4544
Aortic kinetic energy in repaired tetralogy of Fallot patients with or without aortic root dilatation1Department of Biomedical Engineering and Environmental Sciences, National Tsing Hua University, Hsinchu, Taiwan, 2Department of Radiology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 3Department of Pediatrics, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan
Synopsis
The aortic hemodynamic flow pattern and aortic kinetic energy (KE) is less discussed for repaired tetralogy of Fallot (rTOF) patients without aortic root dilatation. We aimed to evaluate aortic KE in rTOF patients with or without aortic root dilatation. The rTOF1 patients (indexed aortic root diameter<16 mm/m2) demonstrated aortic regurgitation. Both rTOF1 and rTOF2 (indexed aortic root diameter≥16 mm/m2) patients exhibited normal aortic vorticity and decreased aortic KE. In conclusion, in rTOF patients with preserved left ventricular ejection fraction, the altered velocity-derived KE and RF can provide an indication of aortapathy progress earlier than morphological aortic dilatation and aortic vorticity.
Introduction
Aortapathy in patients with repaired tetralogy of Fallot (rTOF) is associated with aortic stiffness, dilatation and left ventricular (LV) dysfunction [1,2]. Abnormal flow patterns, such as vortical and helical flow, are seen in rTOF patients with normal diameters in aortic ascending segment [3,4] and may affect the progress of