4549
Aneurysmal wall enhancement is positively correlated with inflow angle in sidewall aneurysms1Department of Biomedical Engineering, Tsinghua University, Center for Biomedical Imaging Research, Beijing, China, 2Department of Interventional Neuroradiology, Beijing Tiantan Hospital, Beijing, China
Synopsis
In this study, we utilized HR-VWI and 3D TOF-MRA images to investigate the relationship between AWE grades and aneurysm inflow angle. Statistics indicated that the AWE grades were positively associated with the aneurysm inflow angle. This is probably because a sidewall aneurysm with high inflow angle is easier to grow and cause slower inflow velocity and lower wall shear stress which contribute to inflammation processes on aneurysmal wall and lead to a high grade of AWE. The results of this study showed that the AWE was positively associated with aneurysm inflow angle.
Introduction
Intracranial aneurysms are local bugles on the wall of intracranial artery with an estimated prevalence of nearly 2% - 5% in the whole world.[1,2] Due to the risk of rupture which could lead to disability even death, a great attention should give to intracranial aneurysms to avoid rupture. Histopathological evidences have suggested that inflammation was a key mediator in the formation, growth and rupture of aneurysms.[3] Moreover, it was reported that morphological parameters including inflow angle could influence the inflammation processes in sidewall aneurysmal wall.[4] However, the relationship between morphological parameters like inflow angle and inflammation processes remained unclear.Recently, aneurysmal wall enhancement (AWE) in high-resolution magnetic resonance vessel wall imaging has been used as the biomarker to assess the aneurysm wall inflammation.[5] Generally, 3D time-of-flight magnetic resonance angiography (3D TOF-MRA) images were utilized to quantify the morphology of aneurysms. So in this study, HR-VWI and 3D TOF-MRA images were used to investigate the relationship between AWE and aneurysm inflow angle.
Methods
Study Population:A total of 54 patients (15 males and 39 females, age range: 16 ~ 73 years) harbored with 59 aneurysms who were performed HR-VWI and 3D TOF-MRA were included in this study. Written informed consents were obtained from all patients.
MR Experiments:
MRI sequences including 3D black-blood T1-weighted volumetric isotropic turbo spin echo acquisition (T1-VISTA) and TOF-MRA were performed on a 3.0T MRI scanner (Philips Achieva, Best, Netherlands) with a 32-channel head coil. The imaging parameters for pre- and post-contrast T1-VISTA were as follows: TR/TE = 800/21 ms, FOV = 200 x 180 x 40 mm3, voxel size = 0.6 x 0.6 x 0.6 mm3. Post-contrast T1W-VISTA was performed about 6 min after an intravenous injection of GdDTPA (Magnevist; Bayer Schering Pharma, Berlin, Germany) at a dose of 0.1 mmol/kg. The imaging parameters for TOF-MRA were TR/TE = 25/3.5 ms, FOV = 160×160×60 mm3, voxel size = 0.8×0.8×0.8 mm3.
Data Analysis:
AWE was divided into four grades according to the extent and range of the enhancement, as shown in Figure 1. Among them grade 0 was with no enhancement; grade 1 was with focal enhancement; grade 2 was with circumferential aneurysmal wall enhancement (CAWE) and maximum thickness ≤1 mm; grade 3 was with CAWE and maximum thickness >1 mm. According to the pre- and post-contrast HR-VWI images, two experienced readers (neuroradiologists with 7 and 5 years of experience, respectively) who were blinded to the imaging data determined the AWE grades. An agreement was reached through joint discussion of the cases if disagreement arisen.
Inflow angle was the angle between the direction of the parent artery flow and the aneurysm dome axis. Here the direction of the parent artery flow was defined as the axis tangent to the parent artery centerline at the point closest to the center point of the aneurysm neck and aneurysm dome axis was the longest line from the center point of the aneurysm neck to the aneurysm top. The inflow angle was measured in three-dimensional space in this study by 3D TOF-MRA images in our inhouse software, as shown in Figure 2.
Statistical analysis:
To identify the characteristics of patients and aneurysms corresponding to different grades of AWE, the statistical comparison was performed using Mann-Whitney U test for continuous variables and χ2 test for categorical variables. Furthermore, the Pearson correlation coefficient was used to investigate the relationship between AWE and inflow angle. The level of statistical significance was set at P< 0.05.
Results
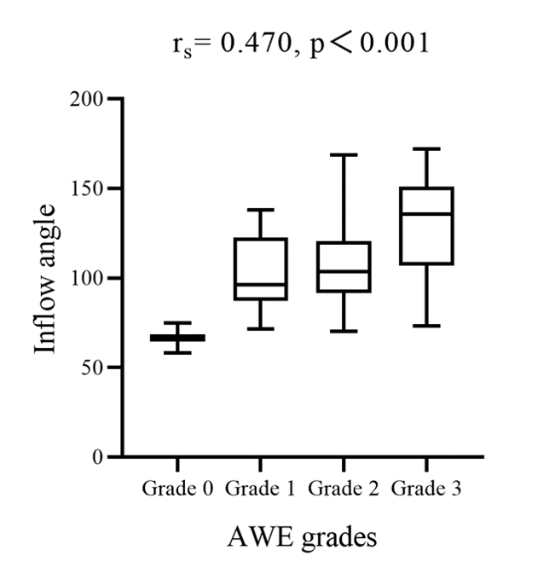
There was a significant difference between inflow angles corresponding to different grades of AWE (p = 0.006), as listed in Table 1. Further Pearson correlation analysis showed that AWE was positively associated with inflow angle (r = 0.470, p < 0.001), as shown in Figure 3. The illustrated cases also showed the same tendency, as shown in Figure 4.Discussion and Conclusion
In this study, we investigated the relationship between AWE grades and aneurysm inflow angle by combination of HR-VWI and 3D TOF-MRA images. Statistics indicated that significant difference existed among inflow angles corresponding to different grades of AWE. The result of Pearson correlation analysis clarified the difference and further showed the positive relationship between AWE grades and inflow angles. This is probably because a sidewall aneurysm with high inflow angle is easier to grow, which leads to farther distance for blood flow traveling in aneurysm, thus slower inflow velocity and lower wall shear stress. Slower inflow velocity and lower wall shear stress may upgrade endothelial surface adhesion molecules and increase the permeability of aneurysm wall[6], thus promoting aneurysmal wall inflammation processes and causing a high grade of AWE.Acknowledgements
No acknowledgement found.References
1. Vlak MH, Algra A, Brandenburg R, et al. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: a systematic review and meta-analysis. Lancet Neurol. 2011, 10(7):626-36.
