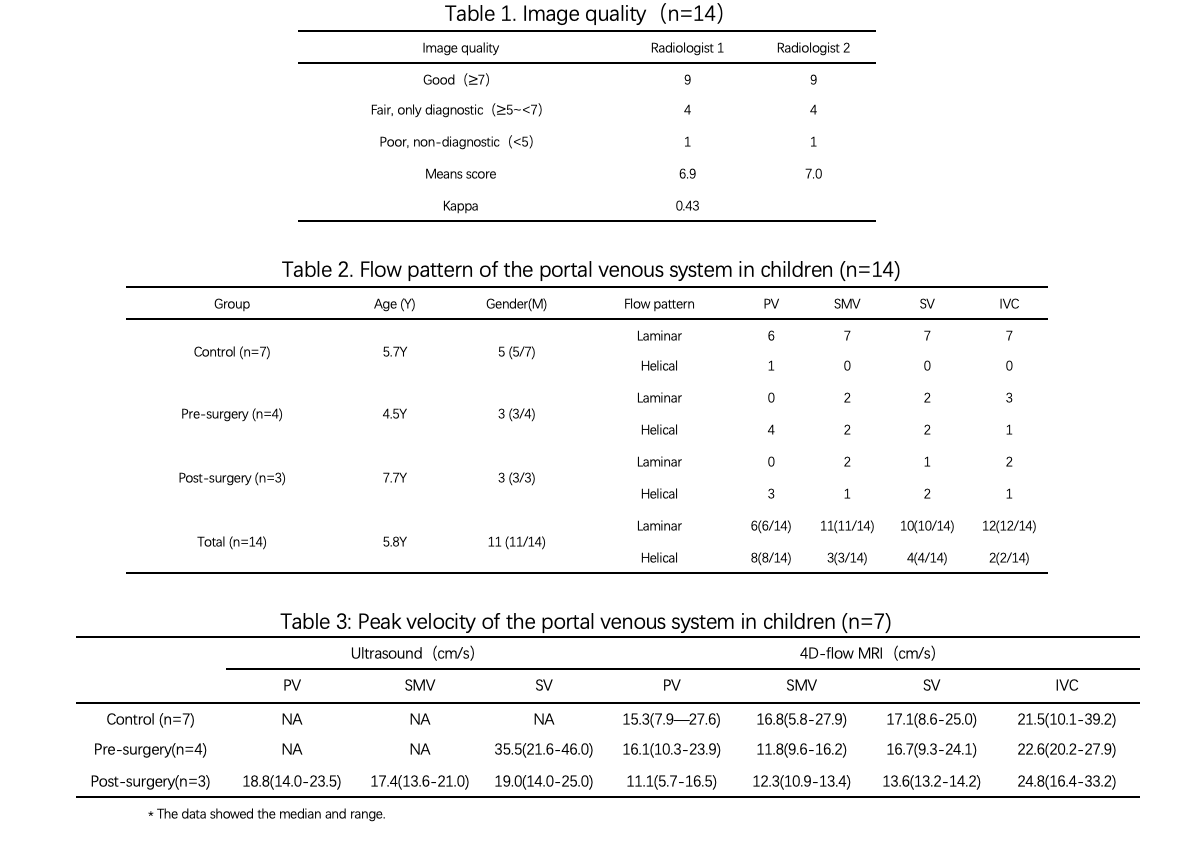
4D-flow MRI was performed on 14 children (median age: 5.8 years old; range: 1.2-14 years old) with 7 cases as the non-operated control group, 4 cases as pre-Rex surgery group, and 3 cases as post-Rex surgery group. Morphological T2W imaging was acquired using a true fast image with steady-state precession (True-FISP) sequence on a 3.0T system (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany). 4D-flow protocols were as following: TR/TE = 46/3.23ms; flip angle = 7deg; FOV = 320×256mm2; scan matrix = 112×107.2; voxel size = 2.0×2.0×2.5mm3; slice number = 26; parallel imaging factor = 2; VENC = 80cm/s [5]; GRAPPA was used to reduce scanning time and retrospective ECG gating was used to perform scanning under free-breathing. All 4D-flow data were reconstructed in CVI 4.2(Circle, Calgary, Ontario, Canada). 4D visualization was independently assessed the diagnostic image quality of 4D imaging by two radiologists. The image quality was graded based on a three-point Likert scale (<5: poor, non-diagnostic; 5-7: fair, diagnostic; >7: good). Children with EHPVO pre- and post-Rex surgery were performed ultrasound 2-3 days later. Flow patterns were defined for the portal (PV), superior mesenteric (SMV), splenic veins (SV), and inferior vena cava (IVC) of all patients. Image quality assessment for 4D-flow visualization and flow pattern analysis was performed. Quantitative parameters of the 4D-flow technique such as regional peak velocity and net flow volume were compared with ultrasound parameters. Agreement of 4D-flow image quality between the ratings of two radiologists was derived using a weighted κ test (poor agreement: κ < 0.2; fair agreement: 0.2 < κ < 0.4 moderate agreement: 0.4<κ<0.6; good agreement: 0.6<κ<0.8; very good agreement: 0.8<κ<1) [10].Results
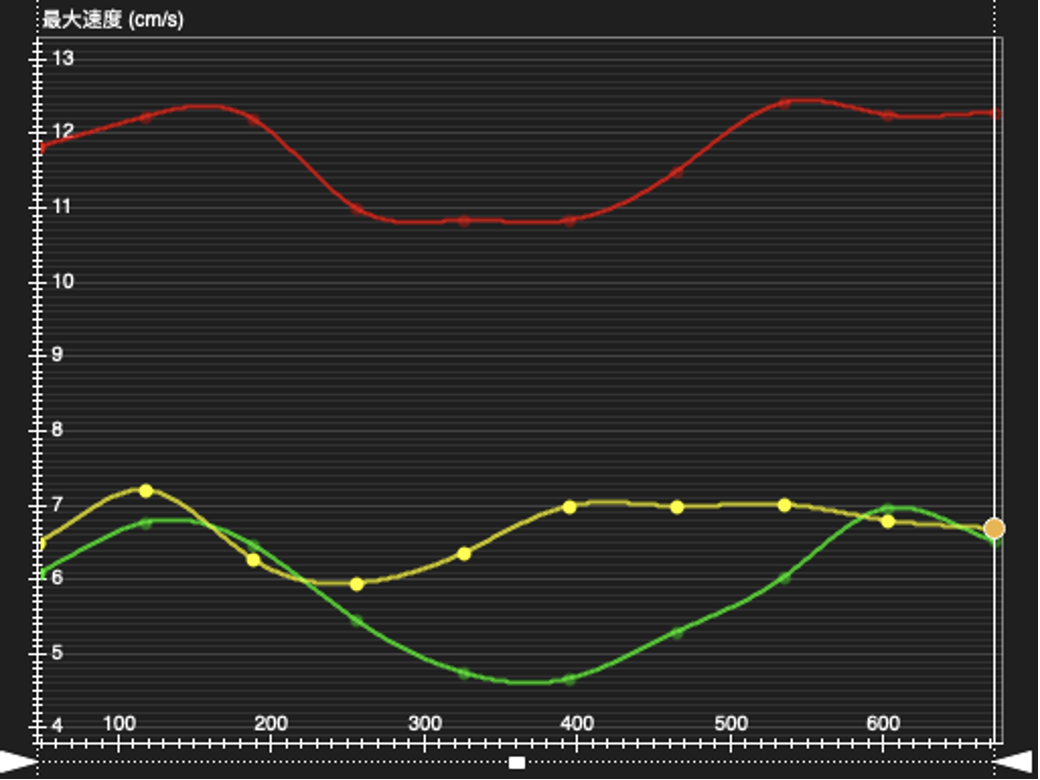
