4472
The influence of scanning order on whole-heart coronary MRA with multiple compressed sensing acceleration factors1Wuhan Asia general Hospital, WuHan HUBEI, China, 2Philips Healthcare,wuhan, WuHan HUBEI, China, 3Philips Healthcare,Beijing, Beijing, China
Synopsis
Compressed sensing (CS) is a novel magnetic resonance imaging technique to accelerate scanning under the premise of ensuring image quality. Whole-heart coronary MRA with CS technique can assess coronary artery lesions. However, the image quality is still sensitive to many factors. In this study, we demonstrated that there were statistical differences in parts of image quality with different scan orders when using CS AF of 6, where the scanning at the late stage of examinations showed high image quality. It might be the optimal choice to start coronary MRA scanning later in cardiac MRI practice.
Introduction
Coronary artery disease (CAD) is one of the main causes of human life-threatening in recent decades. Coronary artery angiography (CAG) is the "gold standard" for the diagnosis of CAD[1-2],and coronary CTA is widely used for CAD screening in clinical practice. However, they both have disadvantages of ionizing radiation and contrast agent allergy. Compressed sensing (CS) accelerated whole-heart coronary MRA (CMRA) is a non-invasive, contrast-free, and radiation-free technique that can assess coronary artery lesions. Multiple acceleration factors (AFs) can be selected in the coronary artery scan protocols. Acceleration factors (AF) of 2, 4, 6 are good options according to our preliminary experiment. This study was to investigate if the scan order of different MRI protocols could affect the image quality of CS CMRA with multiple AFs.Methods
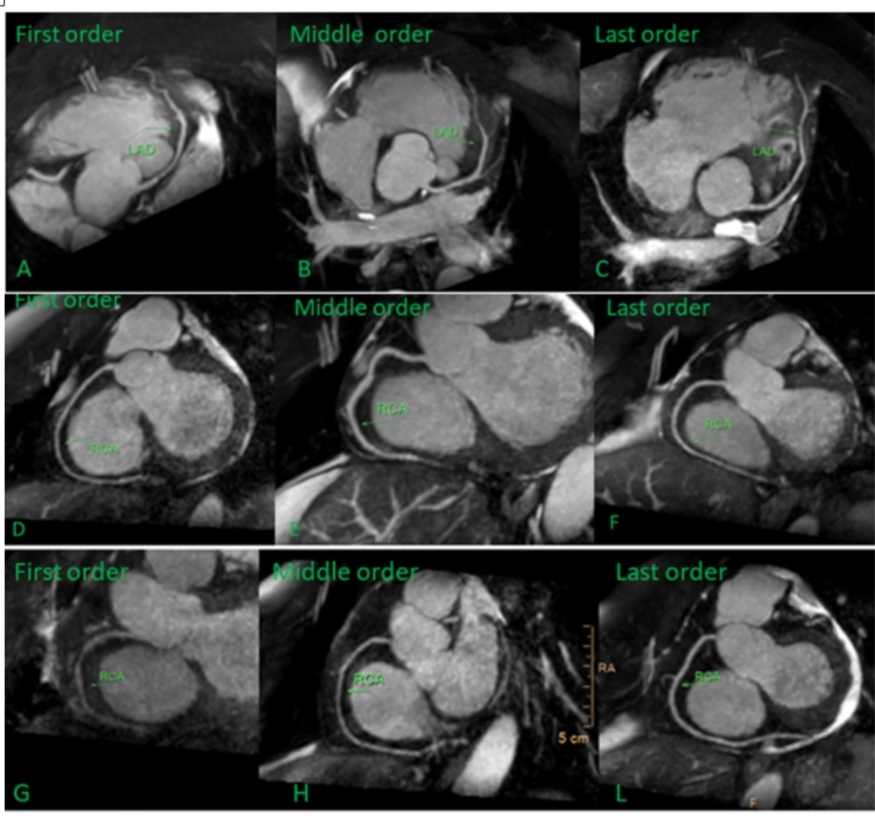
This study was approved by the institutional IRB. This study enrolled 232 patients , all patients underwent whole-heart coronary MRA on a 1.5T MR scanner a clinical 1.5T MR scanners (Ambition, Philips Healthcare, the Netherlands) with a 32-channel body coil. The whole-heart coronary MRA was based on a CS accelerated free-breathing electrocardiogram-triggered navigator-gated steady-state free precession sequence. For each patient, three CMRA protocols with CS AFs of 2, 4, and 6 were scanned with random orders. Therefore, the scanning orders of each protocol included first, middle, and last. Because the scanning duration of the CMRA protocol was related to the breathing and heartbeat rate of patients, the real scanning duration was