4550
Assessment of compressed sensing accelerated non-contrast-enhanced whole-heart coronary MR angiography at 3.0 T1MRI, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 2Philips Healthcare, Beijing, China
Synopsis
The feasibility of non-contrast-enhanced coronary MR angiography (CMRA) with acceleration by compressed sensing (CS) was assessed in patients with suspected coronary artery diseases on a 3.0 T scanner, compared with conventional coronary MRA. Results indicate that the whole-heart non-contrast CMRA accelerated by CS with a factor of 4 obtained relatively high sensitivity, positive predictive value, negative predictive value and accuracy in a significantly shortened acquisition time compared with conventional CMRA.
introduction
Coronary artery disease (CAD) is the most common type of heart disease leading the mortality worldwide (1). Coronary MR angiography (CMRA) has emerged over the past decade as a possible noninvasive and radiation-free technique for visualizing coronary arteries (2). In comparison with coronary computed tomography angiography (CCTA), which has proven to be highly accurate for noninvasive detecting coronary artery stenosis, CMRA still has its unique advantage. In addition to detailed evaluation of coronary vessels, CMRA allows a more comprehensive assessment of the heart, including the assessment of coronary anomalies and aneurysms, interrogation of coronary bypass grafts, soft tissue characterization, viability assessment, coronary vein imaging, and identification of arterial wall abnormalities (3). Moreover, CMRA is not affected by the blooming artifacts from calcification in CCTA. Nevertheless, the utility of CMRA is hampered by the long acquisition times, which may increase the chance of heart rate (HR) variations, respiratory pattern drift, and bulk motion, and all degrade the final image quality. Shortening of CMRA acquisition times has been possible using a parallel imaging technique such as sensitivity encoding (SENSE) (4). Besides, the novel mathematical theory of compressed sensing (CS) has also been applied in MRI (5). The purpose of this study was to investigate the feasibility of non-contrast-enhanced CS coronary MRA with a 3.0 T scanner in patients with suspected CAD compared with conventional coronary MRA with acceleration by SENSE.Methods
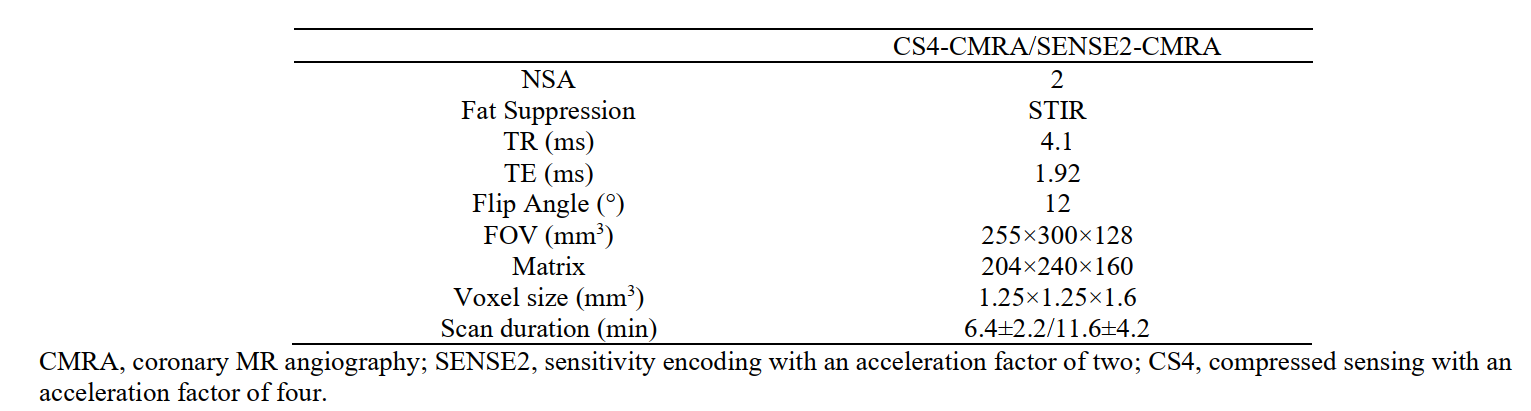
52 patients with suspected coronary artery disease (CAD) were prospectively enrolled in the study, aged 45±16 years, including 28 males. All patients completed two CMRA scans on a 3.0T MR scanner (Ingenia CX, Philips Healthcare, Best, the Netherlands) with acceleration by a CS factor of 4 (CS4-CMRA) and a SENSE factor of 2 (SENSE2-CMRA), respectively. Among them, 17 patients completed coronary computed tomography angiography (CCTA).For MR scans, after the survey scan, a balanced steady-state free-precession (SSFP) cine sequence with retrospective electrocardiography (ECG) triggering was acquired in a 4-chamber view during free breathing to observe a stagnation time of coronary artery and to determine the optimal data acquisition window length. A non-contract enhanced 3D spoiled gradient echo sequence was used with ECG-gating, diaphragm navigator-gating, and fat suppression for coronary MRA data acquisition with detailed imaging parameters listed in (Table 1).