The mean score of 4D-Flow visualization imaging quality was excellent (mean ± SD = 6.9±1.6) with the good inter-observer agreement (κ = 0.43, P = 0.02). Flow patterns of 4D-Flow visualization were analyzed for control, pre-surgery, and post-surgery groups. 7 cases of the control group were laminar patterns in PV, SMV, SV, and IVC, and only 1 case was found with the helical pattern. More helical pattern was found in the pre-surgery group. Quantitative means of peak velocity of PV, SMV, SV, and IVC were 19.7cm/s, 12.3cm/s, 21.6cm/s and 23.6cm/s in pre-surgery group, and 16.1cm/s, 11.8cm/s, 16.7cm/s and 16.4cm/s in post-surgery group, respectively. Ultrasound peak velocity of PV and SMV could not perform in the pre-surgery group, but SP’s mean peak velocity was 35.5 ml/s. The means of peak velocity of PV, SMV, SV were 18.8cm/s, 17.4cm/s and 19.0cm/s in ultrasound post-surgery group, respectively.Discussion
4D-Flow visualization imaging quality score was little lower than Parekh [5], maybe because some of the children were performed MRI without holding breath and the intrahepatic portal vein was not shown apparently. However, 4D-Flow images were good enough to evaluate the extrahepatic portal vein’s hemodynamics in children, which was hard to analyze in traditional MRI. It was difficult to display the superior mesenteric vein in children before Rex surgery, and 4D flow MRI could solve this problem. According to the results, the net flow and peak velocity had good consistency with ultrasound parameters. We also measured the pressure gradient and wall shear stress (WSS) of PV and SMV. In the future, we intend to compare 4D flow MRI parameters with intraoperative manometry and use imaging omics to estimate noninvasive portal vein pressure in children.Conclusion
4D flow MRI is feasible and promised for comprehensive 3D visualization and quantification of portal venous hemodynamics in children and the results had good consistency with ultrasound.Funding
This study was funded by Guangdong Medical Science and Technology Research Foundation, China (Grant number A2021261).Acknowledgements