aortapathy [4].Ventricular kinetic energy (KE) provides a new insight to assess cardiac performance and decreased ventricle-vascular efficiency for systemic circulation will contribute to excess work and earlier failure [5]. Aortic root wall degradation is found in infants with rTOF [6]. However, a systematic investigation focused on the aortic hemodynamic flow pattern and aortic KE is less discussed for rTOF patients without aortic root dilatation. In this study, we calculated aortic KE in rTOF patients with normal or dilated aortic roots. The purpose was to evaluate changes of aortic flow and energetic parameters before aortic root dilatation.
Methods
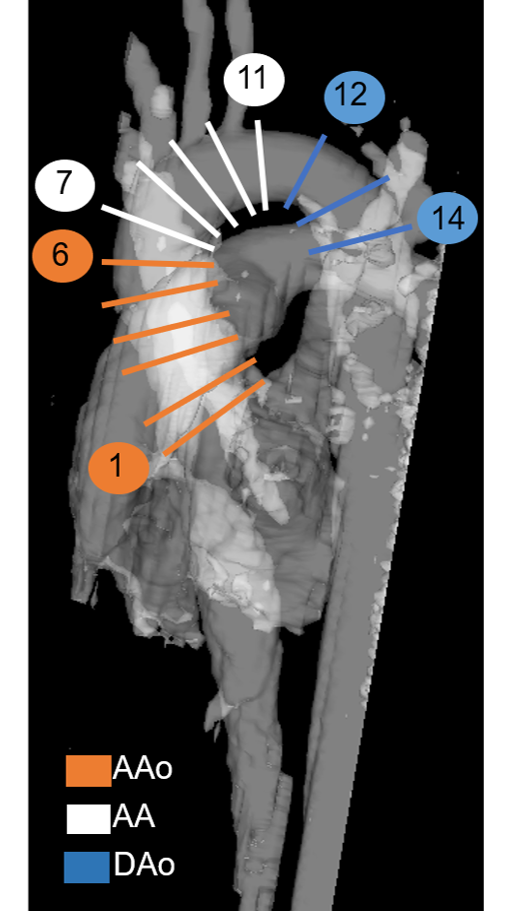
The study population comprised 35 patients with rTOF (age 22±3 years, 15 females) and 28 age-matched normal volunteers (age 22±1 years, 13 females). The indexed aortic diameter is the mean aortic diameter averaged across the cardiac cycle normalized by body surface area. A threshold of indexed aortic diameter, which determined by the mean+2xstandard deviation of at the first plane of the aorta in normal group, was used to divide rTOF patients into two subgroups: rTOF1 group (n=22) and rTOF2 group (n=13) were with indexed aortic diameter < 16 mm/m2 and ≥ 16 mm/m2, respectively. The 4D flow data was acquired in a 3-Tesla MR scanner (Tim Trio or Skyra, Siemens) with prospective ECG-triggering (acquire 90% of RR interval) and navigator-gating to