4470
Wall Enhancement of Unruptured Intracranial Aneurysm on MR Imaging is Associated with Irregular Pulsation Detected by Four-dimensional CTA1Ren Ji Hospital, Shanghai Jiao Tong University School of Medicine, shanghai, China, 2University of Washington, Seattle, WA, United States
Synopsis
Both aneurysm wall enhancement (AWE) and irregular pulsation have been suggested as potential candidates for intracranial aneurysms (IAs) instability. No studies have explored the association between AWE and irregular pulsation. By using vessel wall MRI and four-dimensional computed tomography angiography, we found a significantly strong correlation between AWE and irregular pulsation (phi coefficient=0.569, p<0.001). IAs with irregular pulsation had much less AWE grade 0 and more AWE grade 1, 2 and 3 compared with IAs without irregular pulsation (all p<0.05). Further longitudinal studies are needed to validate the role of the two imaging markers in predicting aneurysm growth and rupture.
METHODS This retrospective study included consecutive patients with IAs who underwent 4D-CTA and VW-MRI between January 2017 to July 2021. 4D-CTA was performed on a 320-detector row CT scanner (Aquilion ONE VISION, Canon Medical System Corporation, Otawara, Japan). Vessel wall MRI was performed on a 3.0T MR scanner (Prisma, Siemens Healthcare or Ingenia, Philips Healthcare or Prisma). The imaging protocols for MR scanning on Ingenia and Prisma were as follows respectively: 1) T1WI volume isotropic turbo spin-echo acquisition (T1-VISTA) sequence with following parameters: TR/TE 800/20msec, number of slices 80, field of view 250mm×162mm, voxel size 0.6mm×0.6mm×0.6mm, acquisition matrix 416×269, and scan time 5 minutes 2 seconds. 2) T1-weighted 3D black-blood fast spin echo with variable flip angle trains (SPACE) sequence with following parameters: TR/TE 1000/15msec, number of slices 240, field of view 193mm× 193mm, voxel size 0.6mm× 0.6mm× 0.6 mm, acquisition matrix 320× 320, and scan time 9 minutes 13 seconds. Post-contrast VW-MRI sequence was acquired 5 minutes after Gadolinium-based contrast agent (Magnevist, Bayer Healthcare, Berlin, German) injection (with a dose of 0.1 mmol/kg, at a rate of 1.5ml/s). Geometric and morphologic parameters were measured and the presence of irregular pulsation (defined as a temporary focal protuberance ≥1 mm on more than three successive frames) was identified on 4D-CTA movies6. AWE was estimated on VW-MRI and classified as 4 grades (grade 0 for none or questionable focal trace enhancement, grade 1 for focal thick [<1mm] enhancement, grade 2 for thin [maximum thickness, ≤1 mm] circumferential wall enhancement, or grade 3 for thick [maximum thickness, ≥1 mm] circumferential wall enhancement)7. The association between AWE and irregular pulsation was analyzed.
RESULTS One hundred and fifty-three patients with 176 saccular IAs were included in this study. Irregular pulsation was observed in 35.8% (63/176) of IAs. Among 176 aneurysms, 64 (36.4%) were enhancing; 23(13.1%) were grade 1, 26 (14.8%) were grade 2, and 15 (8.5%) were grade 3. Larger size, aspect ratio and irregular shape were positively associated with irregular pulsation (p < 0.05). IAs with irregular pulsation had much less AWE grade 0 (27.0% versus 84.1%, p<0.05) and more AWE grade 1, 2 and 3 (25.4%, 30.2% and 17.5%, respectively) compared with IAs without irregular pulsation (6.2%, 6.2% and 3.5%, respectively) (all p<0.05). There was a significantly strong correlation between AWE and irregular pulsation (phi coefficient=0.569, p<0.001).
DISCUSSION Recent studies have showed AWE was promising for identification of unstable aneurysms and it is gaining increasing attention7,8. This study demonstrated a strong positive correlation between AWE and irregular pulsation, indicating that irregular pulsation might have the same potential for predicting aneurysm rupture risk. Wall enhancement possibly indicates vasa vasorum which is an indirect marker of inflammation9. Persistent inflammation of aneurysm wall involves increased elastic lamina breakdown and may thereby cause focal weakening of the wall, perhaps explaining the formation of irregular pulsation. Further research is still needed, however, to study the association between irregular pulsation and AWE, wall thinning and inflammation. We think irregular pulsation and AWE might be two different concepts of the aneurysm instability, but should be mutually complementary. We are currently running a prospective study and scanning patients with both 4D CTA and black blood MRI, and we hope such multi-modality imaging study will help determine the best predictors of aneurysm instability.
CONCLUSION The strong correlation between AWE and irregular pulsation further confirmed the important role of irregular pulsation in predicting aneurysm instability. These two imaging markers should be validated in future longitudinal studies for their values in predicting aneurysm growth and rupture.
