4548
Evaluation of the Instability of Intracranial Aneurysms Wall by Dynamic Contrast-enhanced Magnetic Resonance Imaging and Vessel Wall Imaging1Department of Magnetic Resonance, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 2Department of Interventional Neuroradiology, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 3Department of Radiology, University of Washington, Washington, WA, United States
Synopsis
This study used DCE-MRI and VWI to explore the value of Ktrans and aneurysm wall enhancement (AWE) in screening UIAs instability. Eighty-two patients were enrolled, including 51 patients with stable IAs and 31 patients with unstable IAs. All patients completed examinations based on a 3.0T Siemens Prisma magnetic resonance. Multivariate logistic regression revealed that AWEP (OR, 4.1; 95% CI, 2.06 to 8.16; P < 0.001) and Ktrans (OR, 2.77; 95% CI, 1.49 to 5.17; P = 0.01) were the only independent factors associated with unstable UIAs. Both Ktrans and AWEP were independent risk factors for the unstable state of UIAs.
Objective
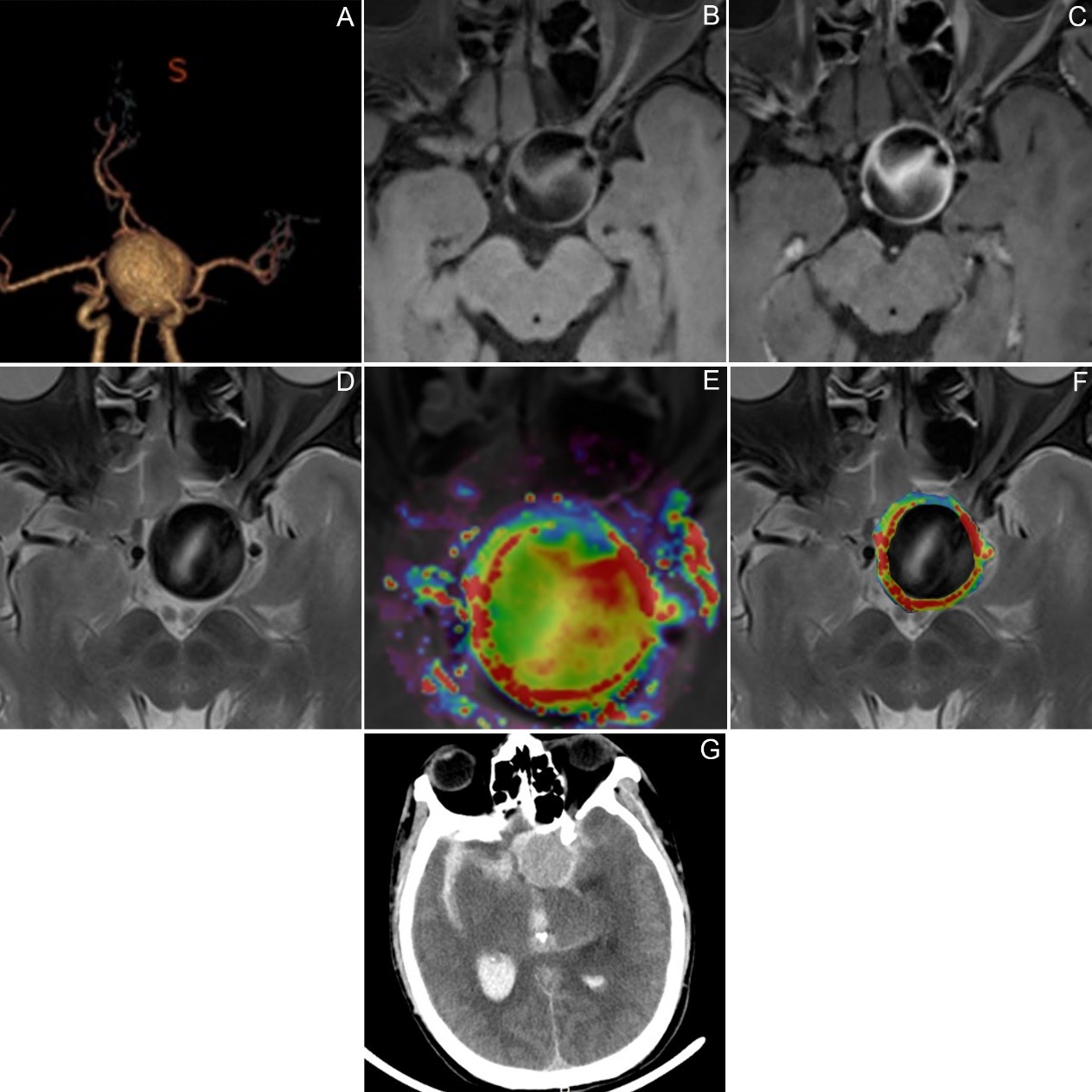
Intracranial aneurysms (IAs) were pathological enlargements of intracranial arteries, with an incidence of 3% to 5% in adult populations regardless of race or region. Relative to the risk of Unruptured intracranial aneurysm (UIAs) spontaneously rupturing, the dangers posed by UIAs treatment might be higher. Therefore, to balance the risks and benefits of the treatment of UIAs patients, it was of great significance to study individualized IAs rupture risk assessment markers. In daily clinical practice, the risk assessment of IAs mainly based on morphological factors such as diameter. Pathological features based on the wall of IAs might help supplement pure morphological markers. At present, most of the noninvasive imaging studies on the walls of IAs based on VW-MRI. In clinical practice, sentinel headaches with a high risk of rupture of IAs also caused by micro-exudation of blood. A large amount of blood surging into the cerebrospinal fluid of the subarachnoid space caused by the total rupture of the IAs wall led to the SAH. The blood mentioned above leakage may be detected by gadolinium contrast agent by DCE-MRI and based on the post-processing algorithm to obtain Ktrans for quantitative evaluation. This study used DCE-MRI and VW-MRI to explore the value of Ktrans and aneurysm wall enhancement (AWE) in screening UIAs instability.Methods