synchronize with heartbeat and respiratory motion, respectively. The scanning parameters were: TR/TE=10.8/2.9 ms, voxel size=3.2x1.4x3.5 mm3, flip angle=7°, Venc=150 cm/s, and temporal resolution=41.6 ms. Fourteen planes were localized perpendicularly to the long-axis of aorta in the 4D flow data-derived MR angiography (Figure 1). The regions-of-interest (ROI) of the aortic lumen were manually determined in magnitude images and transferred to phase images for computation of aortic flow. The aortic RF was calculated by:$$RF=\frac{retrodegrade flow}{antegrade flow}\times100\%$$ The aortic KE was calculated by:$$KE=\frac{1}{2}\rho Vv^{2}$$ where V is the volume of voxel, $$$v$$$ is velocity and $$$\rho$$$ is the blood density with a value of 1060 kg/m3. The peak and mean KE is the maximum and mean aortic KE averaged across the cardiac cycle. The aortic vorticity ($$$\mid\overrightarrow{\omega}\mid$$$) was calculated by: $$\mid\overrightarrow{\omega}\mid=\mid\nabla\overrightarrow{v}\mid$$ where $$$v$$$ is velocity. Student t test was performed when appropriate. A p<0.05 was considered statistically significant. The Receiver operating characteristic (ROC) curve was used to determine the cut-off value.Results
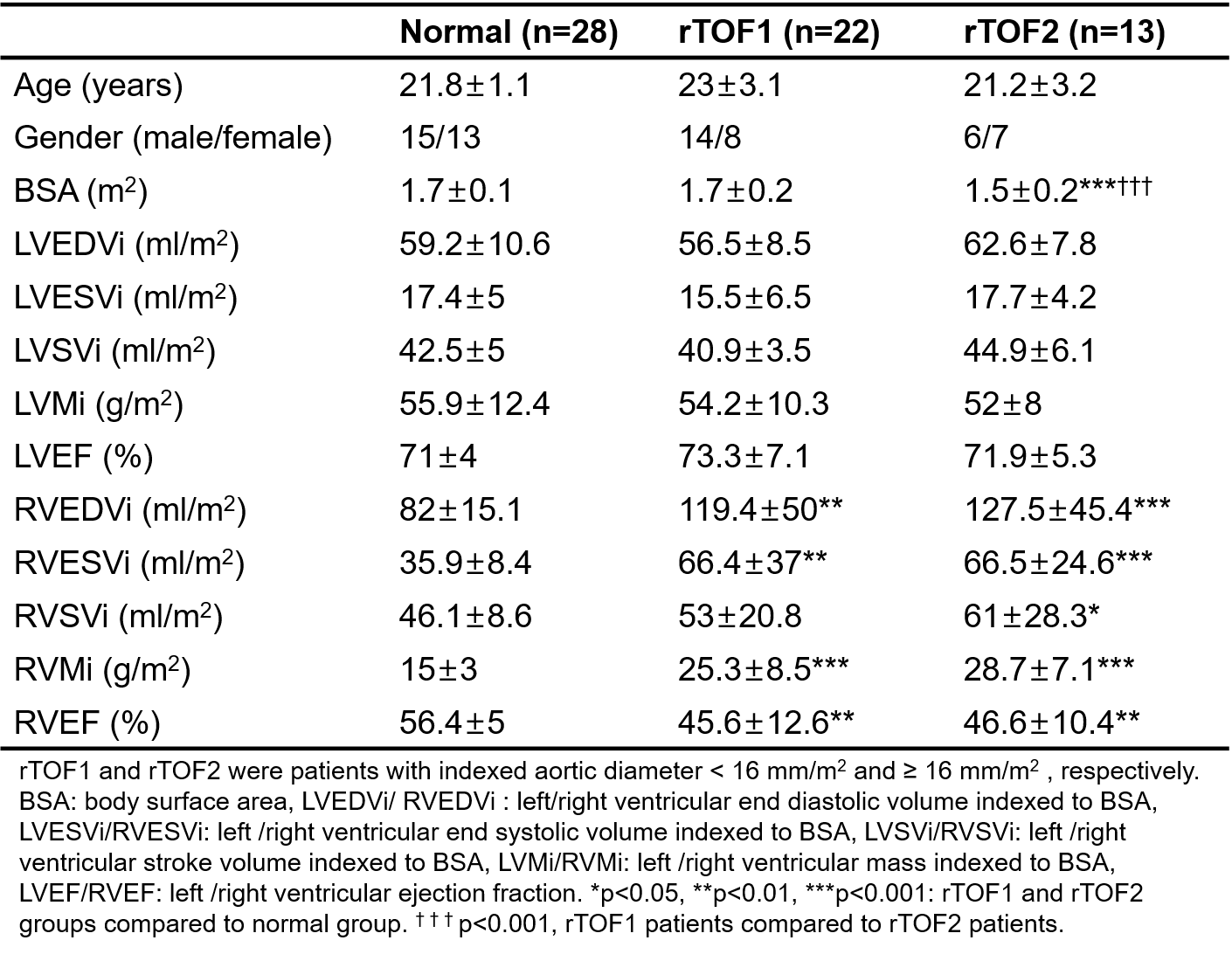
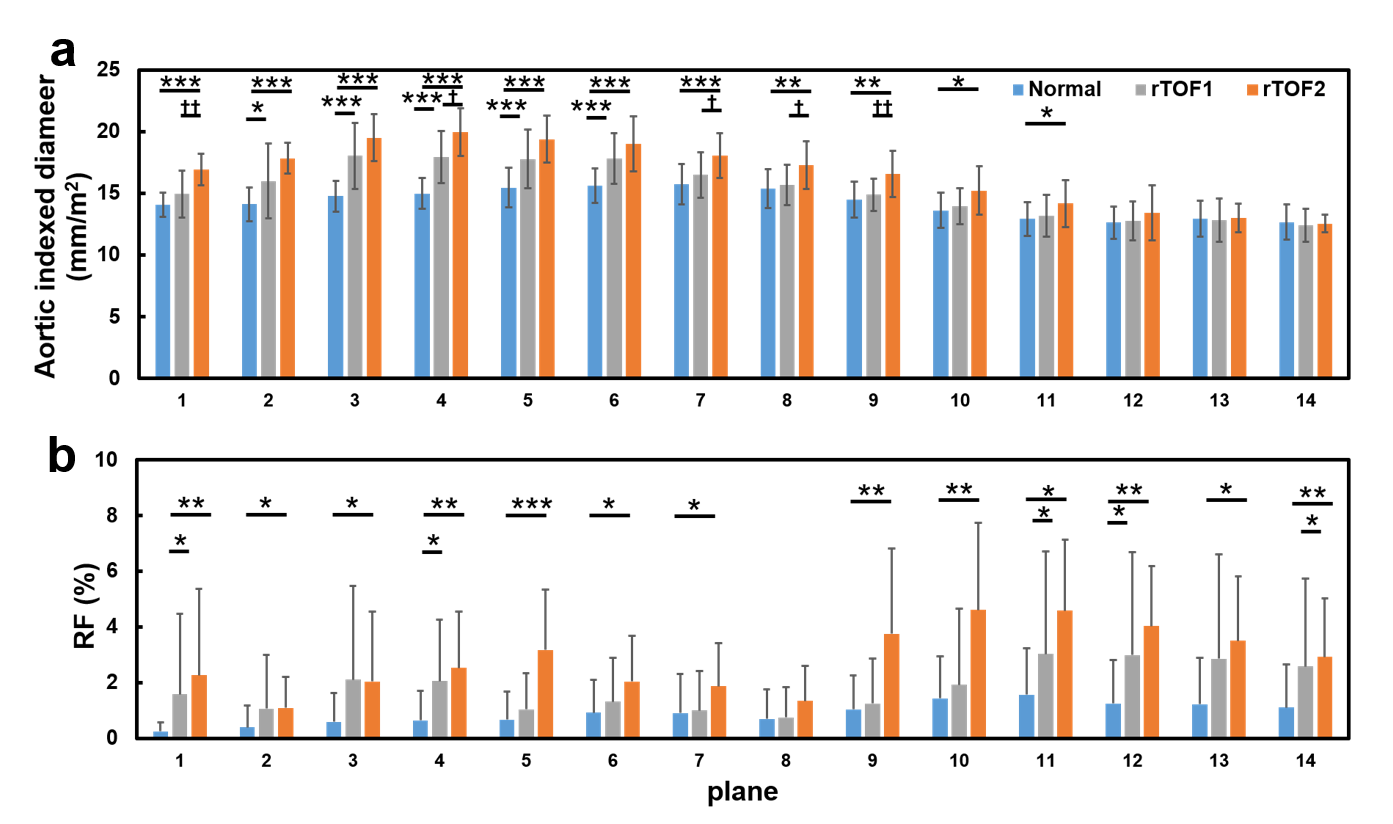
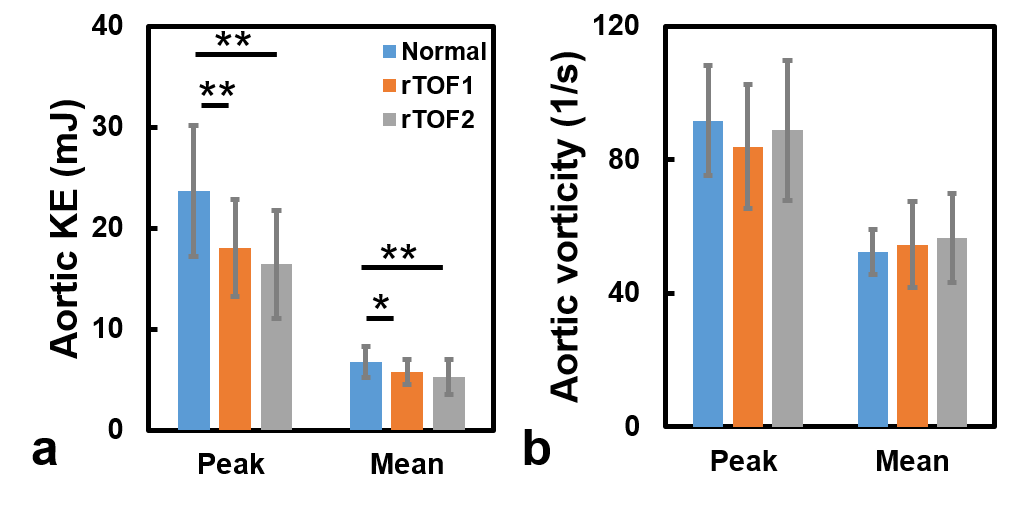
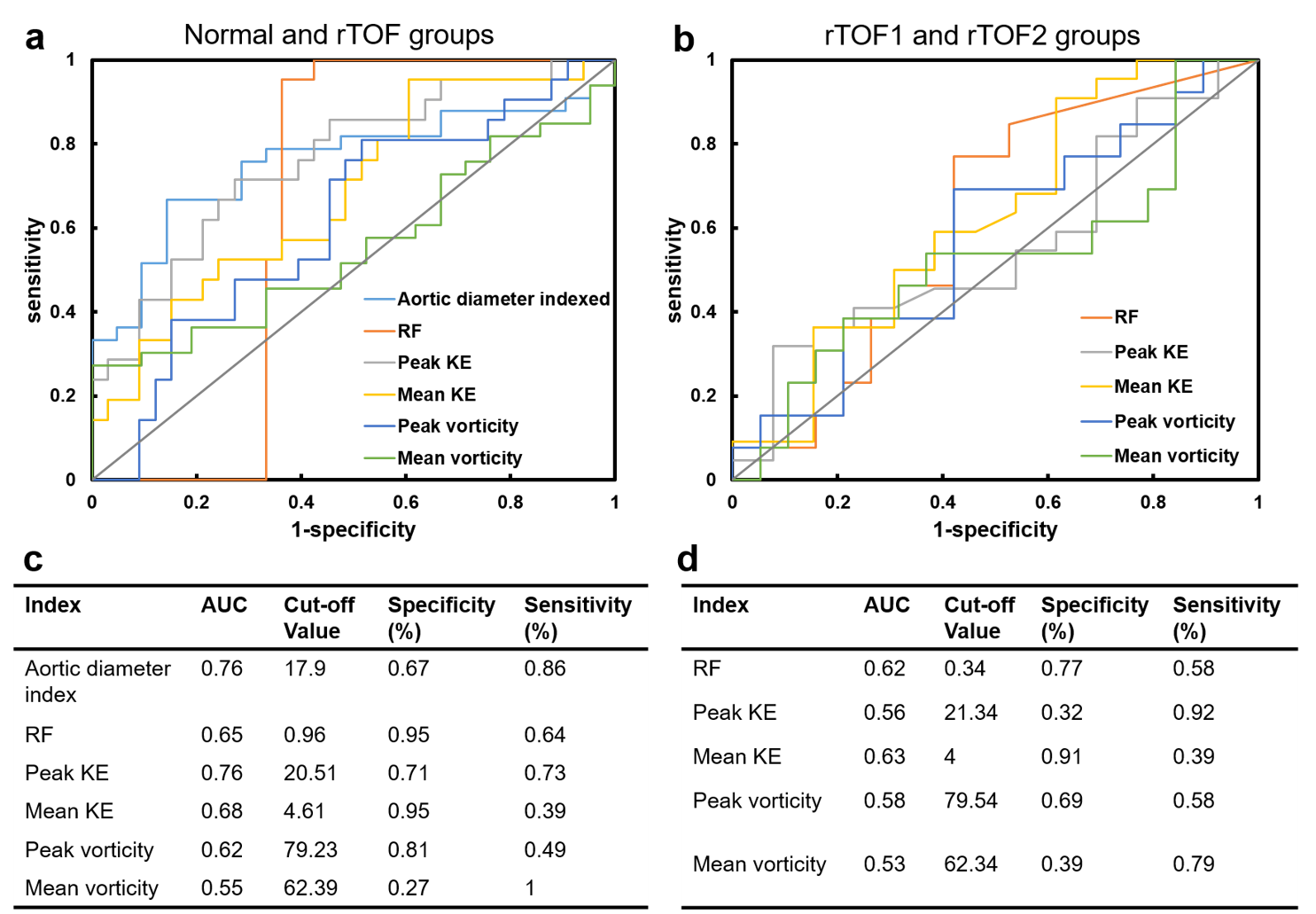