recorded. We used a four-point subjective scale to score coronary image quality (1= poor, 2= medium, 3= good, 4= excellent) at nine branches of the coronary artery, including left main coronary artery (LM), left anterior descending coronary (LAD), left circumflex artery (LCX), posterior descending artery (RCA) at proximal (index 1), middle/distal (index 2), distal (index 3) positions. Three radiologists evaluated the image quality by subjective scores independently. The scanning time and image quality with different scanning orders were compared using the Kruskal-Wallis H test.Results
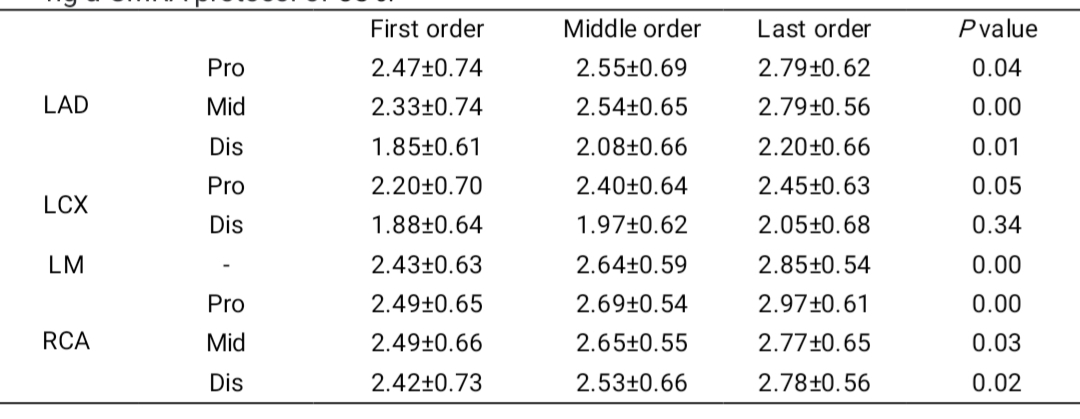
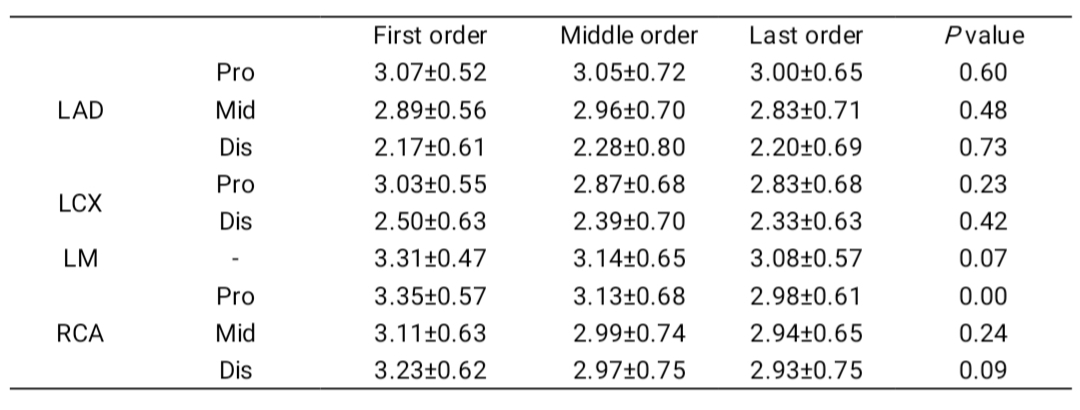
There was a statistical difference in protocol with CS AF of 6 among scanning with different scanning orders in LM, middle LAD, and proximal RCA image quality (P < 0.05) (shown in table 1). Images with the last scanning order showed the highest image quality. There was no statistical significance in CS2 and CS4 with different orders in all branch segments (P > 0.05), except proximal RCA (table 2 and 3). There was a statistical significance in CS AF of 6 with different scanning orders in scanning time (P < 0.05, table 4), where patients with the last scanning order took medium scanning time, while there was no statistical difference in scanning time among protocols with different scanning orders when CS AFs were 2 and 4 (P > 0.05, table 4).Discussion
Due to the shorter scanning time of CS 6, the image quality may be more susceptible to heart rate, heart rhythm, the respiratory rhythm of patients. Scanning at the late stage of CMR examinations could give patients more time to adjust their respiratory and emotion before the coronary MRA scan.Conclusion
In conclusion, this study demonstrated that the scanning order of different protocols during CMR examinations would affect image quality in coronary MRA with CS AFs of 6. It might be the optimal choice to start coronary MRA scanning later in cardiac MRI application.Acknowledgements
On this occasion there is no one we wish to acknowledge.References
1. Masashi Nakamuraa, Tomoyuki Kidoa, Teruhito Kidoa, Kouki Watanabe, et al. Non-contrast compressed sensing whole-heart coronary magnetic resonance angiography at 3T: A comparison with conventional imaging. European Journal of Radiology 104 (2018) 43–48.
2.Akcakaya M, Basha TA, Chan RH, et al. Accelerated Isotropic Sub-Millimeter Whole-Heart Coronary MRI: Compressed Sensing Versus Parallel Imaging. Magn Reson Med. 2014.
Figures