CCTA was conducted on a 128-slice dual-source CT scanner (SOMATOM Force, Siemens Healthcare, Germany). The following acquisition parameters were used: tube voltage, 120 kV; automatic mA (260-300 mA) technology is used for tube current; pitch 0.8 mm; time resolution: 66.0 ms; detector collimation: 2.0 x 192 × 0.6 mm3; gantry rotation time, 0.25 second; field of view, 200-250 mm; and matrix, 512 × 512; and section thickness, 1.25 mm. All CCTA scans were acquired by a prospective ECG triggered axial scan mode. The contrast medium (ioversol, 370 mg/mL) was intravenously injected through an 18-gauge intravenous antecubital catheter at a flow rate of 5 to 6 mL/s followed by 75 mL of contrast medium and saline mixed solution, and then 25mL of saline solution.
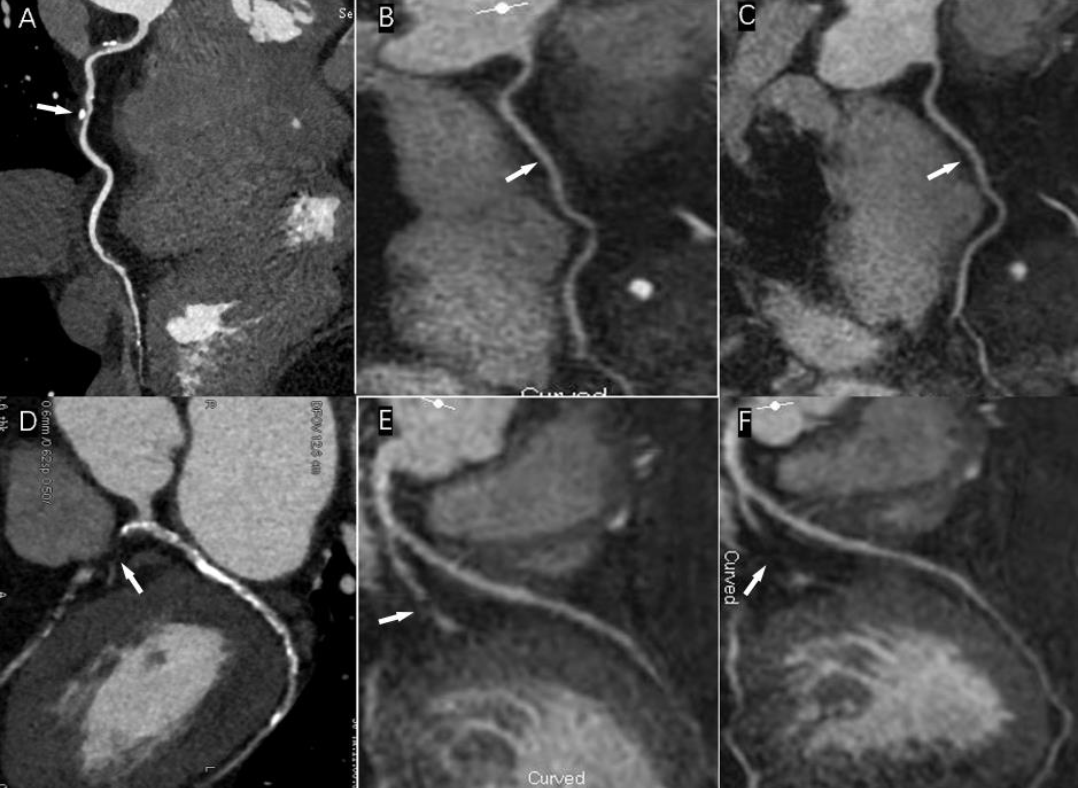
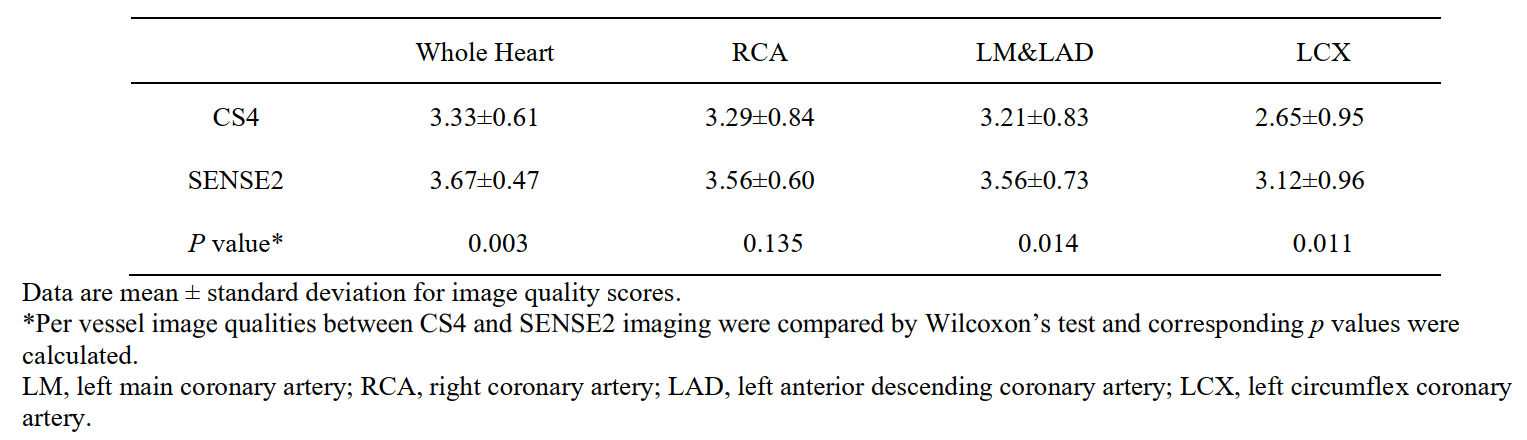
All CCTA and CMRA data were transferred to a workstation (IntelliSpace Portal v9.0; Philips Healthcare) for image reconstruction and subjective evaluation. The CMRA images were visually assessed independently by two radiologists who were blinded to the CCTA results and patient information. Stenosis with diameter reduction ≥50% was defined as clinically-relevant stenosis. Image for visualization of the three sets of arteries (1. left main and left anterior descending arteries, LM&LAD; 2. right coronary artery, RCA; and 3. left circumflex artery, LCX) was assessed with a four-point scoring scale: 1 = non-assessable with severe image artifacts, poor vessel contrast; 2 = assessable with moderate image artifacts, fair vessel contrast; 3 = assessable with minor artifacts, good vessel contrast; and 4 = assessable with no apparent artifacts, excellent vessel contrast. Overall image quality of whole-heart CMRA was calculated on the basis of all visible coronary segments.
Wilcoxon matched-pairs signed-rank tests were used to compare image quality between the two methods. The diagnostic performance of CMRA for the detection of significant coronary artery stenosis (sensitivity, specificity, PPV, NPV, accuracy, and area under ROC curve) was calculated using CCTA as the standard reference.
Results
