4490
3D Dynamic Magnetic Resonance Imaging: A Tool for Describing Velopharyngeal Function1East Carolina University, Greenville, NC, United States, 2Massachusetts General Hospital, Boston, MA, United States, 3University of Illinois Urbana-Champaign, Champaign,, IL, United States
Synopsis
Direct visualization of velopharyngeal structures and musculature during speech is best attained using 3D dynamic magnetic resonance imaging. Through innovative MR imaging and atlasing methods, we successfully describe velopharyngeal contours as represented on MR statistical atlases and individual subject images. Manual linear measurements of velum configurations during /p/ across two different speech stimuli reveal slight velar differences, reflecting major influences of neighboring speech sounds on velar movements.
Introduction
The production of speech is a dynamic process that involves many sudden and discrete movements. The velopharyngeal (VP) mechanism functions for closure between the oral and nasal cavities through lateral pharyngeal wall movement and superoposterior velar moment via contraction of the levator veli palatini muscle. Incomplete closure of VP structures may result in velopharyngeal insufficiency (VPI), characterized by hypernasality and poor speech intelligibility. Clinical imaging methods for assessing the function of the VP mechanism include nasendoscopy and videofluoroscopy. However, these methods are invasive and often not well tolerated by young children1-2.In this current work, we utilize a novel, child-friendly MR protocol, an innovative time-alignment method, and statistical MR atlases to observe and compare changes in velar movements and configurations of the high-pressure consonant /p/. Through the exploration of these methods to assess velar functioning, this work helps pave the way for the implementation of dynamic MRI and MR atlases in the diagnostic process of VPI as seen in children with cleft palate.
Methods
Dynamic speech images were gathered using a high-speed and high-resolution 3D MR sequence3. 4 healthy adult (2 male and 2 female) subjects underwent a 3D structural scan and 5 dynamic speech scans. Scans were obtained in less than 20 minutes resulting in 40960 reconstructed 3D images with 2x2x6 mm with 10 slice locations. Stimuli for /p/ included: “hamper” and “mom ‘n bob are happy.”All images were time-aligned according to novel procedures4. Data were imported into Amira 3D Visualization Modeling Software to manually obtain linear measurements related to VP functioning. Measurements included: velar length, velar thickness, retrovelar space, ABC angle, and alpha angle. Data from all subjects were analyzed and compared to the corresponding statistical atlas across subjects. Of interest was possible variability in velar movements and configurations when the high-pressure consonant /p/ was produced (1) after a nasal consonant and (2) after a vowel.
Results
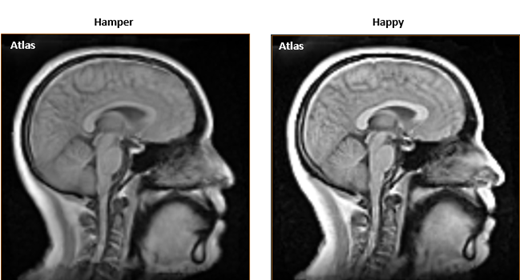
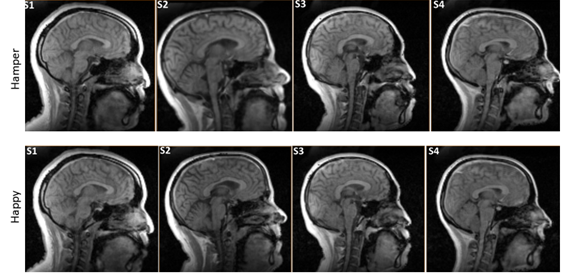
To explore the functionality and use of these methods, we describe average velar characteristics of /p/ as seen on the created atlases (Fig 1). Comparison of /p/ in the varying contexts revealed differences in velar configurations. The /p/ in “hamper” was produced with a longer and thinner velum than in “happy” creating a more pronounced velar knee, suggesting greater levator contraction2. Velar height, as measured by the ABC angle, also was greater when compared to the /p/ in “happy,” contributing to the increased velar flexion seen in “hamper.” The average alpha angle was 177°, indicating VP closure happened at or right below the palatal plane, as consistent with previous literature2. Of note was that the retrovelar space, the distance from the velar knee to the posterior pharyngeal wall, was 2.56 mm for /p/ in “hamper” and 3.44 mm for /p/ in “happy,” suggesting that complete velopharyngeal closure was not reconstructed on the atlas, although visibly present when viewing individual subject data.This work also aimed to provide validity to the use of atlases for demonstrating average VP movements by further analyzing individual subject data and comparing to the atlases. Figure 2 depicts velar configurations across contexts for all subjects. General trends of a longer and thinner velum to produce the /p/ in “hamper” remained consistent. ABC angle also remained greater for the /p/ in “hamper” across subjects. Subjects (except subject 3 in “hamper”) had a retrovelar space of 0 during the production of /p/ across contexts, indicating complete velopharyngeal closure. The varying points of contact on the posterior pharyngeal wall and the differences in pharyngeal depth across subjects likely contributed to the closure discrepancies seen in Figure 1.