Table 1 illustrates the demographics and cardiac function in normal and two rTOF groups. Both rTOF1 and rTOF2 groups exhibited increased indexed right ventricular end diastolic and systolic volumes, stroke volume, and mass (all p<0.05) and reduced right ventricular ejection fraction (p<0.01). The left ventricular volumetric and ejection fraction were preserved. In Figure 2, rTOF1 group presented normal indexed diameter at aortic root while rTOF2 group showed increased aortic root size (p<0.001) in comparison to normal group. Both rTOF1 and rTOF2 groups exhibited elevated RF (both p<0.05) in aortic root. In comparison to normal group, both rTOF1 and rTOF2 groups presented decreased aortic peak and mean KE (all p<0.05) and comparable aortic vorticity (Figure 3). In Figure 4(a,c), indexed aortic diameter and peak KE presented an area-under-curve (AUC) to differentiate rTOF patients from normal volunteers (both AUC=0.76). In Figure 4(b,d), mean KE could differentiate rTOF2 from rTOF1 with an AUC=0.63, although mean KE was with low sensitivity of 0.39.Discussion and conclusion
In this study, the rTOF2 group has mild aortic root dilatation, elevated RF at aortic root, decreased aortic KE, and preserved aortic vorticity. The rTOF1 group, which has normal indexed aortic root diameter, also presented similar hemodynamic and energetic conditions as in rTOF2 group. Therefore, we found that abnormal velocity-derived KE and RF may proceed the morphological aortic dilatation and aortic vorticity in