1. Our hospital prospectively collected IAs patients who underwent 3.0 T magnetic resonance gadolinium-enhanced DCE-MRI, VW-MRI, and DSA from January 2018 to October 2019. Symptomatic UIAs and ruptured IAs were identified through MDT and defined as unstable IAs. The Incidentally discovered IAs limited as a stable state. Eighty-two patients were enrolled, including 51 patients with stable IAs and 31 patients with unstable IAs. All patients completed gadolinium-enhanced DCE-MRI and 3D-VW-MRI examinations based on a 3.0T Siemens Prisma magnetic resonance scanner (64-channel head and neck combined coil).2. Two experienced neuroimaging physicians independently performed the blind analysis of the DCE-MRI images of IAs through the Siemens syngo.via workstation TISSUE 4D software and calculate the complete quantitative pharmacokinetic index of the corresponding aneurysms-Ktrans.
3. Two senior neuroimaging physicians independently performed a blind reading on the PACS platform to determine whether AWE appeared and further classify enhancement pattern of the aneurysm wall (AWEP): AWEP 0 (none), AWEP 1 (focal), and AWEP 2 (circumferential).
4. We used MedCalc 18.2 software for statistical processing. Percentages represented categorical variables, and continuous variables were described by x ̅ ± s or median (interquartile range). Kappa test evaluated the consistency of AWE and its classification by two physicians. We used the Bland-Altman diagram, Passing and Bablok regression, and ICC to consider the character of Ktrans by two physicians. The χ2 test compares categorical variables between groups, and the U test compares continuous variables between groups. The univariate regression analysis included variables with P <0.2 between the groups. The multivariate logistic regression analysis included Variables (univariate regression analysis results P <0.05) to obtain 95% CI and OR for predicting the unstable state of UIAs. We have analyzed categorical or continuous variables through the ROC curve to bring sensitivity, specificity, etc. The Youden index clarified the cutoff value of the ROC curve. The χ2 test analyzed the categorical variables, and the Jonckheere-Terpstra test analyzed the continuous variables. P <0.05 was considered statistically significant.