Acknowledgements
NoneReferences
1. Hackenberg K, Hanggi D, Etminan N. Unruptured Intracranial Aneurysms. Stroke 2018;49(9):2268-2275.
2. Fu Q, Wang Y, Zhang Y et al. Qualitative and Quantitative Wall Enhancement on Magnetic Resonance Imaging Is Associated With Symptoms of Unruptured Intracranial Aneurysms. Stroke 2021;52(1):213-222.
3. Sanchez VKM, Greving JP, Kuroda S et al. External Validation of the ELAPSS Score for Prediction of Unruptured Intracranial Aneurysm Growth Risk. J Stroke 2019;21(3):340-346.
4. Shimonaga K, Matsushige T, Ishii D et al. Clinicopathological Insights From Vessel Wall Imaging of Unruptured Intracranial Aneurysms. Stroke 2018;49(10):2516-2519.
5. Vanrossomme AE, Eker OF, Thiran JP et al. Intracranial Aneurysms: Wall Motion Analysis for Prediction of Rupture. AJNR Am J Neuroradiol 2015;36(10):1796-802.
6. Zhang J, Li X, Zhao B et al. Irregular pulsation of intracranial unruptured aneurysm detected by four-dimensional CT angiography is associated with increased estimated rupture risk and conventional risk factors. J Neurointerv Surg 2021;13(9):854-859.
7. Edjlali M, Guedon A, Ben HW et al. Circumferential Thick Enhancement at Vessel Wall MRI Has High Specificity for Intracranial Aneurysm Instability. Radiology 2018;289(1):181-187.
8. Zhu C, Wang X, Eisenmenger L et al. Wall enhancement on black-blood MRI is independently associated with symptomatic status of unruptured intracranial saccular aneurysm. Eur Radiol 2020;30(12):6413-6420.
9. Quan K, Song J, Yang Z et al. Validation of Wall Enhancement as a New Imaging Biomarker of Unruptured Cerebral Aneurysm. Stroke 2019;50(6):1570-1573.
Figures
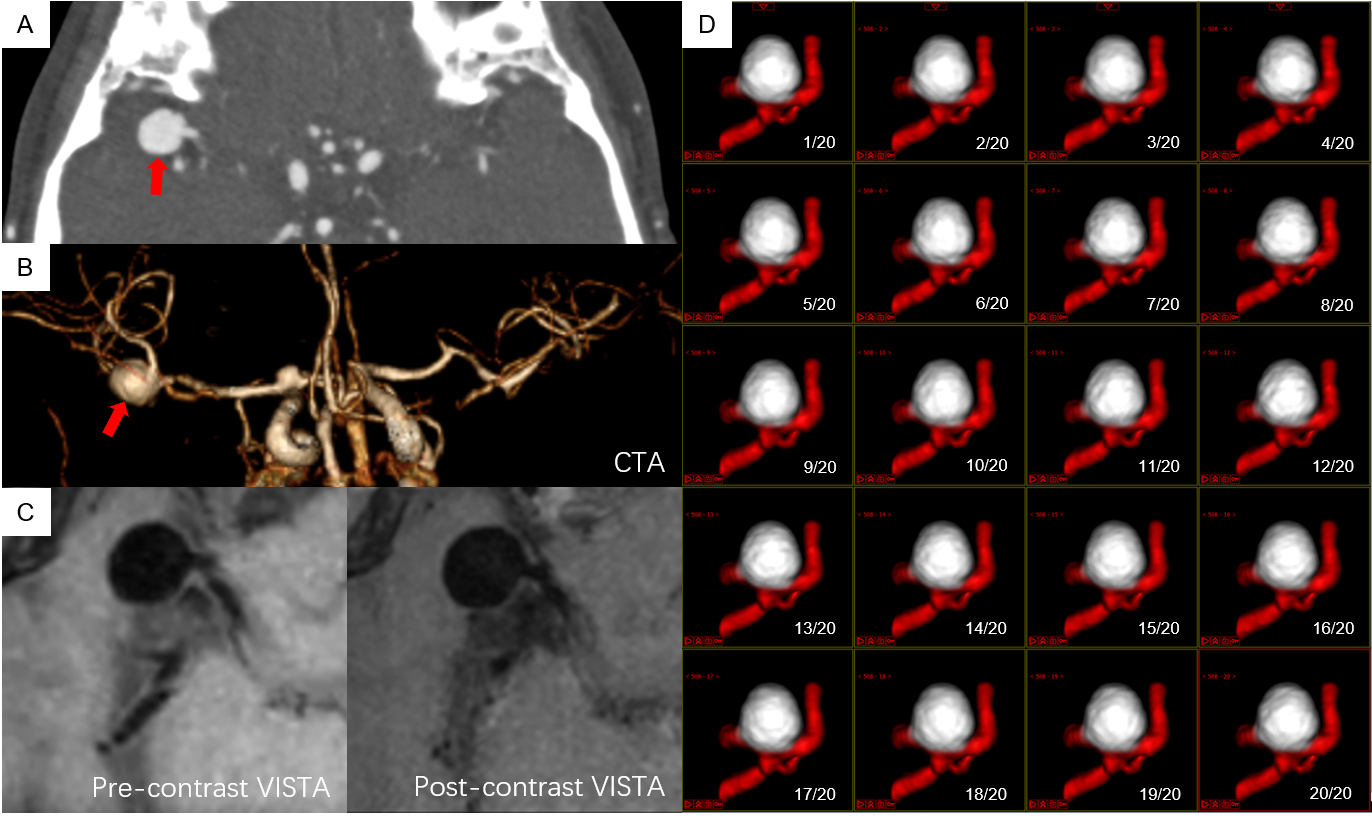
Figure 1. A patient with a right middle cerebral artery aneurysm (size: 9.4mm, height: 9.1mm, neck width:3.5mm). CTA MIP (A), 3D CTA (B), pre-contrast vessel wall image and postcontrast vessel wall image (C) show a right middle cerebral artery aneurysm with enhancement grade 0. 4D-CTA (D) shows no irregular pulsation in the aneurysm.
