4535
The effect of compressed sensing with multiple acceleration factors on brachial plexus 3D NerveVIEW1Department of Radiology, the First Affiliated Hospital of Dalian Medical University, Dalian, Dalian, China
Synopsis
The 3D-NerveVIEW sequence with suppression of lipid and blood signals and a long echo time can obtain high-quality images for visualization of brachial plexus, while the long scan time may limit its clinical application. Compressed SENSE (CS) is a newly developed technique in MRI that enables accelerated acquisition with maintained image quality. By comparing results of 3D-NerveVIEW for brachial plexus imaging with acceleration by the conventional SENSE and the advanced CS with dierent acceleration factors. We found that the 3D-NerveVIEW for brachial plexus imaging with a CS acceleration factor of 6 can obtained favorable images within signicantly reduced scan time.
Synopsis
The 3D-NerveVIEW sequence with suppression of lipid and blood signals and a long echo time can obtain high-quality images for visualization of brachial plexus, while the long scan time may limit its clinical application. Compressed SENSE (CS) is a newly developed technique in MRI that enables accelerated acquisition with maintained image quality. By comparing results of 3D-NerveVIEW for brachial plexus imaging with acceleration by the conventional SENSE and the advanced CS with dierent acceleration factors. We found that the 3D-NerveVIEW for brachial plexus imaging with a CS acceleration factor of 6 can obtained favorable images within signicantly reduced scan time.Introduction
Magnetic resonance imaging (MRI) is the favored modality for evaluating the brachial plexus because of its multiplanar capabilities and excellent soft-tissue contrast. The 3D-NerveVIEW sequence with suppression of lipid and blood signals and a long echo time can obtain high-quality images for brachial plexus, but the long scan time of 3D acquisition can be a problem for clinical applications. Compressed SENSE (CS) is a newly developed technique in MRI that enables acceleration of MR scan without sacrice of image quality1,2. This study aims to evaluate the application CS on 3D-NerveVIEW imaging for brachial plexus, and to find an optimized acceleration factor.Materials and Methods
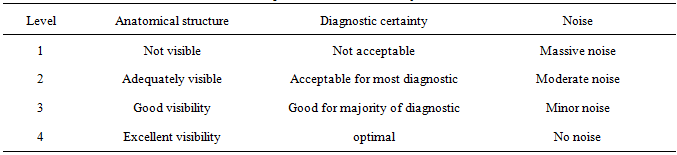
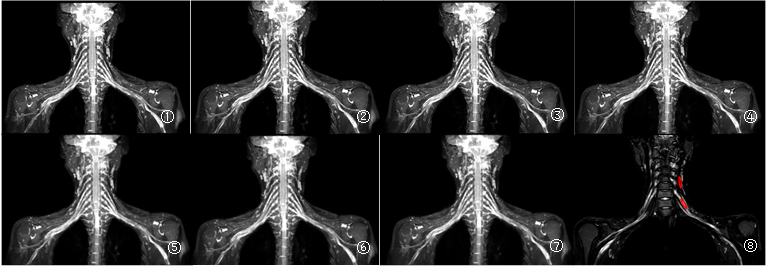
This study has been approved by the local IRB. 24 healthy volunteers (10 males, age 45.92±16.73) were recruited and underwent the 3D-NerveVIEW scan of brachial plexus on a 3.0 T MR scanner (Ingenia CX, Philips Healthcare, Best, the Netherlands). Scan parameters are as follows: TR: 2200ms, TE: 170ms, FOV: 300X453X96 mm, NSA: 2, voxel size: 1.2X1.2X2.4 mm, matrix: 252X378mm, slice thickness and Gap: 2.4/-1.2 mm, The 3D-NerveVIEW was scanned with dierent acceleration factors including the conventional SENSE factor of 2 (SENSE2, as reference) and CS factors of 2 to 12 with a interval of 2 (CS2-CS12). 7 sets of data were collected for each volunteer obtained with scan time recorded. The signal intensity (SI) and standard deviation (SD) for brachial plexus and muscle were measured for each group on the coronal images. ROIs area were approximately 15 mm2 (Fig.1). SNR and CNR were measured as SNR=SIbrachial plexus/SDmuscle and CNR=(SIbrachial plexus-SImuscle)/SDmuscle. The image quality of each dataset was scored subjectively by two radiologists on a four-point scoring criterion(table.1). The intraclass correlation coefficient and Kappa test was adopted to evaluate the consistency of the scores from the two radiologists. If the consistency was in good agreement, the corresponding images would be adopted for the analysis in further by senior physicians. In the following analysis, the Friedman test was used to assess the difference of SNR, CNR and score between groups, and the LSD test was employed to make a pairwise comparison.Result
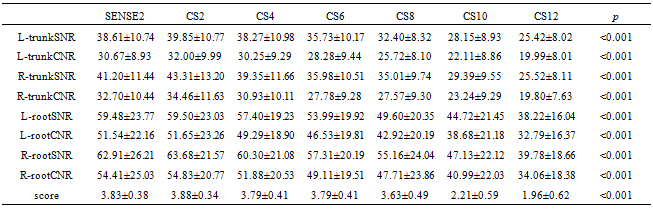
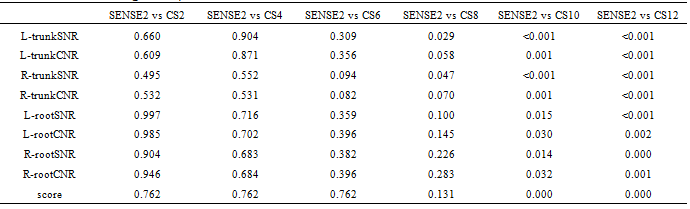
The measurement data and the score of the two observers were in good agreement(ICC:0787-0.995,Kappa:0.778-0.882), it was shown that there were statistically significant differences in SNR, CNR and score of different AF(table.2). When CS=8, the SNR of left and right nerve trunk are significantly different from those of conventional sequences (p<0.05); When CS=10, the SNR of left and right nerve trunk, SNR, CNR and supervisor scores of left and right nerve root have statistically significant differences compared with conventional sequences(table.3) (p<0.05).Discussion and Conclusion
Scan time for the brachial plexus decreased gradually with increase of the CS acceleration factor. CS factor of 6 was recommended for clinical to achieve an optimal balance between scan time and image quality, with scan time decrease to 64.31%.Acknowledgements
No acknowledgement found.References
[1] Craven T P, Jex N, Chew P G, et al. Exercise cardiovascular magnetic resonance: feasibility and development of biventricular function and great vessel flow assessment, during continuous exercise accelerated by Compressed SENSE: preliminary results in healthy volunteers[J]. Int J Cardiovasc Imaging,2021,37(2):685-698.
[2]He M, Xu J, Sun Z, et al. Comparison and evaluation of the efficacy of compressed SENSE (CS) and gradient- and spin-echo (GRASE) in breath-hold (BH) magnetic resonance cholangiopancreatography (MRCP)[J]. J Magn Reson Imaging,2020,51(3):824-832. DOI: 10.1002/jmri.26863.
Figures