Result
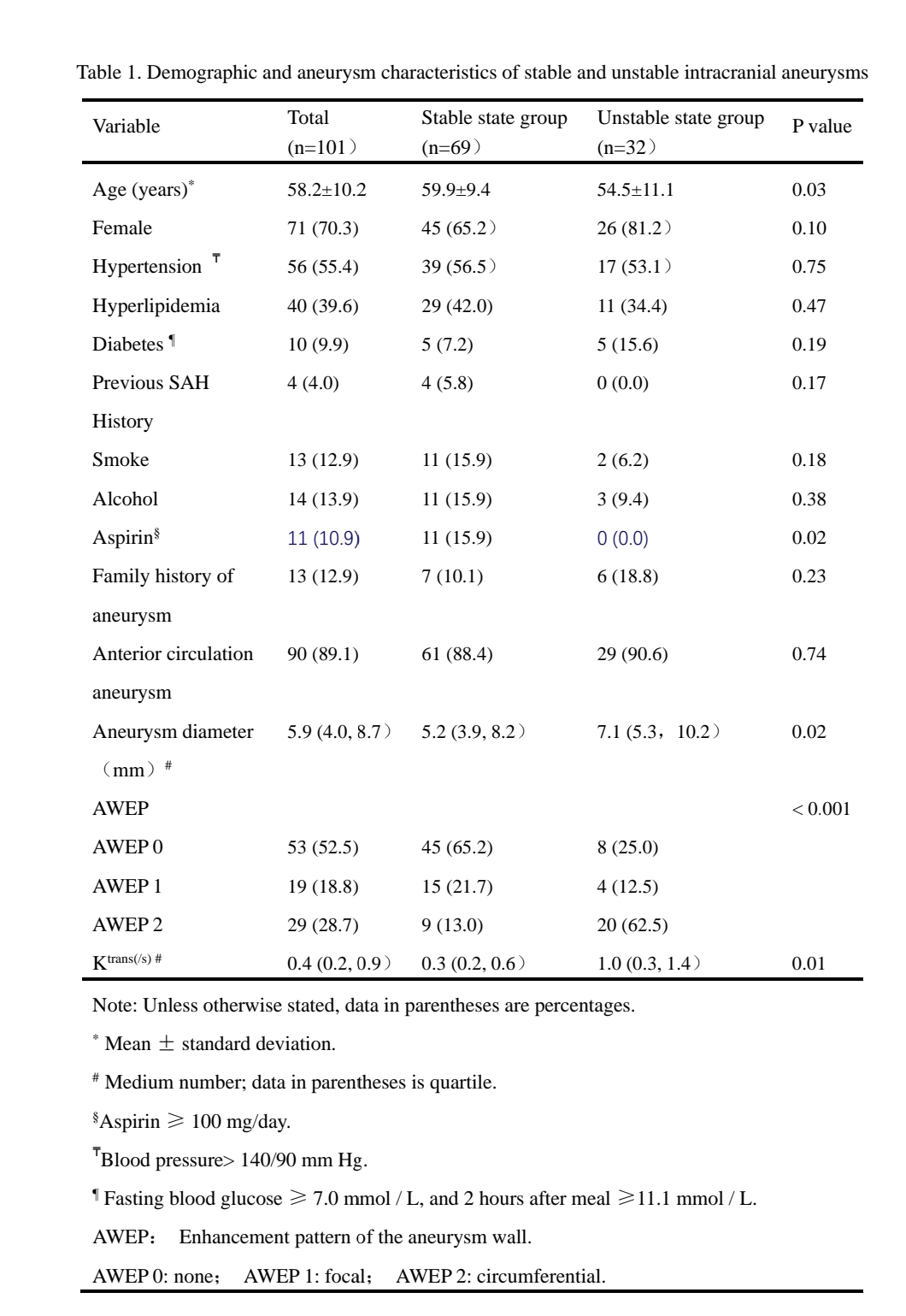
1. This study included 82 patients with 101 UIAs. Inter-reader agreement was excellent for both the presence of AWE (k = 0.85 [95% CI: 0.75 to 0.96]), AWE's classification (k = 0.81 [95% CI: 0.71 to 0.92]) and the calculation of Ktrans (ICC = 0.98 [95% CI: 0.97 to 0.99]).2. The median of Ktrans was significantly higher in unstable than in stable UIAs (0.9 versus 0.3 s-1, respectively; P < 0.001). There was also a difference in the composition ratio of AWEP in the unstable state of UIAs (P <0.001).