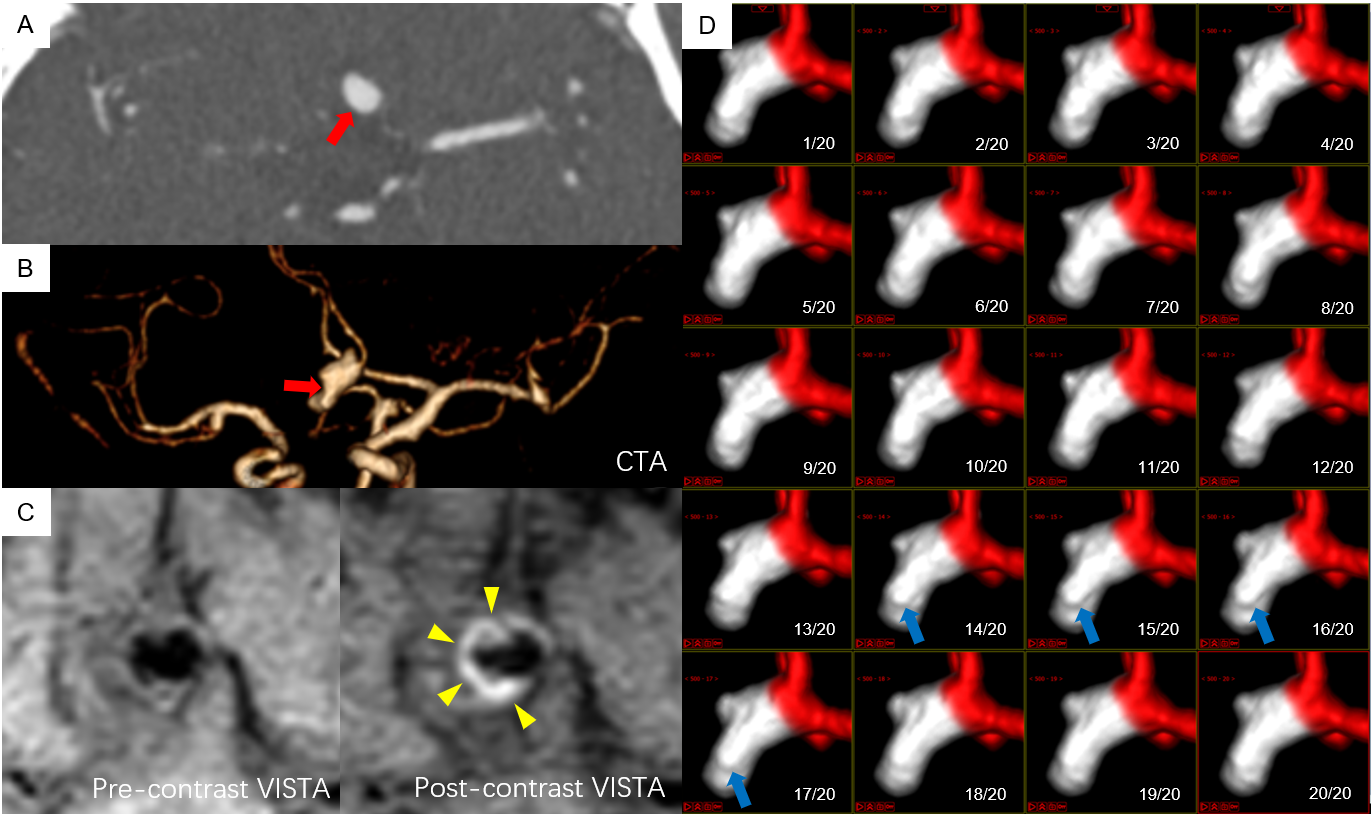
Figure 2. A patient with an anterior communicating artery aneurysm (size: 13.1mm, height: 6.9mm, neck width:4.1mm). CTA MIP (A), 3D CTA (B), pre-contrast vessel wall image and postcontrast vessel wall image (C) show an anterior communicating artery aneurysm with irregular shape and enhancement grade 3. An elevation (irregular pulsation) at the body of the aneurysm is observed in the 13th to 17th frames of 4D-CTA (D, blue arrow). The maximum perpendicular height of the protuberance was 1.52mm.