Discussion
Dynamic imaging and temporal alignment methods of multiple subjects allow for the creation of atlases that can be utilized to make comprehensive observations and reliably assess VP functioning. The differences in velar configuration across /p/ contexts are likely a result of the co-articulatory patterns of the different speech stimuli. The longer and thinner velum seen in “hamper” may be a result of the needed quick and complete VP closure for /p/ after production of /m/, a nasal consonant produced with an open port. The closure force and levator contraction needed for /p/ after a nasal may also result in a more acute ABC angle. Research also indicates that low vowels, such as the vowel directly producing the /p/ in “happy”, are often produced with reduced velar height and closure force, likely leading to the velar configurations of /p/ noted in “happy.”5-7Of further interest is the noted VP opening for subject 3 in “hamper," likely a byproduct of the preceding nasal consonant that resulted in a weak pressured /p/ production. Future work will examine better ways to address the different points of VP closure on the pharyngeal wall within the atlases. We will also examine additional ways to assess velopharyngeal movements in order to best serve a clinical population.
Conclusion
By applying novel MR methods, we accurately described velar movements and compared individual subject data to the atlases, highlighting subject-specific deviations. This work shows great potential in utilizing MR models that capture and compare discrete speech movements, an innovative tool for assessing and characterizing velopharyngeal functioning.Acknowledgements
Research reported in this publication was supported by the National Institute of Dental & Craniofacial Research of the National Institutes of Health under Award Number R01DE027989. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.References
Ysunza PA, Repetto GM, Pamplona MC, et al. Current Controversies in Diagnosis and Management of Cleft Palate and Velopharyngeal Insufficiency. BioMed Research International. 2015;2015:196240-11.
Perry JL, Kuehn DP, Sutton BP, Fang X. Velopharyngeal Structural and Functional Assessment of Speech in Young Children Using Dynamic Magnetic Resonance Imaging. Cleft Palate Craniofac J. 2017;54(4):408-422.
Jin R, Liang ZP, Sutton BP. Increasing three-dimensional coverage of dynamic speech magnetic resonance imaging. Intl Soc Magn Reson Med, 2021, p 4175.
Xing F, Jin R, Gilbert IR, Perry JL, Sutton BP, Liu X, El Fakhri G, Shosted RK, & Woo J. 4D magnetic resonance imaging atlas construction using temporally aligned audio waveforms in speech. Journal of the Acoustical Society of America. 2021;150(1):3500-3508
Bell-Berti F, Krakow RA. Anticipatory velar lowering: A co-production account. Journal of the Acoustical Society of America. 1991;90(1):3500:112-123.
Moll KL. Velopharyngeal closure on vowels. Journal of Speech and Hearing Research.(1962);17:30–77.
Kuehn DP, Moon JB. Velopharyngeal closure force and levator veli palatini activation levels in varying phonetic contexts. Journal of Speech, Language, and Hearing Research. 1998;41, 51–62
Figures