The mean scan time of 52 patients with CS4 and SENSE2 whole-heart non-contrast CMRA were 6.4±2.2 and 11.6±4.2 min, respectively (p<0.001). Compared to SENSE2-CMRA, visualization of coronary arteries (including LCX and LM&LAD) was significantly degenerated in images by CS4-CMRA (Table 2). While with results by CCTA as references, the sensitivity, specificity, positive predictive value, negative predictive value and diagnostic accuracy (70.6%, 88.2%, 75.0%, 85.7% and 82.4%) for CS4-CMRA were all higher than those (64.7%, 88.2%, 73.3%, 83.3% and 80.3%) for SENSE2-CMRA (Table 3). The areas under the ROC curve of CS4-CMRA were also significantly higher than that of SENSE2-CMRA (0.794/0.765) for diagnosis of coronary artery stenosis at the vessel level (Table 3).Discussion and conclusion
CS4 whole-heart non-contrast CMRA obtained relatively high sensitivity, positive predictive value, negative predictive value and accuracy in a relatively short acquisition time compared with SENSE2 CMRA. CS4 whole-heart non-contrast CMRA may serve as a rapid, non-invasive, and no ionizing radiation magnetic resonance imaging technique for clinical evaluation of CAD.Acknowledgements
No acknowledgement foundReferences
1. Mozaffarian D, Benjamin EJ, Go AS. Heart disease and stroke statistics-2015 update: a report from the American Heart Association. Circulation 2015; 131(4). e29-e322.
2. Schuijf JD, Bax JJ, Shaw LJ. Meta-analysis of comparative diagnostic performance of magnetic resonance imaging and multi slice computed tomography for noninvasive coronary angiography. Am Heart J 2005; 151(2):404–411.
3. Kato S, Kitagawa K, Ishida N et al Assessment of coronary artery disease using magnetic resonance coronary angiography: a national multicenter trial. J Am Coll Cardiol 2010; 56:983–991.
4. Yang Q, Li KC, Liu X. 3.0T whole-heart coronary magnetic resonance angiography performed with 32-channel cardiac coils: a single-center experience. Circ Cardiovasc Imaging 2012; 5(5):573–579.
5. Nakamura M, Kido T, Kido T. Non-contrast compressed sensing whole heart coronary magnetic resonance angiography at 3T: A comparison with conventional imaging. Eur J Radiol 2018; 104:43–48.
Figures