We sincerely thank the participants in this study.References
1、 de Ville de Goyet J, D’Ambrosio G, Grimaldi C (2012) Surgical management of portal hypertension in children. Semin Pediatr Surg 21(3):219–232.
2、Sarin SK, Sollano JD, Chawla YK, et al (2006) Consensus on extra-hepatic portal vein obstruction. Liver Int 26:512–519.
3、Yachha SK, Khanduri A, Sharma BC, et al (1996) Gastrointestinal bleeding in children. J Gastroenterol Hepatol 11:903–907.
4、Wu H, Zhou N, Lu L, et al. Value of preoperative computed tomography for meso-Rex bypass in children with extrahepatic portal vein obstruction[J]. Insights into Imaging, 2021, 12(1): 1-12.
5、Parekh, K., Markl, M., Rose, M., Schnell, S., Popescu, A., & Rigsby, C. K. (2017). 4D flow MR imaging of the portal venous system: a feasibility study in children. European radiology, 27(2), 832-840.
6、Motosugi, U., Roldán-Alzate, A., Bannas, P., Said, A., Kelly, S., Zea, R., … & Reeder, S. B. (2019). Four-dimensional flow MRI as a marker for risk stratification of gastroesophageal varices in patients with liver cirrhosis. Radiology, 290(1), 101-107.
7、Hyodo, R., Takehara, Y., Mizuno, T., Ichikawa, K., Ogura, Y., & Naganawa, S. (2021). Portal vein stenosis following liver transplantation was hemodynamically assessed with 4D-flow MRI before and after portal vein stenting. Magnetic Resonance in Medical Sciences, 20(3), 231.
8、Haarbye, S. O., Nielsen, M. B., Hansen, A. E., & Lauridsen, C. A. (2021). Four-Dimensional Flow MRI of Abdominal Veins: A Systematic Review. Diagnostics, 11(5), 767.
9、 Bane, O., Peti, S., Wagner, M., Hectors, S., Dyvorne, H., Markl, M., & Taouli, B. (2019). Hemodynamic measurements with an abdominal 4D flow MRI sequence with spiral sampling and compressed sensing in patients with chronic liver disease. Journal of Magnetic Resonance Imaging, 49(4), 994-1005.
10、 Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174.
Figures