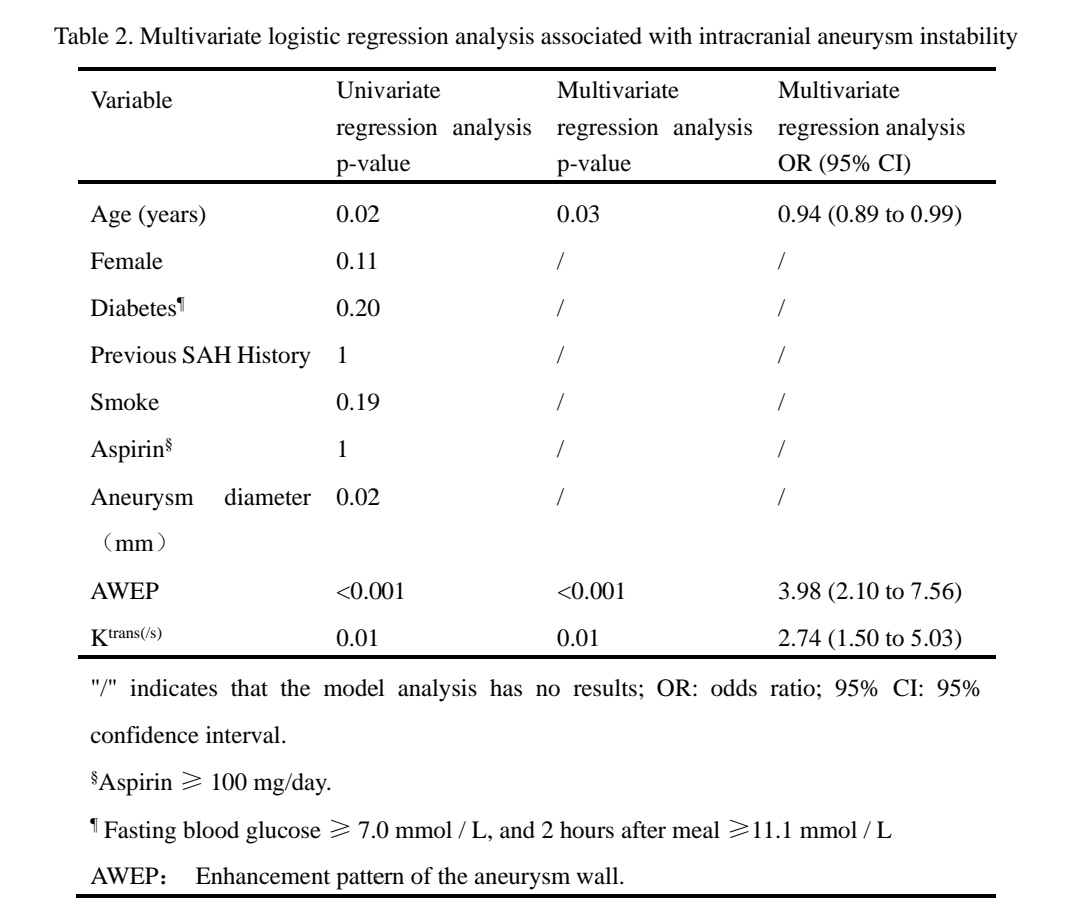
3. Multivariate logistic regression revealed that AWEP (OR, 4.1; 95% CI, 2.06 to 8.16; P < 0.001) and Ktrans (OR, 2.77; 95% CI, 1.49 to 5.17; P = 0.01) were the only independent factors associated with unstable UIAs.