aortapathy progress.Intraventricular KE can reflect disordered flow and may provide earlier evidence of ventricular dysfunction [5]. Abnormal secondary flow is associated with induced viscous energy loss and reduced left ventricular function [7]. In our study, instead of measuring intraventricular KE, we evaluated the aortic KE in aortic root. The rTOF1 group presented comparable aortic root size and aortic vorticity in comparison with normal group while showed decreased peak and mean aortic KE, suggesting that aortic KE was able to detect disturbed aortic flow earlier than aortic dilatation and secondary flow pattern. Furthermore, the high sensitivity of peak KE and high specificity of mean KE underscored the importance of combining these two indices for detection of aortopathy.
In our study, rTOF1 patients present aortic root regurgitation despite normal aortic root size. The histology changes in aortic root wall is found in infants with rTOF [6]. Therefore, we speculated that the aortic root regurgitation could be attributed to inherent aortic wall changes and it could occur even without aortic root dilatation.
In conclusion, in rTOF patients with preserved left ventricular ejection fraction, the altered velocity-derived KE and RF can provide an indication of aortapathy progress earlier than morphological aortic dilatation and aortic vorticity.
Acknowledgements
No acknowledgement found.References
[1] Tan et al. "Intrinsic histological abnormalities of aortic root and ascending aorta in tetralogy of Fallot: evidence of causative mechanism for aortic dilatation and aortopathy." Circulation 112.7 (2005): 961-968.
[2] Shiina et al. "Aortopathy in adults with tetralogy of Fallot has a negative impact on the left ventricle." International journal of cardiology 228 (2017): 380-384.
[3] Schäfer et al. "Reduced proximal aortic compliance and elevated wall shear stress after early repair of tetralogy of Fallot." The Journal of thoracic and cardiovascular surgery 156.6 (2018): 2239-2249.
[4] Shiina et al. "Aortic vorticity, helicity, and aortopathy in adult patients with tetralogy of fallot: Pilot study using four-dimensional flow magnetic resonance images." Pediatric Cardiology 42.1 (2021): 169-177.
[5] Jeong et al. "Ventricular kinetic energy may provide a novel noninvasive way to assess ventricular performance in patients with repaired tetralogy of Fallot." The Journal of thoracic and cardiovascular surgery 149.5 (2015): 1339-1347.
[6] François et al. "Analysis of the aortic root in patients with tetralogy of Fallot undergoing early repair: form follows function." The Journal of thoracic and cardiovascular surgery 148.4 (2014): 1555-1559.
[7] Schäfer et al. "Abnormal aortic flow conduction is associated with increased viscous energy loss in patients with repaired tetralogy of Fallot." European Journal of Cardio-Thoracic Surgery 57.3 (2020): 588-595.
Figures