2. Li MH, Chen SW, Li YD, et al. Prevalence of unruptured cerebral aneurysms in Chinese adults aged 35 to 75 years: a cross-sectional study. Ann Intern Med. 2013, 159(8):514-21.
3. Tulamo R, Frösen J, Hernesniemi J, et al. Inflammatory changes in the aneurysm wall: a review. J Neurointerv Surg. 2018, 10(Suppl 1):i58-i67.
4. Turjman Alexis S,Turjman Francis,Edelman et al, Role of fluid dynamics and inflammation in intracranial aneurysm formation. Circulation, 2014, 129: 373-82.
5. Nagahata S, Nagahata M, Obara M, et al. Wall enhancement of the intracranial aneurysms revealed by magnetic resonance vessel wall imaging using three-dimensional turbo spin-echo sequence with motion-sensitized driven-equilibrium: a sign of ruptured aneurysm? Clin Neuroradiol. 2016, 26:277–83.
6. Takehara Y, Isoda H, Takahashi M, et al. Abnormal Flow Dynamics Result in Low Wall Shear Stress and High Oscillatory Shear Index in Abdominal Aortic Dilatation: Initial in vivo Assessment with 4D-flow MRI. Magn Reson Med Sci. 2020, 19(3):235-246.
Figures

Figure.1 Grading pattern of aneurysmal wall enhancement. Each column corresponds to one grade. A, grade 0: aneurysm with no enhancement; B, grade 1: aneurysm with focal enhancement; C, grade 2: aneurysm with circumferential aneurysmal wall enhancement (CAWE) and maximum thickness ≤ 1 mm; D, grade 3: aneurysm with CAWE and maximum thickness > 1 mm. Time-of-flight MR images, pre-contrast T1-weighted volumetric isotropic turbo spin echo acquisition (T1-VISTA) images, post-contrast T1-VISTA images were shown from top to bottom row, respectively.
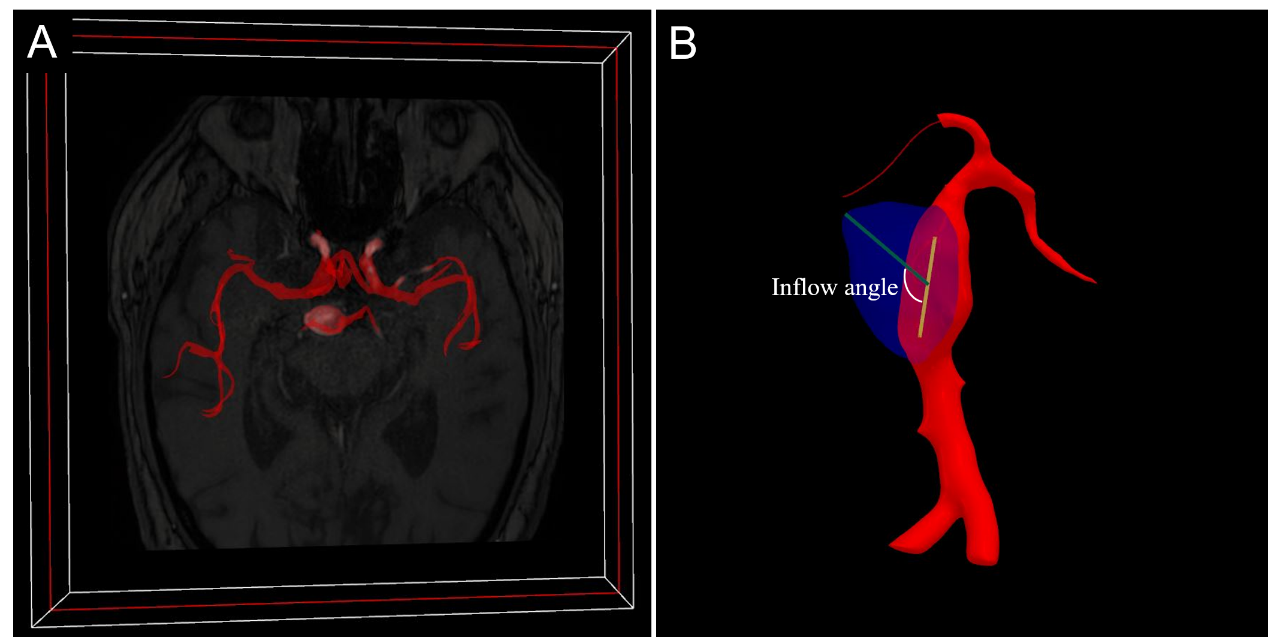
Figure.2 Measurement of aneurysm inflow angle. A, the generated 3D vessel model from Time-of-flight MR images. B, measured inflow angle by axis tangent to the parent artery centerline, indicated by yellow line, and aneurysm dome axis, indicated by green line.

Figure.3 Cases of sidewall aneurysms with different inflow angles and AWE grades. Each column corresponds to one aneurysm.