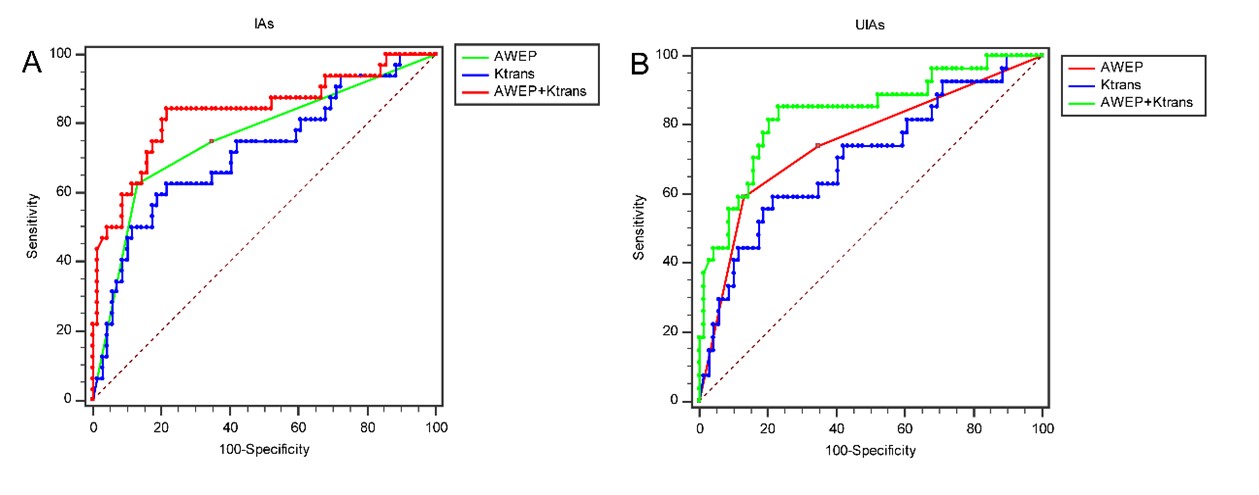
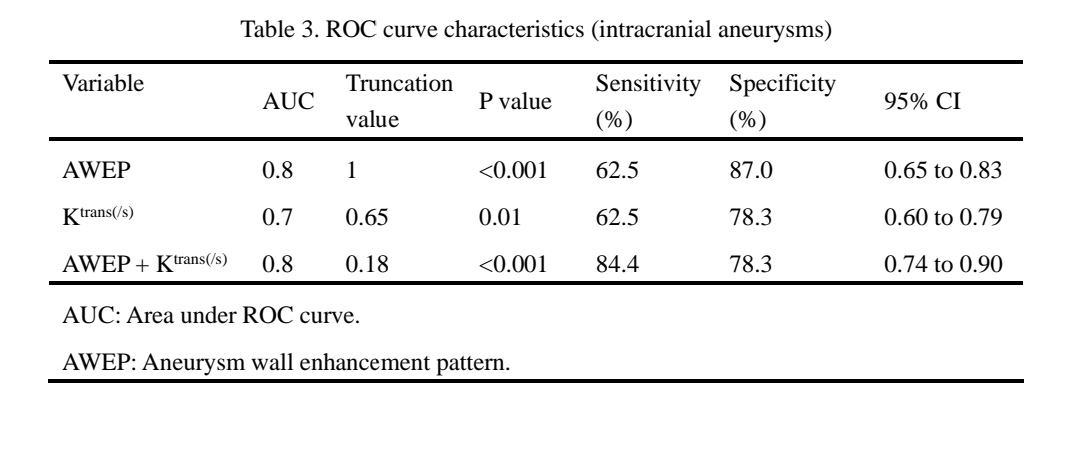
4. The cutoff value of AWEP screening UIAs unstable state was AWEP > 1 (sensitivity: 59.3%, specificity: 87.0%), AUC was 0.75 (95% CI: 0.65 to 0.83), Youden index was 0.50, P < 0.001. The cut-off value of Ktrans screening UIAs unstable state was Ktrans > 0.65 s-1 (sensitivity: 59.3%, specificity: 78.3%), AUC was 0.70 (95% CI: 0.60 to 0.79), and Youden index was 0.38, P = 0.01. The cut-off value of combined with Ktrans and AWEP screening UIAs unstable state was Ktrans + AWEP > 0.18 (sensitivity: 85.2%, specificity: 76.8%), AUC was 0.83 (95% CI: 0.74 to 0.90), and Yoden index was 0.62 , P <0.001.