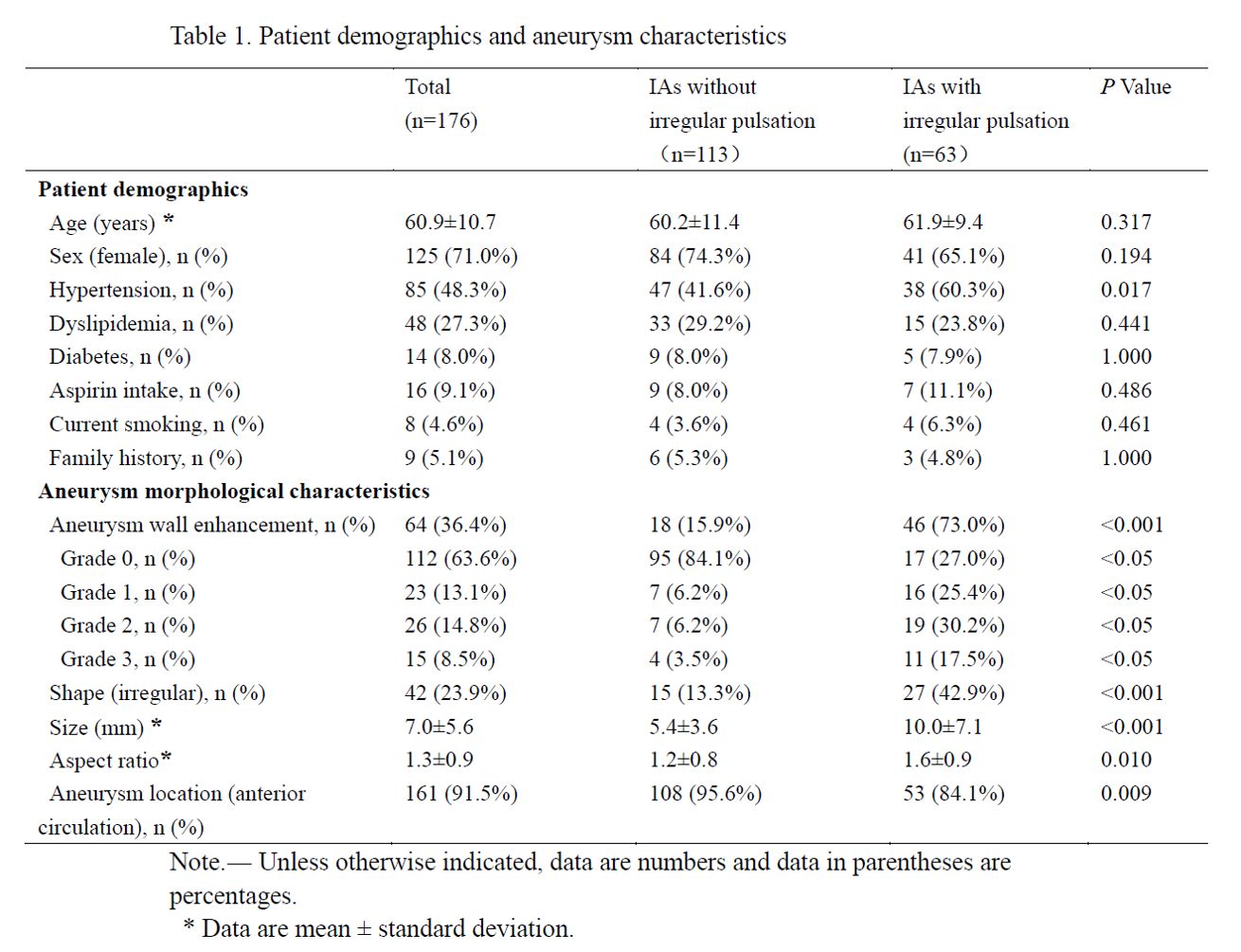
Figure 3. Patient demographics and aneurysm characteristics