Conclusion
1. This is the first large-sample study combining DCE-MRI and VWI to explore the instability of UIAs.2. Both Ktrans and AWEP were independent risk factors for the unstable state of UIAs.
3. Ktrans> 0.65 s-1 could effectively screen the unstable state of UIAs. AWEP could also effectively screen the unstable state of UIAs. The Ktrans + AWEP had the highest sensitivity to screen the unstable state of UIAs.
Keywords
magnetic resonance imaging; intracranial aneurysms; aneurysmal wall enhancement; the contrast agent permeability rateAcknowledgements
No acknowledgement found.References
[1] Quan K, Song J, Yang Z, et al. Validation of Wall Enhancement as a New Imaging Biomarker of Unruptured Cerebral Aneurysm[J]. Stroke, 2019.DOI:10.1161/ STROKEA HA.118.024195.
[2] Fu Q, Guan S, Liu C, et al. Clinical Significance of Circumferential Aneurysmal Wall Enhancement in Symptomatic Patients with Unruptured Intracranial Aneurysms: a High-resolution MRI Study[J]. Clinical Neuroradiology, 2018,28(4):509-514.DOI:10.1007/s00062-017-0598-4.
[3] Zhang Y, Fu Q, Wang Y, et al. Qualitative and Quantitative Wall Enhancement Analyses in Unruptured Aneurysms Are Associated With an Increased Risk of Aneurysm Instability[J]. Frontiers in Neuroscience, 2020,14.DOI:10.3389/fnins.2020.580205.
[4] Fu Q, Wang Y, Zhang Y, et al. Qualitative and Quantitative Wall Enhancement on Magnetic Resonance Imaging Is Associated With Symptoms of Unruptured Intracranial Aneurysms[J]. Stroke (1970), 2021,52(1):213-222.DOI:10.1161/STROKEAHA.120.029685.
[5] Edjlali M, Guédon A, Ben Hassen W, et al. Circumferential Thick Enhancement at Vessel Wall MRI Has High Specificity for Intracranial Aneurysm Instability[J]. Radiology, 2018,289(1):181-187.DOI:10.1148/radiol.2018172879.
[6] Vakil P, Ansari S A, Cantrell C G, et al. Quantifying Intracranial Aneurysm Wall Permeability for Risk Assessment Using Dynamic Contrast-Enhanced MRI: A Pilot Study[J]. American Journal of Neuroradiology, 2015,36(5):953-959.DOI:10.3174/ajnr. A4225.
[7] Qi H, Liu X, Liu P, et al. Complementary Roles of Dynamic Contrast-Enhanced MR Imaging and Postcontrast Vessel Wall Imaging in Detecting High-Risk Intracranial Aneurysms[J]. American Journal of Neuroradiology, 2019.DOI:10.3174/ajnr.A5983.
Figures